Common animal-associated infections (England): first quarter 2024
Updated 31 October 2024
Applies to England

© Crown copyright 2024
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/common-animal-associated-infections-2024/common-animal-associated-infections-england-first-quarter-2024
Background
This quarterly report is produced by the Emerging Infections and Zoonoses team in the Travel Health, Zoonosis, Emerging Infections, Respiratory and TB Division, Clinical and Emerging Infections Directorate, UK Health Security Agency (UKHSA). As of 2023, the data presented in these reports is for England only. Data for Wales will be reported separately by Public Health Wales. Previous reports presenting data for both England and Wales can be found elsewhere on the GOV.UK website.
The report summarises laboratory-diagnosed cases of selected zoonoses reported in England between January and March 2024 (first quarter) and includes additional information on the quarterly trends for hepatitis E, leptospirosis, Lyme disease, toxoplasmosis and psittacosis.
It is important to note that not all cases of a zoonotic infection will present to healthcare services, and some cases may be treated empirically based on clinical suspicion without the need for a confirmatory test. Therefore, the numbers in this report are expected to be an underestimate of the true burden of zoonotic disease in England, likely biasing towards severe infections as individuals with severe or symptomatic disease may be more likely to be tested. Furthermore, not all zoonoses presented in this report are notifiable in England. As such, it is likely not all confirmed laboratory test results are reported to UKHSA. For a list of notifiable diseases and causative organisms in England see the Notifiable diseases and causative organisms: how to report webpage.
The impacts of the public health measures implemented in England due to the COVID-19 pandemic during 2020 and 2021 should be considered when making comparisons with this time period.
Data reported as provisional is subject to change due to late notifications and de-duplication. Therefore, the data presented in this report supersedes data in previous reports.
The regional data presented is based on the location of the patient postcode where available. If patient postcode is not available, then location of the referring hospital or laboratory is used. This means the regional data presented does not necessarily reflect the geographic area where the cases are located or the infection is acquired.
Q-fever data is not presented in this quarterly report. As part of an internal review, the data is being validated and will be published as soon as possible.
Overview
Table 1. Animal-associated infections in England: quarterly confirmed laboratory reports by specimen date Q1 2022 to Q1 2024
| Disease (Organism) | Q1 2022 | Q2 2022 | Q3 2022 | Q4 2022 | Total 2022 | Q1 2023 | Q2 2023 | Q3 2023 | Q4 2023 | Total 2023 | Q1 2024* |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Anthrax (Bacillus anthracis) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Brucellosis (Brucella spp.) ** | 1 | 3 | 4 | 5 | 13 | 2 | 7 | 9 | – | – | – |
| Hepatitis E | 322 | 397 | 343 | 457 | 1,519 | 378 | 384 | 409 | 355 | 1,526 | 350 |
| Leptospirosis (Leptospira spp.) | 4 | 10 | 26 | 12 | 52 | 5 | 8 | 34 | 23 | 70 | 15 |
| Lyme disease (Borrelia burgdorferi) | |||||||||||
| All cases | 157 | 243 | 577 | 269 | 1,246 | 158 | 253 | 908 | 351 | 1,670 | 192 |
| Acute infections | 101 | 192 | 441 | 182 | 916 | 87 | 183 | 704 | 180 | 1,154 | 77 |
| Pasteurellosis (Pasteurella spp.) | 173 | 214 | 230 | 184 | 801 | 151 | 222 | 255 | 187 | 815 | 219 |
| Psittacosis (C. psittaci / C. abortus) | 0 | 0 | 0 | 0 | 0 | 3 | 0 | 1 | 1 | 5 | 2 |
| Toxoplasmosis (Toxoplasma gondii)† | 54 | 37 | 57 | 45 | 193 | 63 | 54 | 56 | 55 | 228 | 48 |
*Provisional data.
**Data has not been included in this report since Quarter 3 2023 due to an ongoing review of recent results in collaboration with the reference laboratory. This data will be published once this review is complete.
† Based on date specimen received.
Hepatitis E
The national hepatitis E virus (HEV) surveillance reports reference laboratory data (Public Health Laboratory Birmingham and the UKHSA Blood Borne Virus Unit Colindale) together with additional cases reported by local laboratories through the Second Generation Surveillance System (SGSS). The combined data sets provide a more accurate reflection of the number of acute HEV cases reported in England.
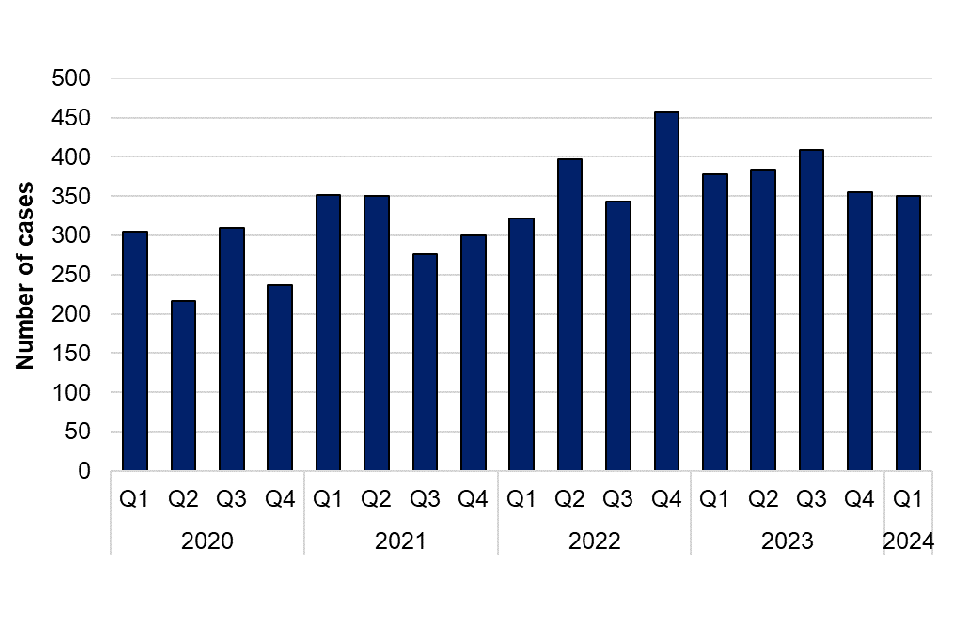
There were 350 laboratory-reported cases of HEV infection in the first quarter of 2024 compared with 378 in the same quarter of 2023. Figure 1 shows the number of HEV infections by quarter between 2020 and 2024. The greatest number of laboratory reported HEV cases were in quarter 4 of 2022; since then, the number of cases has decreased. The number of cases varies each quarter with no distinct seasonal pattern.
Figure 1. Laboratory-confirmed cases of hepatitis E in England by quarter, Q1 2020 to Q1 2024
Of the 350 cases reported in the first quarter of 2024, 193 (55%) were male (aged 4 to 91 years, median 57 years) and 157 (45%) were female (aged 6 to 95 years, median 57 years) (Table 2). There is a persisting predominance of middle aged and older men (aged 45 years and over).
Table 2. Laboratory-confirmed cases of hepatitis E in England by age group and sex, Q1 2024
| Age group | Male | Female | Total |
|---|---|---|---|
| 0 to 14 | 2 | 1 | 3 |
| 15 to 24 | 11 | 10 | 21 |
| 25 to 44 | 44 | 38 | 82 |
| 45 to 64 | 63 | 59 | 122 |
| Over 64 | 73 | 49 | 122 |
| Total | 193 | 157 | 350 |
Leptospirosis
Data for leptospirosis was obtained from the Rare and Imported Pathogens Laboratory (RIPL, UKHSA Porton). As of 1 August 2020, a laboratory-confirmed case of leptospirosis is defined by a positive 16S ribosomal ribonucleic acid (rRNA) polymerase chain reaction (PCR) result only. An Immunoglobulin M (IgM) enzyme-linked immunoabsorbent assay (EIA) continues to be performed on all samples of suspected leptospirosis cases. A case with a positive leptospirosis IgM result will usually be treated clinically on the basis of this result, even in the absence of a positive PCR result. A case with a positive IgM but without a confirmatory PCR result is therefore reported as a probable case for surveillance purposes. National surveillance of probable cases of leptospirosis was introduced in 2021.
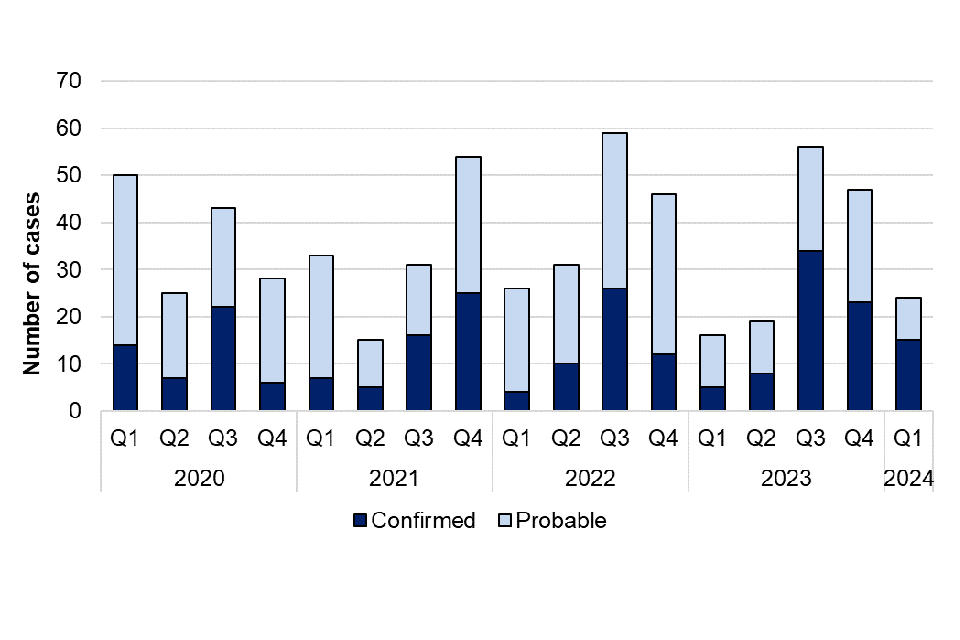
There were 15 confirmed cases and 9 probable cases of leptospirosis reported in the first quarter of 2024, compared with 5 confirmed and 11 probable cases reported in the same quarter of 2023. Figure 2 shows the number of confirmed and probable cases reported by quarter over the past 5 years (2020 to 2024).
Figure 2. Laboratory-confirmed cases of leptospirosis in England by quarter, Q1 2020 to Q1 2024
In the first quarter of 2024, 13 (87%) confirmed cases were male (aged 25 to 58 years, median 44 years) and 2 (13%) were female (median 38 years). Based on patient postcode, or reporting laboratory location where patient postcode was missing, cases were reported in the South East (n=4), South West (n=3), North East (n=2), East of England (n=2), East Midlands (n=1), Yorkshire and Humber (n=1), West Midlands (n=1), and the London region (n=1).
Table 3. Laboratory-confirmed cases of leptospirosis in England by age group and sex, Q1 2024
| Age group | Male | Female | Total |
|---|---|---|---|
| 0 to 14 | 0 | 0 | 0 |
| 15 to 24 | 0 | 0 | 0 |
| 25 to 44 | 7 | 1 | 8 |
| 45 to 64 | 6 | 1 | 7 |
| Over 64 | 0 | 0 | 0 |
| Total | 13 | 2 | 15 |
Travel history is not always available for all laboratory diagnosed cases and the reported country of recent travel does not necessarily reflect where the infection was acquired. Of the confirmed cases, 6 reported recent travel abroad. These included to Southeast Asia (n=1), South Asia (n=2), South America (n=1), and the Caribbean (n=2).
Of the 15 confirmed cases, 3 reported potential exposure to a water source, 1 reported swimming in a waterfall, 1 reported ingesting water from a waterfall and 1 exposure was unspecified. Two confirmed cases reported potential exposures linked to rats.
Lyme disease
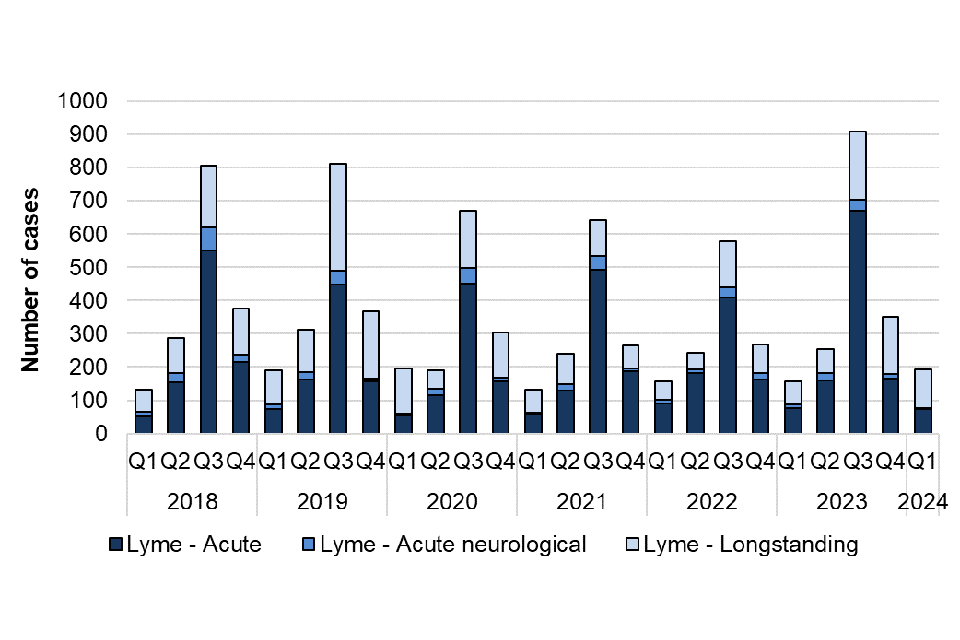
Data for Lyme disease was obtained from the Rare and Imported Pathogens Laboratory (RIPL, UKHSA Porton). The total number of confirmed Lyme disease cases reported in the first quarter of 2024 (n=192) was higher than in the same time period in 2023 (n=158), however the total number of acute cases reported was lower in the first quarter of 2024 (n=77) compared to the same period in 2023 (n=87). The recent number of cases reported are similar to data reported in 2018/2019, prior to a decrease in cases during COVID-19 when there was a decrease in laboratory confirmed cases, possibly due to cases being treated without being tested. It should be noted that diagnosis for acute Lyme disease presenting with erythema migrans (“bullseye rash”) is made clinically and testing is not recommended, as per NICE guidelines. The number of laboratory-confirmed cases presented in this report are therefore likely an underestimate of the true burden of acute Lyme disease in England.
Figure 3 shows how the number of cases continues to peak during the summer months (third quarter), which corresponds to the peak period of exposure to ticks in the UK, the spring and summer months.
Figure 3. Laboratory-confirmed cases of Lyme disease in England by quarter, Q1 2018 to Q4 2024
Of the total cases reported in the first quarter, 77 (40%) were acute (including 3 with neurological Lyme disease) and 115 (60%) were longstanding. Of the acute cases, 37 (48%) were male (aged 7 to 77 years, median 46 years), 39 (51%) were female (aged 11 to 76 years, median 48 years) and 1 case was of unknown. Table 4 shows the age group and sex distribution of acute cases.
Table 4. Laboratory-confirmed acute cases of Lyme disease in England by age group and sex, Q1 2024
| Age group (years) | Male | Female | Unknown | Total |
|---|---|---|---|---|
| 0 to 14 | 2 | 1 | 0 | 3 |
| 15 to 24 | 2 | 2 | 0 | 4 |
| 25 to 34 | 8 | 6 | 0 | 14 |
| 35 to 44 | 6 | 10 | 1 | 17 |
| 45 to 54 | 7 | 6 | 0 | 13 |
| 55 to 64 | 7 | 9 | 0 | 16 |
| 65 to 74 | 3 | 3 | 0 | 6 |
| Over 74 | 2 | 2 | 0 | 4 |
| Total | 37 | 39 | 1 | 77 |
The regions that reported the most acute cases in the first quarter of 2024 were London (n=19), the South East (n=15), and the South West (n=11) (Table 5). These data are based on the patient’s postcode where available. Where patient postcode is not available, the location of the referring hospital or laboratory is used. As such, location of cases does not necessarily reflect the geographic area where the tick bite occurred. Of the 77 acute cases in the first quarter of 2024, 5 reported foreign travel; 2 cases reported travel to Europe, 1 case reported travel to Africa, 1 case reported travel to North America and for 1 case travel was unspecified.
Table 5. Laboratory-confirmed acute cases of Lyme disease in England by centre, Q1 2022 to Q1 2024
| UKHSA Centre | Q1 2022 | Q2 2022 | Q3 2022 | Q4 2022 | Total 2022 | Q1 2023 | Q2 2023 | Q3 2023 | Q4 2023 | Total 2023 | Q1 2024 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| East Midlands | 5 | 5 | 6 | 7 | 23 | 1 | 0 | 22 | 4 | 27 | 4 |
| East of England | 6 | 14 | 25 | 19 | 64 | 3 | 8 | 27 | 8 | 46 | 10 |
| London | 21 | 31 | 69 | 34 | 155 | 16 | 28 | 120 | 42 | 206 | 19 |
| North East | 2 | 3 | 15 | 6 | 26 | 3 | 2 | 23 | 12 | 40 | 2 |
| North West | 13 | 12 | 28 | 16 | 69 | 10 | 10 | 47 | 12 | 79 | 9 |
| South East | 25 | 61 | 136 | 46 | 268 | 25 | 63 | 195 | 50 | 333 | 15 |
| South West | 18 | 56 | 114 | 35 | 223 | 18 | 55 | 202 | 32 | 307 | 11 |
| West Midlands | 5 | 1 | 22 | 5 | 33 | 4 | 11 | 27 | 9 | 51 | 3 |
| Yorkshire and Humber | 5 | 9 | 26 | 14 | 54 | 7 | 6 | 41 | 11 | 65 | 4 |
| Unknown | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| Total | 101 | 192 | 441 | 182 | 916 | 87 | 183 | 704 | 180 | 1,154 | 77 |
Toxoplasmosis
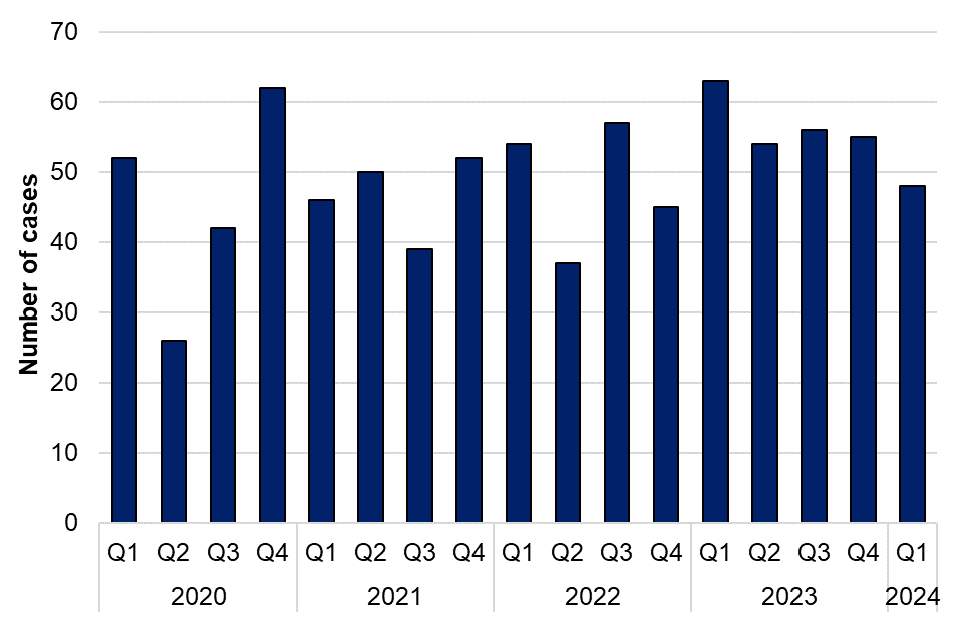
Data for toxoplasmosis in England is obtained from the Toxoplasma Reference Unit (TRU, Public Health Wales Swansea). There was a total of 48 confirmed toxoplasmosis cases reported in the first quarter of 2024
Figure 4. Laboratory-confirmed cases of toxoplasmosis in England by quarter, Q1 2020 to Q1 2024
Of the total confirmed cases, 16 (33%) were male (aged 19 to 52, median 33 years), 31 (65%) were female (aged 10 to 88, median 34 years) and 1 case where sex was unknown. Table 6 shows the age group and sex distribution.
Table 6. Laboratory-confirmed cases of toxoplasmosis in England by age group and sex, Q1 2024
| Age group (years) | Male | Female | Unknown | Total |
|---|---|---|---|---|
| 0 to 14 | 0 | 2 | 1 | 3 |
| 15 to 24 | 2 | 3 | 0 | 5 |
| 25 to 44 | 12 | 16 | 0 | 28 |
| 45 to 64 | 2 | 7 | 0 | 9 |
| 65 and over | 0 | 3 | 0 | 3 |
| Unknown | 0 | 0 | 0 | 0 |
| Total | 16 | 31 | 1 | 48 |
Chlamydia psittaci / Chlamydia abortus
Data for C. psittaci / C. abortus was obtained from the Respiratory and Vaccine Preventable Bacteria Reference Unit (RVPBRU) in Colindale and from cases reported by local laboratories through SGSS. As of 1 January 2023, a confirmed case of psittacosis is defined by a positive 16S rRNA PCR result or culture isolation only.
It should be noted that the existing PCR assay is unable to differentiate between C. psittaci and C. abortus. However, as there are currently no other reliable methods of psittacosis identification, the numbers presented in these reports will reflect laboratory-confirmed cases with a positive PCR result for C. psittaci / C. abortus.
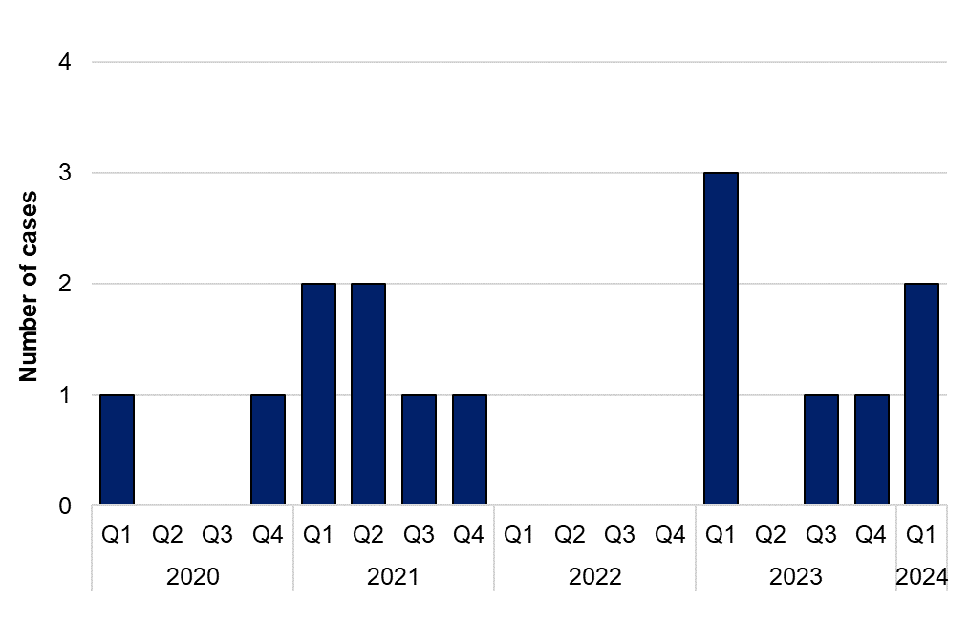
There were 2 reports of C. psittaci / C. abortus in the first quarter of 2024. Figure 5 shows the number of laboratory confirmed cases of C. psittaci / C. abortus between 2020 and 2024.
Figure 5. Laboratory-confirmed cases of Chlamydia psittaci / Chlamydia abortus in England by quarter, Q1 2020 to Q1 2024
Other zoonotic organisms
Data for other zoonotic organisms are obtained from cases reported by local laboratories through SGSS. Region is based on the patient postcode where available. If patient postcode is not available, then location of the referring hospital or laboratory is used.
There were 7 reports of Capnocytophaga spp. infection in the first quarter of 2024. Of the cases reported this quarter, 4 were further speciated to C. canimorsus. Of those speciated, 2 cases were male and 2 were female, and cases were reported in the South West (n=2), Yorkshire and the Humber (n=1), and West Midlands (n=1). Capnocytophaga spp. are frequently carried in the mouths of companion animals (cats and dogs) or humans, and may be associated with an animal or human bite, or opportunistic infections in those with impaired immune systems.
There were 4 reports of Mycobacterium marinum infection in the first quarter of 2024. Of these, 3 cases were male and 1 was female, and cases were reported in the South West (n=3) and London (n=1).
There were 3 reports of Erysipelothrix rhusiopathiae in the first quarter of 2024. Of the 3 cases reported this quarter, 2 were male and 1 was female, and cases were reported in the South West (n=2) and West Midlands (n=1).
There were 2 reports of toxigenic Corynebacterium ulcerans infection in the first quarter of 2024, compared with 3 reported in the same quarter in 2023. Of the cases reported this quarter, both were male. One case reported contact with companion animals. In England, contact with companion animals remains the most frequently reported exposure for individuals with confirmed toxigenic C. ulcerans infections. However, the animals may not show evidence of infection and it is not always possible to confirm the carriage of C. ulcerans in animals
There were 5 reports of Taeniasis in the first quarter of 2024. Of the cases reported this quarter, 1 was further speciated to T. saginata.
There were no reports of Toxocariasis in the first quarter of 2024.