Frequently asked Brucella canis testing questions
Published 1 September 2023

© Crown copyright 2023
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/brucella-canis-testing-faq/frequently-asked-brucella-canis-testing-questions
1. What tests should I select for screening or diagnostic testing?
We recommend that serum samples are submitted to APHA Weybridge for serological testing. The tests we recommend are Brucella canis SAT (Serum Agglutination Test) (TC1032) and Brucella canis iELISA (indirect Enzyme Linked Immunosorbent Assay) (TC0116). If either test is positive, then the sample is considered serologically positive. If both tests are negative, then the sample is considered serologically negative. This approach gives an estimated diagnostic sensitivity and specificity of approximately 92% (95% Confidence Interval = 83.9% to 97.6%) and 99% (95% Confidence Interval = 96.0% to 99.7%) respectively. The Positive Predictive Value (PPV) for this approach is show at the bottom of this document.
2. Why are two test types recommended to be used together for serology?
The two tests work well together as the SAT is more sensitive to IgM (Immunoglobulin M) antibodies, which are more abundant during early stages of infection, and the iELISA detects IgG (Immunoglobulin G) antibodies which are more abundant after the early stages of infection and during chronic infection. This combination gives good coverage for detection of disease from early to late/chronic stages of infection.
3. Are there alternatives to serology?
Whole blood samples for bacterial culture can be sent when there is a high clinical suspicion of disease (especially if there is also a high risk of onwards transmission of disease) or for contact dogs (especially those where transmission may have been recent). This test is not appropriate for routine screening. Please contact the Brucella Group email address (BrucellaGroup@apha.gov.uk) prior to taking and submitting such samples.
4. How does serology and bacterial culture from whole blood for B. canis compare?
The diagnostic sensitivity of bacteriology (and PCR), as undertaken from readily available clinical samples such as blood, is low as the presence of bacteria in the blood can be short lived or intermittent. Many infected animals would be missed by sole reliance on this approach. Serology is more diagnostically sensitive but has imperfect diagnostic specificity and so some false positive test results can occur. The probability that a seropositive result is a true positive (i.e. the dog is truly infected) depends on the diagnostic specificity of the test (or combination of tests) and the prevalence of disease in the population of dogs the sampled dog is a member of. The higher the prevalence of disease in that population, the higher the probability that the positive result is a true positive. Unfortunately, the prevalence of disease in the UK and in countries from which dogs are imported is not currently known. However, the higher the number of risk factors and the severity of these for the dog in question, the more reasonable it is to consider that it is a member of a population with a higher disease prevalence. In some cases there may be few risk factors (or these may be of low severity) in which case it may be appropriate to retest the dog one or more months after the initial sampling. We recommend that if this is the path followed, the animal is isolated from other dogs during this period.
5. What type of sample should I send?
Samples for serology should be a non-heparinised blood sample (or other means of serum separation) and a minimum of 1 ml of blood. The assays have not been validated for plasma therefore gel-based separation tubes should be of the type that separate serum rather than plasma. Whole blood samples containing anticoagulant are also unsuitable for serology.
Samples for blood culture should be a 1ml whole-blood sample collected with an anticoagulant. Sodium citrate anticoagulant tubes should be used as they provide better sensitivity compared to EDTA (ethylenediaminetetraacetic acid), which is inhibitory. Other samples can be submitted, such as swabs and tissues, but this should be discussed with the laboratory prior to sending using the Brucella Group email address above.
6. How do I submit samples for serology?
These can be sent directly to the APHA as per sample submission form LSW008. The general submission form can be found using this link (LSW008).
7. How do I submit samples for culture (whole blood/swab/tissue)?
Email BrucellaGroup@apha.gov.uk prior to submission.
Samples can be sent with the serology samples using form LSW008 and add a description in the note section of the APHA submission form (top of page 2), culture samples for Brucella reference laboratory.
Results from Brucella culture may take up to 14 working days for blood samples and longer for tissues samples.
8. How do I package and send samples?
All diagnostic samples should be packaged and dispatched in accordance with UN3373 packing regulations. Failure to comply with this requirement may result in the sample being destroyed to avoid further infection risk.
See the following link for information on how to submit samples to APHA APHA Scientific Tests (vla.gov.uk)
9. Where can I find the prices, turnaround times and sample types for B. canis serology?
Please find link to the requested information APHA Scientific Tests (vla.gov.uk).
10. How does test B. canis SAT (TC1032) work?
The B. canis SAT (Serum Agglutination Test) detects mainly IgM antibodies and the result of the test represents the degree to which any antibodies in the serum are able to agglutinate B. canis antigen (agglutination indicates the presence of anti-B. canis antibodies). The result is expressed as the agglutination score at the highest dilution of the sample in which agglutination occurred. The agglutination score is marked from 0 (no agglutination) to 4 (complete agglutination). The starting dilution of the serum is 1/25 and increases in doubling dilutions (1/50, 1/100, 1/200, etc). The result is presented in a format that looks like a fraction (although it is not) with the agglutination score shown as the ‘numerator’ and the highest dilution at which agglutination occurred shown as the ‘denominator’. The titre of the sample increases in the following order: <1/25, 1/25, 2/25, 3/25, 4/25, 1/50, 2/50, 3/50, 4/50, 1/100, 2/100, 3/100, 4/100, 1/200, etc. Samples that give results from <1/25 to 1/50 are considered negative. Samples that give results of 2/50 or more are considered positive. The higher the titre, the greater the content of B. canis agglutinating antibodies in the serum sample.
11. How does the B. canis iELISA (TC0116) work?
The B. canis iELISA (indirect Enzyme Linked Immunosorbent Assay) detects IgG antibodies and the result is expressed as a percentage of the strong positive control (S/P ratio). The test cut-off for this ELISA is 1.47, all S/P ratios below this value are considered negative and all S/P ratios equivalent or above this value are considered positive. The higher the S/P ratio the more antibodies are present in the sample. The iELISA average result from dogs considered infected is approximately 3.0 and the range is from 0.85 (this dog was confirmed infected by culture and SAT positive) to 4.6.
12. What to do in the event of a positive result?
Please find the link below to the APHA “Canine Brucellosis: Summary sheet for veterinary staff”. This contains useful information about the disease to help inform actions in the event of a Brucella canis case or a positive Brucella canis result. A link to this information can be found on the APHA Vet Gateway Disease Information page Disease Information (defra.gov.uk).
13. Do you have a contact I can discuss this result with?
14. Should I be selecting the B. canis RSA test?
The APHA also offer the RSA (Rapid Slide Agglutination) serology test. This is similar in principle to the SAT as it is also an agglutination assay that is also sensitive to IgM, but is inferior to the SAT for diagnostic purposes. It is sometimes used for pre-export testing of dogs if required by a specific country and so still appears on the APHA sample submission form. If it is possible to test by SAT and iELISA (as described above), the APHA would recommend this choice if testing for diagnostic/screening reasons.
The RSA can be performed within minutes once the sample reaches the testing laboratory if there is an urgent need. It is a qualitative test only and the diagnostic specificity is lower than the SAT and the iELISA (and sensitivity is also lower than iELISA). It may have a purpose when a rapid result is required – for example when it is important to have some information with respect to the infection status of a dog when there has been a potential high risk human exposure event (the potential being dependent on the infection status of the dog) and some health intervention may be required. Even if RSA is completed, SAT and iELISA should also be done on each sample and the sample interpretation based on the SAT and iELISA results as described above. If the RSA result and combined SAT and iELISA result is discordant please refer to the APHA Brucella Reference Laboratory for specific advice using the Brucella Group email address above (as interpretation may depend on other case circumstances).
15. Do APHA provide a PCR test?
The APHA do not provide a commercial PCR test for the detection of Brucella DNA from clinical samples (for example blood) because there have not been enough suitable samples from which to robustly validate the diagnostic sensitivity and specificity of this approach. We are aware that PCR is available commercially elsewhere but have not been able to find a provider that can provide validation data for their method. As with Brucella culture from blood we do not believe that PCR is sufficiently sensitive for screening or diagnosis but will always consider good quality data if it becomes available.
16. How should I report a positive result?
The detection of Brucella canis (B. canis) (including positive serology) is Reportable under 2021 amendments to the Zoonoses Order (1989) that were made in Great Britain in early 2021, and with this is a legal obligation for the submitting laboratory or veterinary practice to provide statutory data for the case to the APHA for dogs living in Great Britain. Where the tests have been performed at APHA, there is no need to report the result to the APHA, although the obligation to provide all the statutory information must still be fulfilled if not submitted with the material for testing. The APHA will request any missing statutory information from the customer that submitted the sample(s) when issuing positive results. Where testing has not been done by APHA, the legal requirement to report results and the necessary statutory information still exists and this applies to mobile tests such as, but not limited to, lateral flow tests. It is also a legal requirement to supply diagnostic material to APHA upon request. Reports can be made to: brucellagroup@apha.gov.uk.
17. Test Interpretation
The following test metrics should be considered before and after testing: Important metrics to consider before and after testing:
- Diagnostic sensitivity (DSn [or sometimes DSe]): Percentage of known infected animals that test positive in the assay; infected animals that test negative are considered to have false- negative results
- Diagnostic specificity (DSp): Percentage of known uninfected animals that test negative in the assay; uninfected animals that test positive are considered to have false positive results
- Analytical sensitivity: the ability of an assay to detect a specific analyte within a matrix (sometimes expressed as the lowest limit of detection and often determined with spiked samples)
- Analytical specificity (or Exclusivity): the ability of the assay to detect an analyte that is unique to a targeted organism
- Positive Predictive Value (PPV): The probability that an animal that has tested positive is infected with the disease being tested for
- Negative Predictive Value (NPV): The probability that an animal that has tested negative is not infected with the disease being tested for
The Predictive Values are influenced by the true prevalence of the disease in the target population and are a function of this and the DSn and DSp values. For example, the PPV will be higher when the prevalence of the disease is higher and the PPV will be lower (there will be more false positive results) when the prevalence of the disease is lower.
The PPV for the APHA recommended serological testing algorithm (alongside those for the individual tests) against a range of hypothetical disease prevalence values is shown in the figure below.
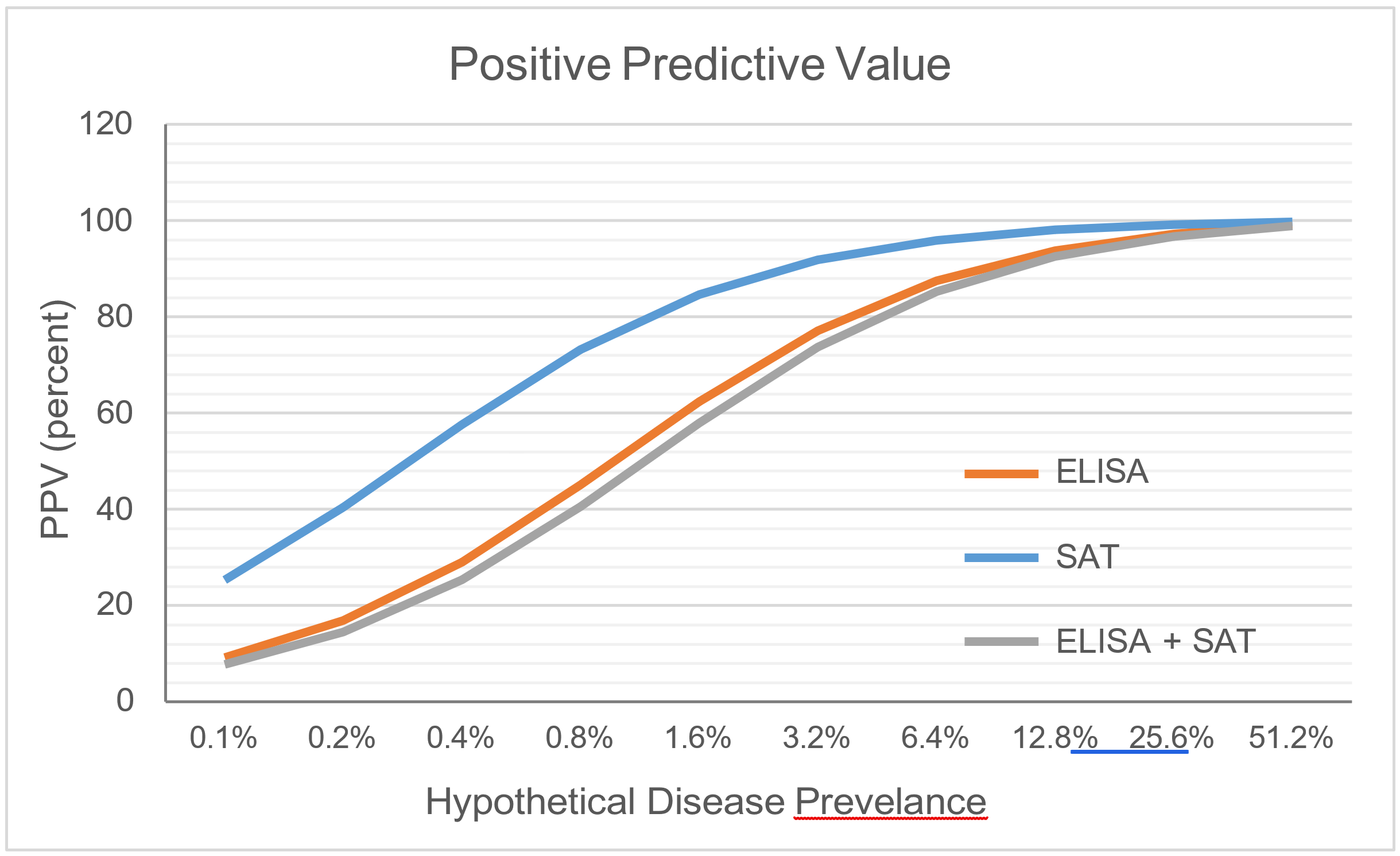{kind=link}
For iELISA only DSp = 99.1%, 95% Confidence interval: 96.8% - 99.9%, DSn = 89.6%, 95% Confidence interval: 80.8% - 94.6%. For SAT only DSp = 99.8%, 95% Confidence interval: 99.2% - 99.97%, DSn = 71.1%, 95% Confidence interval = 61.3% - 79.5%.
The APHA aims to update the validation data for its tests when new material becomes available to make this possible. Therefore, the exact DSp and DSn values may change over time. The values listed in the current online version of this document describe the most up to date information.
For a useful guide for information about these values refer to the WOAH Manual of Diagnostic Tests and Vaccines for Terrestrial Animals, Chapter 1.1.6 (noting that brucellosis due to Brucella canis infection is itself not covered by WOAH, although the principles for the test metrics above still apply)