Employment advisers in improving access to psychological therapies: client research
Updated 5 May 2022

© Crown copyright 2022
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/employment-advisers-in-improving-access-to-psychological-therapies/employment-advisers-in-improving-access-to-psychological-therapies-client-research
DWP research report no. 1013
A report of research carried out by IFF and Bryson Purdon Social Research LLP on behalf of the Work and Health Unit.
Crown copyright 2022.
You may re-use this information (not including logos) free of charge in any format or medium, under the terms of the Open Government Licence
Or write to:
Information Policy Team
The National Archives
Kew
London
TW9 4DU
Email: psi@nationalarchives.gov.uk
This document/publication is also available on our GOV.UK website
If you would like to know more about DWP research, email: socialresearch@dwp.gov.uk
First published April 2022.
ISBN 978-1-78659-402-0
Views expressed in this report are not necessarily those of the Department for Work and Pensions or any other government department.
Executive summary
This report forms part of an evaluation of the Work and Health Unit (WHU) programme to increase the number and integration of Employment Advisers (EAs) in Improving Access to Psychological Therapies (IAPT) services. EA support is intended to help clients struggling with staying in, returning to, or finding work. The primary aim of the evaluation is to robustly determine the additional employment and health outcomes associated with EA support, within an integrated care setting. This report presents findings from the impact strand of the evaluation, drawing on evidence from a longitudinal telephone survey with IAPT clients in areas where EA support had been introduced or increased, five months and twelve months after entering the IAPT service. A further telephone survey was conducted with IAPT clients in areas where EA support had not yet been introduced or increased, twelve months after entering the IAPT service. Statistical matching was used to create a comparison group from the areas where support had not been introduced or increased, to estimate the impact of EA support. This analysis was supported by longitudinal qualitative interviews with clients from eight case study IAPT services that experienced increased EA support, around five months and twelve months after entering the service.
The research found that:
- On entry to the EA service, clients were more likely to be in employment than looking for work and hence – to a large extent – EA support entailed helping them make an existing job work better for them. This included having difficult conversations with employers, such as requesting reasonable adjustments.
- From a client perspective, EA support was well integrated with therapy and delivered effectively. Clients particularly valued the balance between practical, emotional and motivational support.
- Impact estimates suggest that EA support had a positive impact on employment for clients who were out of work on entry to IAPT, and indicative evidence of a positive impact on job search activities. However, there was also some evidence of EA support being linked to lower levels of confidence in finding work amongst those who remained out of work.
- Impact estimates found no positive impact on return to work among those who were off work sick at IAPT entry.
- Longitudinal survey analysis identified indicative positive outcomes for clients who were working on entry to IAPT, in terms of job retention, reduced presenteeism and improved work relationships. However, it was not possible to make impact estimates for this group due to difficulties in establishing a suitable matched comparison group.
Acknowledgements
This report was commissioned by the Work and Health Unit (WHU), a joint unit for the Department for Work and Pensions (DWP) and Department for Health and Social Care (DHSC).
We would like to thank Lyndon Clews, Laura Parkhouse, David Johnson, Owen Davis, Navneet Dalton and Mark Langdon in WHU’s Employment Advisers in Improving Access to Psychological Therapies (EA in IAPT) Evaluation Team for their guidance and contributions throughout the project, and to Chris Sutton and Anna Saunders who designed the evaluation. We would also like to thank Kevin Jarman and his delivery team for their input and support when liaising with IAPT providers, and to the members of the IAPT Outcomes and Informatics group for their advice and expertise.
We would like to thank all IAPT providers involved in the evaluation for the time taken to introduce the evaluation to their clients, and thus providing a crucial gateway to invite services users to take part.
We would also like to thank all the participants that gave up their time to take part in the study. Without them, of course, the research would not have been possible.
Authors and researchers
A large team of research partners worked on the study and contributed to the report.
IFF Research, were the lead contractors and led on all quantitative fieldwork and some qualitative interviews with EAs in IAPT clients. Lorna Adams and Rowan Foster, Directors, headed up the IFF team responsible for the research. Gill Stewart, Associate Director and Christabel Downing, Senior Research Manager, were responsible for day-to-day management of the study. Ed Castell, Senior Research Executive, Johanna Lea, Senior Research Executive, Nicky Mitchell, Research Executive and Rachel Keeble, Research Executive worked on the fieldwork, delivery, analysis and reporting.
ICF led on all qualitative fieldwork and analysis with clients. Lucy Loveless, (Managing Consultant) led the ICF team, and managed all aspects of the qualitative research strand. Hayley D’Souza (Research Consultant) carried out client interviews, worked on data analysis, and authored the qualitative findings sections of this report. Jennifer Uddin (Research Consultant) carried out client interviews and worked on data analysis. Aisha Ahmad (Senior Consultant) carried out client interviews.
Caroline Bryson and Susan Purdon of Bryson Purdon Social Research (BPSR) lead on the impact analysis for this report.
Scott Weich from the School of Health and Related Research (ScHARR) at Sheffield University led the literature review which underpinned the study and provided academic guidance throughout.
Glossary of terms
| Term | Definition |
|---|---|
| Access to Work | A publicly funded employment support programme that provides personalised support to those who are disabled or have a physical or mental health condition to start or stay in work. |
| Advisory, Conciliation and Arbitration Service (ACAS) | Non-departmental public body designed to improve organisations and working life through the promotion and facilitation of strong industrial relations practice. |
| Clinical Commissioning Group (CCG) | NHS organisations in England responsible for the planning and commissioning of health care services for their local areas. |
| Clinical Lead | Clinician taking lead responsibility for the clinical aspects of a IAPT service and who bears the responsibility for clinical governance and ensuring high standards of clinical care and service delivery. |
| Constructed counterfactual | A matched comparison group constructed using the available data on baseline characteristics (for example, age, gender, level of qualifications, among others). This gives a matched comparison that is very similar to the treated group on all selected characteristics. |
| Employability partners | Refers here to stakeholders from organisations delivering employment support and advice who work collaboratively with Employment Advisers in IAPT services. |
| Employment Adviser (EA) | Person providing a range of support and advice on issues related to employment to clients who are in and out of work. |
| EQ-5D-3L | A survey instrument for measuring health-related quality of life across the following five dimensions: mobility, self-case, usual activities, pain/discomfort and anxiety/depression. Each dimension has three levels. The 3-level version was introduced in 1990 by the EuroQol Group. |
| Health state | A five-digit number that describes the patient’s health state in relation to five dimensions measured by the EQ-5D-3L. |
| IAPTUS | Case management software system for clients receiving psychological therapies in an IAPT service. |
| Improving Access to Psychological Therapies (IAPT) | Programme that began in 2008 and delivers services that provide evidence-based psychological therapies to people with anxiety disorders and depression. |
| iMTA Productivity Cost | A measure of the number of days lost to workplace presenteeism - the extent to which an individual’s health conditions impact their ability to perform their usual workplace duties. This is calculated using the iMTA Productivity Cost Questionnaire (iPCQ). |
| Individual Placement and Support (IPS) | An employment support service integrated within community mental health teams for people who experience severe mental health conditions. It provides intensive, individual support to people to help them to move towards and into or stay in employment. |
| Jobcentre Plus (JCP) | Government-funded employment service that aims to help people of working age find employment. JCPs provide resources to enable jobsearchers to find work, offer information about training opportunities, and administer claims for benefits. |
| Logic model | A graphic which represents the theory of how an intervention produces its outcomes. It presents, in a simplified way, the hypothesis or ‘theory of change’ that process evaluations test. |
| ONS4 | A measure of personal well-being (PCB) developed by the Office for National Statistics. Respondents are asked four 11-point survey questions on life satisfaction, happiness, anxiety and feeling life is worthwhile. |
| PCMIS | Case management software system for clients receiving psychological therapies in an IAPT service. |
| Presenteeism | Refers to when individuals are in work but, because of illness or other medical conditions, not fully functioning. In many situations there is a productivity loss as an employee’s focus is not on the work due to illness or related distractions. |
| Productivity loss | A decrease in the effectiveness of productive effort in the workplace. In this reporting, productivity loss is measured in terms of the number of working days lost due to impairments causing inefficient working. |
| Propensity score matching | A statistical method for generating a matched comparison group for an intervention. It is useful in instances where data on a potential comparison group is available, but where there are observable profile or baseline differences between the intervention group and the comparison group. Propensity score matching generates weights for the comparison group which, when applied, reduce any such differences. |
| Reasonable adjustments | Refers to changes made to the work environment to remove barriers or disadvantages that enable people with a disability to work safely and productively. Under the Equal Opportunity Act 2010, ‘disability’ includes: physical, psychological or neurological disease or disorder, illness, whether temporary or permanent. |
| Senior Employment Adviser (SEA) | Manage and support a team of EAs in offering a support service to individuals with common mental health problems to gain, return to or retain employment. |
| Service Lead | Post-holder leading an EA service with overall responsibility for its delivery. |
| Service Provider | Contracted organisation that provides services on behalf of a CCG. |
| Statistical significance | a difference is said to have statistical significance, or be statistically significant, if it is likely not caused by chance for a given statistical significance level. In the current report, statistical significance is reported at a 95 per cent confidence level i.e. 95 per cent confident it did not happen by chance. |
| Time 1 | The time point at which clients were interviewed approximately five months after starting support through IAPT. |
| Time 2 | The time point at which clients were interviewed approximately twelve months after starting support through IAPT. |
| Wave One | Overall, 40 per cent of CCGs were selected for the trial. Wave One refers to those randomly-allocated (within the trial selection) where there was an increase in the number of Employment Advisers embedded in IAPT services from March 2018. CCGs selected for the trial |
| Wave Two | Overall, 40 per cent of CCGs were selected for the trial. Wave Two CCGs refers to those randomly-allocated (within the trial selection) where there was no increase in the number of Employment Advisers embedded in IAPT services from March 2019. |
| WHO-5 | The World Health Organization-Five Well-Being Index assesses subjective psychological well-being to measure quality of life using a five-point scale across five statements. This gives a raw score of 0 to 25 where a higher score denotes better well-being. In this report, scores are also grouped into ‘unimpaired well-being’ (13 to 25), ‘impaired well-being’ (9 to 12) and ‘likely depressed’ (0 to 8). |
Summary
Introduction
This report forms part of the evaluation of the Employment Advisers in Improving Access to Psychological Therapies (EAs in IAPT) programme. IAPT is a NHS England programme that provides evidence based psychological treatments for people with mental health problems, principally anxiety and depression. The EAs in IAPT delivery model has been designed as an integrated service that brings together employment advice and support with IAPT provision to enable IAPT clients to stay in or take up work. Both IAPT and EAs in IAPT are voluntary interventions.
EAs in IAPT is funded by the cross-government Work and Health Unit (WHU), jointly sponsored by the Department for Work and Pensions (DWP) and Department of Health and Social Care (DHSC).
Employment Advisers (EAs) provide employment support within the service, supporting clients typically falling into one of three categories: in work but struggling; employed but off work sick; or looking for work. Since 2008, EAs have been introduced in some IAPT services and findings from a pilot report (DWP, 2013)[footnote 1] suggest that they may be effective in supporting an individual back to work.
The WHU provided funding for approximately 350 additional EAs across IAPT services in 40 per cent of Clinical Commissioning Groups in England (CCGs; clinically-led statutory NHS bodies responsible for the planning and commissioning of health care services for their local area), split into two waves. IAPT services in Wave One CCGs recruited their EAs so that they were ready to see clients from 1 March 2018, whilst services in Wave Two CCGs received investment later so that their EAs were in place to start to see clients on 1 March 2019. Allocation to Wave One and Wave Two was at random, and the Wave Two areas acted as a control group for Wave One.
In 2017, the WHU commissioned IFF Research, in partnership with ICF, Bryson Purdon Social Research (BPSR) and the School of Health and Related Research (ScHARR) at Sheffield University, to undertake a process and impact evaluation of the EAs in IAPT programme. The primary aim of this evaluation was to robustly determine the likely additional employment and health outcomes from receiving Employment Adviser support in an integrated care setting with IAPT services. A process evaluation looking at the implementation of the programme was published in July 2019.[footnote 2]
Methodology
This report draws on evidence from:
- A quantitative telephone survey with 1,609 Wave One IAPT clients – both those who saw an EA and those who did not – around five months after entering the service.
- A follow-up telephone survey with 755 Wave One clients who saw an EA, around 12 months after entering the service, and a corresponding survey with 609 Wave Two IAPT clients (including those who saw an EA and those who did not).
- Longitudinal qualitative interviews with EA clients from eight Wave One case study services, around five months after entering the service (with 55 clients) and a follow-up around six to eight months later (with 36 clients).
All fieldwork was carried out between January 2019 and March 2020. All fieldwork was completed before the national lockdown caused by the COVID-19 pandemic in March 2020.
This report explores the profile of EAs in IAPT clients, the experiences and longitudinal outcomes of these clients, and the impact of seeing an EA by comparing Wave One clients to clients who served as a counterfactual from Wave Two. Outcomes explored include work-related, job search activity, well-being and wider health outcomes.
Key considerations when interpreting results
It is important to note that clients included in this evaluation who received support from an EA did so at the start of the programme, when the service model was not yet fully embedded and national training for EAs had not been rolled out. Relatively small sample sizes (a by-product of the consent process outlined in Chapter 1) create limitations in some areas of analysis.
Furthermore, it is important to note that the sample is not representative of the whole EAs in IAPT pilot population; not all sites engaged with the consent process (and, thus, not all sites were included in the sample) and the sample is skewed towards those who took up EA support. This skew is due to EA clients being more likely than therapy-only clients to be asked to take part in the evaluation, although the extent of the bias is unknown as there is no reliable information on the population profile. Additionally, the small sample sizes mean that the impacts have to be very large before reaching statistical significance. Because of this, patterns of non-significant impacts are commented on in this report, even though the evidence they provide is relatively weak. Given these caveats, the estimates of impact should be treated as indicative only.
Such limitations are clearly flagged as and where relevant.
Another consideration when reviewing findings is that a ‘positive’ employment outcome and a ‘positive’ IAPT outcome may not always be aligned. For example, an individual may retain employment (considered a positive employment outcome) but this work could be negatively impacting their mental health and may result in future psychological treatment needs.
Client profile and support needs
The profile of EA clients
For all three key client groups of interest (employed and working, employed off sick and looking for work), the majority of IAPT clients sampled and surveyed in Wave One areas took up the offer of EA support. Those off work sick on entry to IAPT services were the most likely to take up EA support (79 per cent), as did a slightly lower proportion of clients looking for work (73 per cent) and around three-fifths (59 per cent) of clients who were employed and working.
Sampled and surveyed Wave One EA clients had a fairly even split between the three key employment groups: 36 per cent were employed and working, 30 per cent were employed off sick and 31 per cent were looking for work. Compared to those who took up EA support, IAPT clients who declined or were not offered a referral to EA support by their therapist were more likely to be in work (both 47 per cent).
Outside of the three key groups, small minorities of EA clients were employed but off work for other reasons (such as maternity or compassionate leave, one per cent) or retired and not looking to work in the future (two per cent).
Reasons for taking up EA support
For employed EA clients (including those working and off sick or off work for other reasons such as maternity leave), many took the service up because they felt it could help them with difficulties at work. Some of these clients were seeking help in managing their health conditions at work, for example through coping mechanisms or reasonable adjustments. Poor work relationships were also common, with some clients alluding to workplace harassment and bullying.
EA clients who were looking for work on referral mainly wanted help with the practicalities of applying for jobs such as CV writing, interview technique and knowing where to look for jobs. Those who had been out of the job market for a while or had left their previous job under stressful circumstances, often wanted help with confidence building for re-entry into the job market.
Apparent in all situations was the relationship between employment and mental health. Clients commonly described about how the situations they were seeking support with were both exacerbating and exacerbated by poor mental health.
Reasons for declining EA support
Among IAPT clients who declined the EA offer, many (44 per cent) gave reasons implying they had no employment needs. That said, other responses (such as prioritising health, 40 per cent, or already receiving support elsewhere, 17 per cent) imply employment issues were present for a decent proportion of these clients too.
Client experience of the EAs in IAPT service
Views of the EA service
Overall, experiences of the EAs in IAPT service were very positive. Just over threequarters (78 per cent) of EA clients surveyed agreed that the sessions had been useful, and the vast majority felt their adviser was understanding of their needs (92 per cent) and that the support they received was tailored (82 per cent). Clients were less positive when asked about the extent to which support helped them achieve key employment goals (e.g. to stay in work, return to work or find work), although over half (57 per cent) agreed it had.
In interviews with EA clients, EAs were highly commended for their friendly and flexible approach; clients particularly appreciated having a choice of how (i.e. face to face or via telephone) and how often sessions could take place and being able to maintain communication via email between sessions.
Furthermore, many clients commented that they appreciated receiving independent, non-judgmental advice, and that there was a good balance between practical, emotional and motivational support.
Client experiences also point to successful and valued integration between employment advice and therapy support with IAPT provision. Generally, clients felt the two elements of the service enhanced each other and created an effective holistic package.
Common employment activities
More than two-thirds (68 per cent) undertook at least four types of employment support activities with their EA. The most common activity was developing an action plan (77 per cent). Job search activities were common too; around three-quarters (74 per cent) explored how their skills could apply to other jobs and a third (32 per cent) had help with job interview techniques. Although more common among clients looking for work, these types of activities were prevalent among the employed. For example, 71 per cent of employed clients explored how their skills could apply to other jobs, compared to 80 per cent of clients who were out of work. This may reflect that many in work were unhappy with their current employment situation.
As mentioned, practical skills were often well balanced with emotional and motivational support. EAs provided emotional support through positive reinforcement of their abilities, encouraging them to stay with their employer where appropriate and reassuring the client that they would work together to address the difficulties with their employer. They provided advice on how to start difficult conversations with employers, for example, asking for adjustments at work through role play exercise.
Longitudinal outcomes for clients receiving EA support
Overall, more than two-thirds (68 per cent) of EA clients surveyed experienced a positive employment outcome between entry to IAPT and 12 months later; that is, they had either remained employed and in work (31 per cent), moved into employment (16 per cent) or returned to work after being on leave (21 per cent).
Other clients experienced more negative employment outcomes or no change. One in ten (10 per cent) clients had moved out of employment, 18 per cent remained out of work, and very small minorities had either remained employed but off work (three per cent) or moved from working to being on leave (one per cent).
It is important to note that the changes over time observed in this section are not necessarily attributable to the employment support received; some level of change may have resulted from the therapy alone, and some may have occurred without any intervention. That said, clients who saw an EA were asked the extent to which the support helped them to achieve their specific employment aim; these figures are presented in the subsections below.
Outcomes for those working on entry to IAPT services
The vast majority (87 per cent) of EA clients who were employed and working on entry to IAPT services were also working 12 months later – two-thirds (66 per cent) of these clients remained in the same role as on entry to IAPT. Just under two-thirds (63 per cent) of EA clients who stayed in work agreed that support from their EA had helped them do so.
Within this group, 91 per cent had experienced at least one positive in-work outcome during this time, with “softer” outcomes relating to experiences of work, workplace and job role adjustments and relationships most common. For most of these outcomes, the majority of clients felt support received from their EA and IAPT services played a role in the positive outcome. Clients were most likely to state that adjustments to job roles/responsibilities and working hours could be directly attributed to the service (27 and 26 per cent, respectively).
Improvements in presenteeism (an individual’s productivity at work being negatively affected by working whilst sick) were seen among this group, with the average number of days of productivity loss (in a four-week timeframe) decreasing from 6.10 across all working clients at the start of IAPT, to 1.72 days 12 months later.
Outcomes for those off work sick on entry to IAPT services
After twelve months, around seven in ten (69 per cent) clients who were off work sick on entry to IAPT services had returned to work, with fewer than half (44 per cent) returning to their previous job role. More than three-quarters (77 per cent) of clients who had returned to work felt the EA and/or IAPT service had helped them to do so, with more than half (56 per cent) ‘strongly agreeing’.
Presenteeism in this group reduced substantially between entry to IAPT services and approximately 12 months later. On average, these clients had a productivity loss of 7.91 days in the four weeks they were last in work before IAPT treatment; this decreased to an average of 1.21 days by 12 months.
Outcomes for those looking for work on entry to IAPT services
Half of EA clients (50 per cent) who were looking for work on entry to IAPT services had found work 12 months later. Nearly two-thirds (65 per cent) of clients who had found work agreed that IAPT services had helped them do so, with 48 per cent ‘strongly agreeing’.
As well as simply not being successful in finding a suitable job, reasons for being out of work at 12 months included a movement into education, taking on a voluntary role or caring responsibilities (all of which could be seen as positive outcomes), or job searching being affected by health.
The impact of EAs in IAPT support
The impact of EAs in IAPT support was measured by comparing the 12-month outcomes of IAPT clients who saw an EA against those of a matched[footnote 3] comparison group of IAPT clients from Wave Two areas, with similar IAPT baseline characteristics, who had not seen an EA. This report focuses on those looking for work and those off work sick when they began IAPT because it proved infeasible to identify a plausible comparison group for those employed and working when they saw the EA. Information collected on the reasons why people chose to see an EA suggests that two thirds (67 per cent) of those who saw an EA while in work did so because they were experiencing difficulties at work. No similar information was collected from those not seeing an EA, to allow for the identification of a plausibly similar comparison group for those employed and working.
Despite rigorous methods, for the two groups where impact estimates have been made, it is possible that the matched comparison groups may not give an unbiased estimate of the counterfactual. The comparison groups may have started with less acute employment problems and better well-being than the EA groups. If this is the case the impacts reported may be underestimated and some of the negative impacts may be spurious. Conversely, it could be that those in the out of workgroup seeing an EA were very actively engaged in seeking work and the out of work comparison group, on average, less so, in which case impacts on this group might be overestimated.
In addition, it should be noted that the sample sizes, particularly for the matched comparison groups, are small, limiting the conclusions that can be drawn. There are 223 EA clients who were looking for work when they started IAPT, but just 68 in the comparison group. The numbers are very similar for the off work sick group, with 227 seeing an EA and just 70 in the comparison group. Given these caveats, the estimates of impact presented should be treated as indicative only.
Relative to their matched comparison group, those who were looking for work on IAPT entry and saw an EA were significantly more likely to be employed and working after 12 months than their matched comparison group. Half (48 per cent) of those who saw an EA were employed and working compared to three in ten (29 per cent) of the matched comparison group. The small samples sizes mean that impacts have to be very large before reaching statistical significance so patterns of non-significant impacts are commented on in this report, even though the evidence they provide is relatively weak. Among those still looking for work after 12 months, there is a consistent positive pattern of non-significant evidence that those who had EA support are both engaging in more job search activity and having a stronger desire to find work than their matched comparison group. For instance, 48 per cent of those who saw an EA reported higher levels of job search activity compared to 38 per cent of those in the comparison group. Similarly, those receiving EA support appear to be more likely to think they could consider entering work than the matched comparison group (85 per cent compared to 77 per cent). However, counter to this, they appear to be less confident that they will find work than the matched comparison group, although, again, the differences are not statistically significant (18 per cent compared to 35 per cent had higher confidence).
There is only one piece of statistically significant evidence for EA support having an impact on the well-being or health of those who were off sick when they started IAPT: those who had seen an EA are statistically significantly less likely to have reported visiting a GP in the previous two weeks (74 per cent versus 59 per cent had not done so). However, there is no statistically significant evidence of EA support having an impact on hospital outpatient or Casualty use or health-related quality of life (according to the EQ-5D measure) among this group.
There is very little statistically significant evidence of EA support having an impact on those who were in work but off sick when they began IAPT. However, there is nonsignificant evidence that they are in fact less likely to be employed and working after 12 months compared to their matched comparison group (72 per cent compared to 81 per cent). One possible explanation of this observed difference is that it may reflect a potential bias in the matched comparison group, with the EA group perhaps starting with more problems at work than the matched comparison group. An alternative hypothesis is that the EA group may be slower to re-enter work because liaison with employers is ongoing. Among the sub-set of those who had re-entered work after 12 months rather than being off sick, there is non-significant evidence that those who had seen an EA are less likely to report that their work is affected by physical or psychological health problems. There is no statistically significant evidence of EA support having an impact on health service use among this group.
Conclusions
A challenge of this evaluation was securing access to a representative sample of clients for the whole EAs in IAPT pilot population for the primary research. The variation in volumes of contact details provided by sites (with some services returning none at all) raises concerns about the consistency with which the process was applied. This, as well as the fact that these tended to be ‘early’ clients, means that the impact findings need to be treated with some caution.
That said, the conclusions that can be drawn from the evaluation to date are that:
- Those engaging with an EA were more likely to be in employment than looking for work and hence – to a large extent – EA support involved addressing difficulties at work.
- A close link between employment and mental health was evident among most patients seeking EA support.
- From a client perspective, EA support seems to have been delivered well.
- Across all client groups, qualitative research indicated that what really seemed to work in delivering EA support was the combination of practical, emotional and motivational support.
- A key intended outcome of the EAs in IAPT programme was to create an integrated service with therapeutic support and this was largely achieved from the clients’ perspective.
- Impact estimates found a positive impact from EA support on entry to work for clients who were looking for work on entry to IAPT. There was also an indicative (but non-significant) evidence of EA support having a positive impact on job search activity for those still looking for work at 12 months.
- Impact estimates did not find a positive impact on the likelihood to have returned to work among those who were off work sick.
- Impact estimates showed a positive impact in one area of healthcare utilisation; those off work sick and who had seen an EA were significantly less likely to have seen a GP in the previous two weeks. There were no other statistically significant health impacts.
1. Introduction
The Employment Advisers (EAs) in Improving Access to Psychological Therapies (IAPT) programme is funded by the Work and Health Unit (WHU), the crossgovernment unit, jointly sponsored by the Department for Work and Pensions (DWP) and Department of Health and Social Care (DHSC). The service seeks to provide integrated psychological treatment and employment support to enable people to stay in, return to, or take up work. In 2017, WHU commissioned IFF Research, in partnership with ICF, Bryson Purdon Social Research (BPSR) and the School of Health and Related Research (ScHARR) at Sheffield University, to undertake a process and impact evaluation of the EAs in IAPT programme.
This report provides findings from the impact components of the evaluation of the EAs in IAPT programme. It draws on evidence from:
- A quantitative telephone survey with Wave One IAPT clients – both those who saw an EA and those who did not – around five months after entering the service.
- A follow-up survey with Wave One clients who saw an EA, around 12 months after entering the service, and a corresponding survey with Wave Two IAPT clients (both those who saw an EA and those who did not).
- Longitudinal qualitative interviews with clients from eight Wave One case study services, around five months after entering the service and a follow-up interview between six and eight months later.
All fieldwork was undertaken between January 2019 and March 2020.
1.1. The EAs in IAPT programme
IAPT, established in 2008, is an NHS England programme that provides evidence based psychological treatments for people with common mental health problems, principally anxiety and depression.
In 2009, an EA pilot pathfinder programme was introduced in 11 areas in IAPT services across England, which set out to test the benefits of offering employment support via Employment Advisers (EAs) to help IAPT clients remain in or return to work. Findings of a DWP evaluation in 2013[footnote 4] suggest that EAs may be effective in supporting an individual back to work. At the time of the 2013 report, the EA service was only available for employed clients, i.e. those working or those employed but off sick. A recommendation of the report was to expand access to include out of work clients. Shortly after its inception in 2015, WHU secured funding to extend the employment advice component of IAPT provision. The key catalyst in renewing the EAs in IAPT pilot was a policy recommendation in the 2014 RAND Europe report on psychological well-being and work,[footnote 5] which specified that vocational support should be embedded in local IAPT or psychological therapy services, based on the principles of the Individual Placement and Support (IPS) model.[footnote 6]
The programme adds additional capacity to deliver employment support to the target areas, by funding 350 additional EA posts across 40 per cent of Clinical Commissioning Groups (CCGs) over a three-year period. The original IAPT business case recommended a 1:8 ratio between EAs and Therapists and the additional funding added sought to bring the EA to therapist ratio closer to 1:8. The programme was rolled out in two waves: Wave One which went live in March 2018 and Wave Two which went live in March 2019. This was designed as a randomised control trial (RCT) between CCGs, with half the CCGs getting immediate funding (Wave One) and the others receiving extra investment a year later and acting as a control group (Wave Two) for the period without additional investment.
Each CCG or service directly recruited their EAs or commissioned a third party to provide them. The service has been designed to be managed and coordinated through the appointment of Senior Employment Advisers (SEAs) with the aim of ensuring that there is one SEA for up to a maximum of six EAs.
The EAs in IAPT delivery model has been designed as an integrated service that brings together employment advice and support with IAPT provision. Therapists and EAs are expected to work collaboratively to deliver a personalised service to clients based on their individual needs. The service is designed to support people with common mental health conditions who are either:
- In work but struggling or facing difficulties in the workplace;
- Employed but off work sick/suspended from work; or
- Looking for work.
Participation in employment support is voluntary and can be accessed at any point in the client journey from referral to discharge. Clients referred to the IAPT service are intended to follow one of four pathways according to their needs, although there is some variation between CCGs. Following assessment by a therapist they will receive:
1. Therapeutic treatment only;
2. Therapeutic treatment and employment support simultaneously;
3. Employment support continued beyond point of discharge/after their
therapeutic treatment has been completed;
4. Employment support while waiting for therapeutic treatment.
The approach is client-led so that if there are no pressing employment concerns during assessment or subsequent therapeutic sessions, only therapeutic treatment will be offered. If employment support is clearly indicated at the outset, pathway two or four (depending on the waitlist for therapy and considered appropriateness of starting employment support first) would be followed and if it only emerges later that employment is an issue, then pathway three would be followed.
As well as delivering an integrated employment advice and therapy service to the target group, the programme aims to contribute towards a wider systemic and cultural change, whereby structural barriers to integrated working around employment and health are challenged. At the local level, the intention was to support change through developing collaborative working relationships between EAs in IAPT providers and local employers, trade unions, Jobcentre Plus (JCP) and support organisations within the local labour market.
1.2. Research aims
The focus of this evaluation has evolved over time, as shown below.
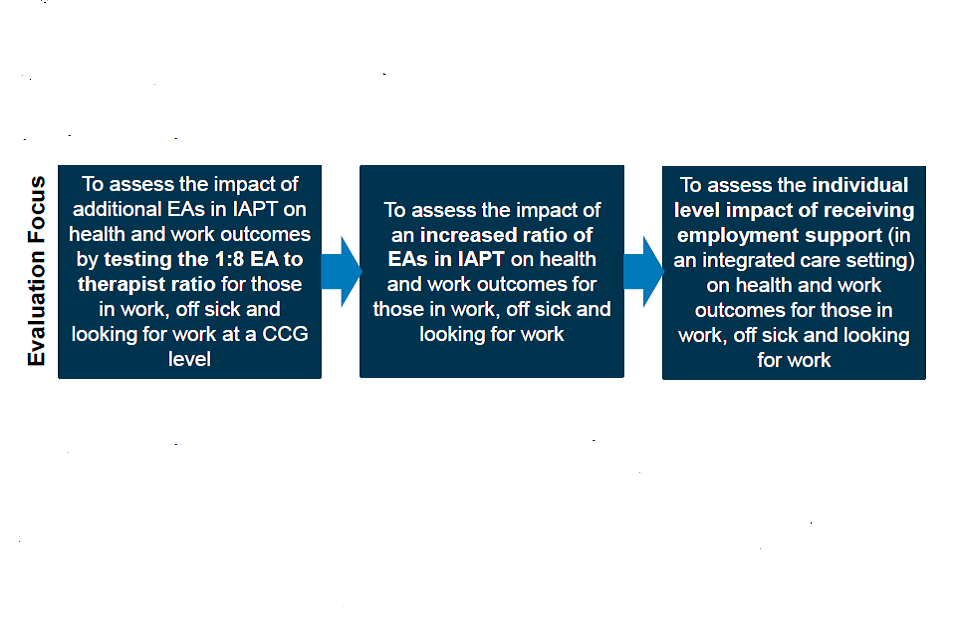
The original shift in focus from testing the ratio to testing an increased ratio was due to the limited likelihood of the 1:8 ratio being achieved and maintained across all Wave One providers in the evaluation period. It was then later decided that assessing the individual level impact of receiving EA support was a more primary focus than reviewing the impact of “more EAs” in an IAPT service, although analysis of the latter is included in Appendix C.
Ultimately, the primary aim of this evaluation was to robustly assess the likely additional employment and health outcomes from receiving Employment Adviser support in an integrated care setting with IAPT services. The evaluation aims to identify any differences in outcomes and experience for three key groups of clients, those:
- Employed and working – referred to as employed in work or working in this report unless otherwise specified
- Employed but off work due to health reasons – referred to as employed off work sick or off sick unless otherwise specified
- Out of work but looking to work in the future – referred to as looking for work in this report unless otherwise specified
Impact will be evaluated by comparing work and health outcomes for Wave One clients (who received treatment in a setting where the increased in EAs had been rolled out) and Wave Two clients (who did not see an EA and who received therapeutic treatment in a setting where the increased in EAs had not yet been rolled out). Thus, Wave One will be the treatment group and Wave Two will be the counterfactual group.
The results of the evaluation will inform the future design of integrated employment support in IAPT services and any further roll out decisions.
1.3. The evaluation approach
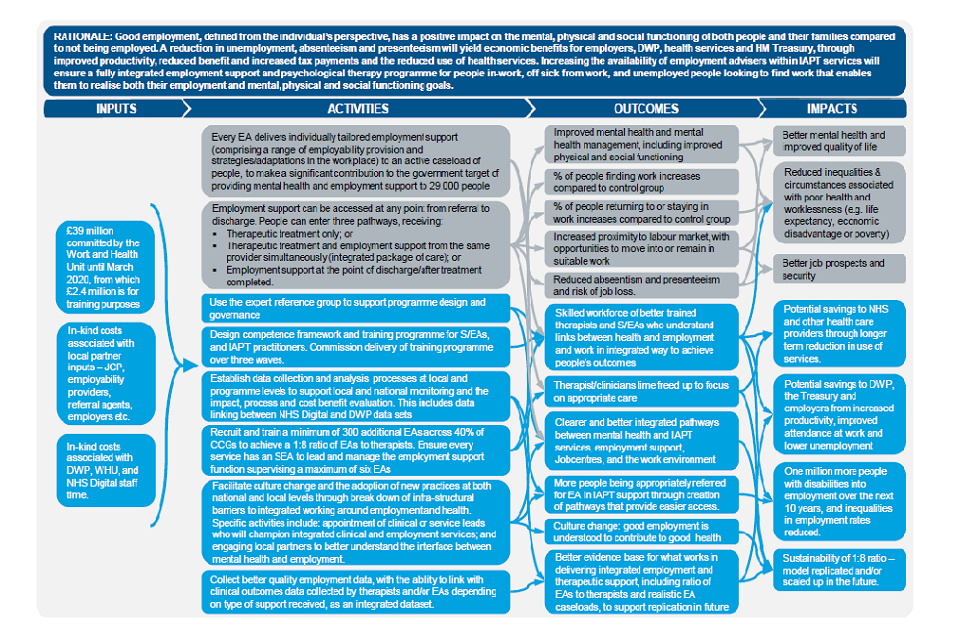
The evaluation began with a scoping phase designed to inform and develop the evaluation team’s understanding of the programme, refine the evaluation approach and develop a programme level theory of change (ToC) logic model. A review of the evidence for integrated work-related advice and support interventions for people with common mental health conditions was also undertaken by ScHARR at Sheffield University. The logic model is shown overleaf (Figure 1.1).
Figure 1.1 EAs in IAPT logic model
Evaluation components were designed to gather process learnings and to test the theory of change by which intended outcomes of EAs in IAPT were met. The evaluation consists of five key components:
1. Case study visits to eight Wave One CCGs in which face to face, in-depth interviews were carried out with EAs, SEAs, therapists, programme coordinators and managers, and employability partners (such as Job Centre Plus), following the increase in EA numbers. These case studies provided process information in terms of what went well and areas for improvement during the process of increasing EA numbers in Wave One sites. In addition, the interviews with therapists and EAs explored some elements of impact, such as what it was about the EA support that helped clients.
2. A ‘Time 1’ survey of 1,609 clients, conducted just in Wave One areas approximately five months after the start of IAPT treatment. The timing of this survey was based on an average expected treatment length of 3-4 months. This survey focussed on the take up and experiences of receiving employment advice and also collected some early outcome data.
3. A ‘Time 2’ survey of 1,364 clients from Wave One (n=755) and Wave Two (n=609) approximately 12 months after the start of IAPT treatment. In Wave One areas only those who have received support from an EA were included. This survey allowed comparison of outcomes for those who received employment support in Wave One areas with ‘those who would have been likely to receive employment advice if the ratio of EAs had made it possible’ in Wave Two areas. This collected information on longer-term outcomes.
4. Client interviews: In-depth telephone interviews were carried out with clients who had experienced EA support within an IAPT service that had increased its EA numbers (i.e. Wave One areas). The interviews approximately five months after entry to IAPT services explored views on the EA support they had received, what benefits they gained from the support, and crucially, what elements of the support had contributed to these benefits, to understand what it was about the support that created any positive impact. Follow-up qualitative interviews were carried out with 36 of these clients around six to eight months after their initial interviews for the purposes of longitudinal analysis, to establish whether any benefits created by the support remained.
5. Further analysis of IAPT data (pending data access) to supplement the impact estimates reported on in Chapter 5 of this report.
This report builds on a previous process report, published in July 2019, which presented evidence from the eight case studies outlined in component 1 above.[footnote 7]
This report presents findings from qualitative and quantitative fieldwork with IAPT clients (evaluation components 2, 3 and 4 above) to explore the outcomes and impacts that can be attributed to the programme. Data collection methodologies for each component are outlined later in this chapter.
1.4 Recruitment and consent process
This study was confirmed by the Health Research Authority (HRA) as a Service Evaluation, meaning no further ethical approval from the HRA or Research Ethics Committee (REC) was required. However, due to the nature of the audience it was considered important to follow a thorough informed consent process before contact details were passed from IAPT providers to the research partners, and again when clients were directly contacted for the research.[footnote 8] An overview of the three-step consent process is provided in Figure 1.2 below, with further details in Appendix A. The process outlined below was followed for both qualitative and quantitative client interviews.
Figure 1.2 Overview of client consent process
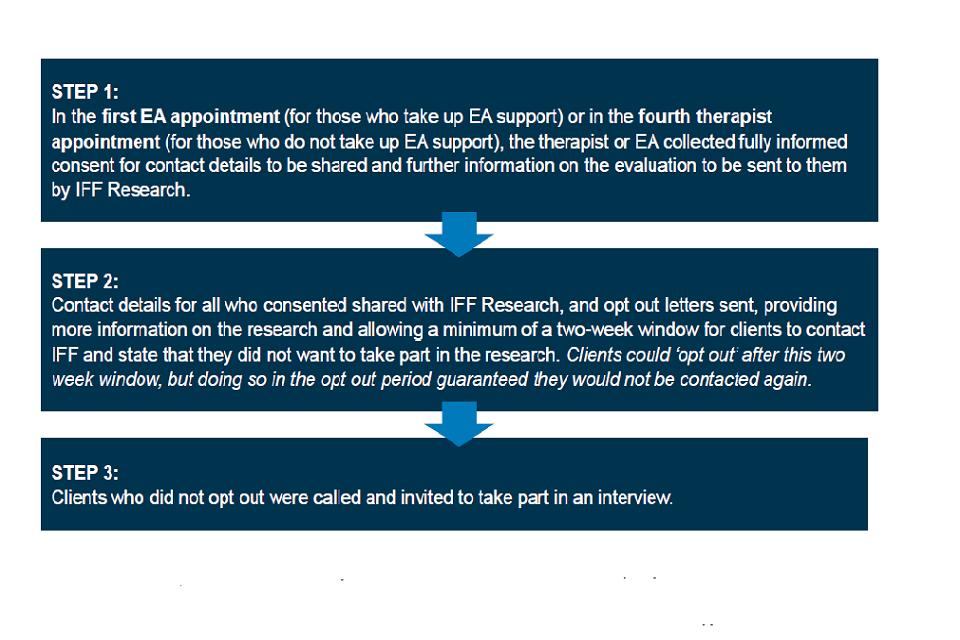
As suggested by stakeholders, this consent process was designed primarily to avoid the potential distress for individuals with mental health conditions being contacted for research with no or limited prior knowledge.
It is important, however, to outline the methodological limitations of this approach, namely:
-
Small sample sizes: The process was heavily reliant on EAs and therapists taking time in their sessions to introduce the evaluation and gain consent. Some providers did not engage with the consent process at all (sample was not shared with the evaluation team in these cases) and others mentioned that it was not always deemed appropriate to discuss a research evaluation in their session, or clients did not meet the necessary threshold of appointments for doing so (i.e. they did not see an EA and had fewer than four therapy sessions). Ultimately, this had an impact on the volume of sample available for the research.
-
Bias in the sample: It is highly likely that those consenting differed from those who did not, and those who were asked for consent differed from those who were not (due to reasons outlined above). One by-product of the consent process is that clients in the research sample were more likely to have taken up EA support than those in the general IAPT population. This is because:
- EAs were more engaged and complicit with the consent process – anecdotal evidence from site visits indicated that the evaluation and collecting consent was more ‘top-of-mind’ for EAs than therapists, and therapists were less engaged in the process of introducing the research and collecting consent in their sessions. Driving the relative opposition from therapists were two concerns; many did not want to take treatment time away from clients within their appointment, and many felt it was inappropriate to mention given the content of discussions or the state of their clients.
- Therapy-only clients were required to reach their fourth appointment before consent was collected to avoid impact on treatment, but some clients left the service before reaching a fourth therapy appointment. EA clients, on the other hand, were asked in their first EA appointment.
1.5. Data collection for this report
Time 1 survey
The purpose of the Time 1 survey was to speak to Wave One clients relatively soon after they were likely to have finished receiving support through IAPT. An average length of time receiving IAPT support was identified as around three to four months, so the survey sought to speak to clients around five months after starting IAPT treatment.
The survey, conducted via telephone interview, explored the offer and experience of EAs in IAPT support and collected early outcome data (details on outcomes collected are outlined later in this chapter).
Sample
Sample was received directly from Wave One IAPT providers in monthly batches, between January and July 2019.
In total, useable[footnote 9] contact details were received for 3,268 Wave One IAPT clients for the purpose of the Time 1 survey. On receipt of the opt out letter, a total of 218 clients opted out before their fieldwork period, resulting in a starting sample of 3,050 records.
Fieldwork
Fieldwork took place between January and September 2019. On average, the survey took 22 minutes to complete.
A total of 1,609 telephone interviews were completed, a response rate of 53 per cent of the starting sample. A full breakdown of final sample outcomes is shown in Appendix B.
Within this survey, two-thirds (66 per cent) of clients had taken up EA support. Of these, 961 respondents agreed to re-contact for the Time 2 survey. This equates to a 91 per cent agreement to the follow-up.
Time 2 survey
The purpose of the Time 2 survey was to speak to both Wave One and Wave Two clients around 12 months after they started receiving IAPT treatment, to explore longer-term outcomes (details on these outcomes are explored later in this chapter). Again, this survey was conducted via telephone interview.
Sample
The vast majority of the sample for Wave One clients were those that took part in the Time 1 survey, received EA support, and agreed to re-contact (n=961). This sample was ‘topped up’ by a further 126 records who were not able to be included in the Time 1 survey. The top up sample was screened within the survey to determine whether they received EA support.
For Wave Two, the sample was received directly from IAPT providers. In total, useable[footnote 10] contact details for 1,012 Wave Two IAPT clients were received.
On receipt of the opt out letter,[footnote 11] a total of 51 clients opted out before their fieldwork period, resulting in a total starting sample of 2,048 records.
Fieldwork
Fieldwork took place between August 2019 and March 2020. A total of 1,364 interviews were completed – 755 for Wave One clients and 609 for Wave Two clients - with an overall response rate of 67 per cent of starting sample. On average, the survey took 20 minutes to complete.
The full breakdown for final sample outcomes can be found in Appendix B.
Qualitative interviews with clients
The purpose of the qualitative strand was to explore in greater depth how clients came to use the service, what support they received, whether they had experienced any benefits or impacts from the support received, as well as what specific elements of support they perceived to be the most useful/impactful.
Clients were contacted for depth interviews around five months after they started IAPT treatment and then follow-up around six to eight months later (12 months after starting IAPT treatment).
The interview at the five-month point focused on:
- The client’s experience of employment and the barriers they faced to finding or sustaining work;
- Their experiences of and perspectives on engaging with the EAs in IAPT service; and,
- Early benefits and impacts of the service, any areas for improvement and any future expectations or support needs.
Follow-up interviews (i.e. those at the 12-month point) focused on:
- What had happened since the client was first interviewed;
- Progress towards/into employment, returning to work after sick leave, or employment sustained, and changes in associated behaviours (interest in finding work, change in job search behaviour, etc.);
- A review of their future expectations and ambitions – including their confidence in finding or sustaining work;
- The extent to which the benefits of EA support received have been sustained and any factors that may have enabled or prevented this; and
- With hindsight, a review of their experience of EAs in IAPT to identify what worked well, what less so etc.
Sample
Clients were from one of eight case study areas (aligned with the eight areas selected for the process evaluation). The case study areas, selected from a possible 40 CCGs participating in Wave One of the programme, were as follows:
- Buckinghamshire CCG
- Camden CCG[footnote 12]
- City and Hackney CCG
- Dorset CCG
- East Riding of Yorkshire CCG
- Leicester City CCG
- Nottingham and Nottinghamshire CCG
- St Helen’s CCG
The following sampling approach was taken to maximise the range of contexts, thus ability to explore contextual factors and common enablers and challenges.
CCGs were chosen to include a mix of:
- NHS England regional teams;
- Rural, urban and combined rural/urban areas (as described at local authority level); and,
- Deprivation levels, as defined by the 2015 English Indices of Deprivation.[footnote 13]
The sample was agreed with WHU and where chosen areas did not give consent to participate (n=2), substitute areas with similar characteristics were selected.
A random selection of 348 records from case study areas - ensuring a spread by case study as far as possible – were invited to take part in the qualitative interviews. In total, 348 records were contacted for qualitative interviewing. The sample for the follow-up interviews (at the 12-month point) consisted of participants who agreed to be re-contacted at the end of their five-month interview (n=58). Clients who took part in the qualitative interview did not take part in the Time 1 or Time 2 surveys.
Fieldwork
A total of 55 depth interviews were completed via telephone at the five-month point (between February and March 2019). Follow-up interviews were conducted with 35 EA clients between September and December 2019. Table 1.1 shows the breakdown of interviews by the key employment groups.
Table 1.1 Number of qualitative interviews completed, by employment group
| Employment status on entry to IAPT | Five-month point | Follow-up |
|---|---|---|
| Employed in-work | 49 | 23 |
| Employed off work sick | 4 | 3 |
| Looking for work | 14 | 10 |
| Total | 55 | 36 |
Analysis
Interviews were recorded, with participant consent,[footnote 14] and fully transcribed. Transcriptions were coded and analysed thematically using a framework analysis approach. Framework analysis is a systematic approach to analysing qualitative data. The approach enables the identification of common themes, and the differences and relationships between them, in order to draw explanatory conclusions clustered around key areas of interest.[footnote 15] The approach is particularly useful in the analysis of semi-structured interviews and when multiple researchers are working on projects that involve large amounts of qualitative data.
Following framework analysis, the results were written up under thematic headings before being synthesised with the quantitative findings.
1.6 Outcome measures
Drawing on the aims of the trial, the evaluation measured the impact of EAs in IAPT on a range of employment, job search, mental health and well-being outcomes, all collected in the quantitative surveys.
This section provides more detail on each of the outcome measures, including the points at which the data were collected and how it was analysed, divided into:
- Work-related outcomes;
- Job search related outcomes;
- Well-being outcomes; and,
- Wider health outcomes.
Outcome measure data was collected at three time points in reference to:
1. Entry to the IAPT service (baseline) – collected retrospectively for all survey participants. For Wave One clients who completed a Time 1 survey, baseline data was collected retrospectively within this survey, approximately five months after entering IAPT services. For all Wave Two clients, and the few Wave One clients who did not take part in a Time 1 survey, this data was collected retrospectively in the Time 2 survey, approximately 12 months after entering IAPT services.
2. Five months after entry to IAPT service – data for this time point was only collected for Wave One clients who completed the Time 1 survey.
3. 12 months after entry to IAPT services – data for this time point was collected for all Wave One and Two clients who completed a Time 2 survey.
Due to the nature of some outcome measures and the necessary timing of surveys, baseline data was not collected for all measures. Some measures were considered too difficult for clients to accurately recall retrospectively given the time that had passed since the time point, and the nature of the question. A summary of the time points for which we have data on each outcome measure is included in the sections below.
Work-related outcomes
A core aim of EAs in IAPT is to help people with employment-related issues which, are making it difficult to retain return to or find “good” work. As such, the impact of EAs in IAPT against the work-related outcomes was dependent on the client’s journey since entering IAPT. These outcomes and who they were measured for is shown in Table 1.2.
Table 1.2 Work-related outcome measures and audience asked
| Work-related issue | Remained employed and working | Returned to work from being off sick or off for other reasons | Moved into employment |
|---|---|---|---|
| More job satisfaction | Yes | No | No |
| More job enjoyment | Yes | Yes | Yes |
| Better workplace relationships | Yes | No | No |
| Beneficial adjustments made in work | Yes | No | No |
| Improved career progression, prospects, and security | Yes | No | No |
| Improved presenteeism | Yes | Yes | No |
| Motivation and confidence to stay in work | Yes | Yes | Yes |
How each of these measures were collected and the timing or their collection is summarised below.
- The following questions were based on a ‘Yes’, ‘No’ or ‘Don’t know’ response:
- Clients were asked whether they were getting more job satisfaction and enjoying their job more since they started receiving support through IAPT.
- Clients were asked if any of the following things which indicate better
workplace relationships had happened since receiving support through
IAPT:
- Your relationship with your employer has improved
- Your relationships with colleagues have improved
- Clients were asked if any of the following things which indicate beneficial
adjustments at work had happened since receiving support through IAPT:
- You have adjusted your working hours to suit you better
- You have increased your working hours
- You have changed your roles and responsibilities to suit you better
- Your employer has made adjustments to improve the working environment for you
- Clients were asked if any of the following things which indicate improved
career prospects, progression and security had happened since
receiving support through IAPT:
- Has your pay rate, salary or income increased?
- Have your future pay and promotion prospects improved?
- Do you have better job security?
- Your employer has a better understanding of how to maximise the contribution you can make at work
- A subset of questions from the Institute for Medical Technology Assessment (iMTA) Productivity Cost Questionnaire (PCQ) were used to assess impact of EAs in IAPT on presenteeism, for clients who were employed and working or employed but off sick on entry to the service and at subsequent survey points. Presenteeism relates to the notion that continuing to work despite illness, such as anxiety, can often result in reduced productivity. To ascertain presenteeism, survey respondents were asked in the four weeks before entering IAPT how many days they were bothered by psychological problems at work, and on those days to rate on a 0 to 10 scale how their work was affected by these problems (i.e. the efficiency score).)
To calculate lost productivity due to workplace presenteeism, the number of days worked while impaired is multiplied by ‘one minus the efficiency score divided by 10’ for these days:
Number of workdays impaired X [1 – (efficiency score/10)]
This determines the amount of time lost in the four weeks due to workplace presenteeism.
- Motivation for staying in work was measured with the question: “On a scale of 1 to 5, where 1 means not at all and 5 means very, at this moment in time how motivated are you to stay in work?” Motivated was measured as ‘4’ or ‘5 - Very’.
- Confidence in staying in work was measured with the question: “On a scale of 1 to 5, where 1 means not at all and 5 means very, at this moment in time how confident are you in staying in work?” Confident was measured as ‘4’ or ‘5 - Very’.
Table 1.3 Timing of data collection for work-related outcomes
| Work-related issue | IAPT start (retrospective) | Five-month point (W1 only) | 12-month point |
|---|---|---|---|
| Employment situation (in-work, off sick, looking for work) | Yes | Yes | Yes |
| Improvements in quality of job (i.e. “suitable” work) and relationships in the workplace | No | Yes | Yes |
| iMTA PCQ Presenteeism score | Yes | No | Yes |
| Motivation and confidence for staying in / returning to work | No | Yes | Yes |
| Job enjoyment | No | Yes | Yes |
Job search outcomes
Despite not entering employment as a result of EA support, a positive outcome would be evidence that someone is closer to entering work. The evaluation included a range of measures about people’s job search activity and propensity to look for work:
- Levels of job search activity are measured using the Finnish Institute of Occupational Health (FIOH) Job Seeking Activity Scale (Revised). This seven-item job search activity scale measures the frequency with which individuals undertake key job search activities, for example contacting employers or searching for job vacancies on the internet. The original version of this measure was developed at the Finnish Institute of Occupational Health (FIOH)[footnote 16] and subsequently modified for use in the UK labour market.[footnote 17] The modified version has two additional items, to address online job search and CV submissions to internet search sites. Survey respondents are asked whether and how often they had undertaken a range of job search activities in the previous two weeks.:
A rating for each activity from ‘not at all’ to ‘every day’ over the past two weeks is used to create a scale from 1 (no job search) to 4 (scoring ‘every day’ on all seven items). The impact of EA support is measured using both the mean scale score and a binary variable where those scoring 1.0 to 1.6 are coded as doing ‘lower levels of job search activity’ job search and those scoring higher than 1.6 are coded as doing ‘higher levels of job search activity’. This binary was based on the comparison group data to produce roughly equal splits between high and low activity groups.
- Also an element of the JIOH Job Seeking Activity Scale, the number of vacancies applied for and number of CVs submitted in the past two weeks are categorised as two separate outcome variables and reported as a mean.
- Motivation for finding a job was measured with the question: “On a scale of 1 to 5, where 1 means not at all and 5 means very, at this moment in time how motivated are you to find work?” Motivated was measured as ‘4 or ‘5 - Very’.
- Confidence in finding a job was measured with the question: “On a scale of 1 to 5, where 1 means not at all and 5 means very, at this moment in time how confident are you in finding work?” Confident was measured as ‘4 or ‘5 - Very’.
Table 1.4 Timing of data collection for job search outcomes
| Job search outcomes | IAPT start (retrospective) | Five-month point (W1 only) | 12-month point |
|---|---|---|---|
| FIOH JSA scale (revised) | No | No | Yes |
| Jobs applied for | No | No | Yes |
| CVs submitted | No | No | Yes |
| Motivation for and confidence in finding work | No | Yes | Yes |
Well-being outcomes
In addition to helping clients with their employment goals, EA in IAPT could also improve mental health as measured by the IAPT Patient Reported Outcome Measures (PROMS), the Patient Health Questionnaire (PHQ-9), Generalised Anxiety Disorder Assessment (GAD-7) and the Anxiety Disorder Specific Measures (ADSMs). The evaluation measures the impact of EAs in IAPT on two well-being measures not collected as part of IAPT’s PROMS. This will be captured in the quantitative analysis. The evaluation measured the impact of EAs in IAPT on:
- The ONS4 Subjective Well-being questions ask individuals to rate themselves on a scale of 0 to 10 to four statements related to their well-being and life satisfaction:
“For the next questions, please give me an answer on a scale of zero to ten, where zero is not at all and ten is completely
- Overall, how satisfied are you with your life nowadays?
- Overall to what extent do you feel the things you do in your life are worthwhile?
- Overall how happy did you feel yesterday?
- Overall, how anxious did you feel yesterday?”
We report on the impact on the mean score of each item as well as the proportion scoring as ‘high’ (a score of 7 or more on satisfaction, feeling worthwhile and happiness, and 6 or more for anxiety). For the first three items, ‘high’ is a positive outcome, while for anxiety it is negative.
• The World Health Organisation-Five Well-being Index (WHO-5) is a five-item unidimensional measure of well-being with a good research pedigree. Individuals are asked to consider how often in the previous two weeks they have experienced particular feelings such as being in good spirits, feeling active and vigorous, calm and relaxed. This was asked across five statements. A score of 0 to 25 is derived by looking at responses across all statements. We report on the mean score where a higher score denotes better well-being. We also group scores into ‘unimpaired well-being’ (13 to 25), ‘impaired well-being’ (9 to 12) and ‘likely depressed’[footnote 18] (0 to 8).
Table 1.5 Timing of data collection for well-being outcomes
| Well-being outcomes | IAPT start (retrospective) | Five-month point (W1 only) | 12-month point |
|---|---|---|---|
| ONS4 Subjective Well-being | No | Yes | Yes |
| WHO-5 Well-being index | No | No | Yes |
Wider health outcomes
In addition to the mental health outcomes described above, the evaluation measured the impact of EAs in IAPT on client’s overall health, captured in the quantitative analysis via the EQ-5D[footnote 19] and use of health services during the past three months:
- The EQ-5D-3L[footnote 20] is a standardised measure of health status created by EuroQol. It comprises five questions, each of which asks about a different aspect of health (mobility, self-care, performing usual activities, pain and discomfort, and anxiety and depression). Focusing on how they feel today, people are asked to use a three-point scale to rate themselves as having no problems or issues (1) to it being extreme (3). Responses to the five questions can be aggregated to provide an overall health state score between 0 to 1, where a higher score denotes better health.[footnote 21]
- Self-reported visits to GP and engagement with mental health services (excluding IAPT) in the last two weeks and use of Casualty and Outpatients (excluding straightforward ante- or post-natal visits) services in the past three months are also used as measures of overall health.
Table 1.6 Timing of data collection for wider health outcomes
| Wider health outcomes | IAPT start (retrospective) | Five-month point (W1 only) | 12 month point |
| EQ-5D-3L health state | No | Yes | Yes |
| Engagement with health services | No | Yes | Yes |
1.7. About this report
Statistical differences
T-tests were used for comparing mean scores and z-tests for comparing percentages. The 95 per cent confidence level was used for establishing whether findings are significant or not, meaning we can be 95 per confident that the observed results are real and not an error caused by randomness.
Bold figures in tables indicate statistically significant difference to other subgroups displayed.
We have only reported relationships between data in the text of the report if they are statistically significant and if the relationship was thought to be relevant and/or interesting to the topic being discussed.
Relationships that were not statistically significant are not discussed in the text, except possibly in a few cases where an indicative relationship was thought to be relevant and/or interesting to the topic being discussed. Where this is the case, it has been made clear that the relationship is not significant.
Weighting
Data for this report has not been weighted.
It was not possible to weight the survey respondents to the EAs in IAPT pilot population due to a lack of accurate population data. Likewise, weighting to account for non-response at the five-month survey was not possible due to the following limitations with the sampling frame:
- Lack of demographic data in the sample frame
- There were indications of data inaccuracy in the original sample frame. For example, some individuals who were not marked as taking up EA support in the sample frame stated that they had done so within the survey. Findings from the pilot stage indicated that uptake of EA support is under-estimated in the original sample frame by approximately seven per cent.
- Inconsistency across CCGs for how support (whether EA support taken up; whether sought EA support to retain, return to or find work) and employment data (whether employed and working, employed but off work, or unemployed) were recorded in the sample frame.
The profiles of Wave One clients in the five- and 12-month surveys were compared to test for non-response bias. Owing to the low attrition between surveys, differences between the two profiles across key characteristics (age, gender, education level, employment status on entry and at five months, and subjective well-being) were negligible. As such, weighting was not required.
Key considerations when interpreting results
It is important to note that clients included in this evaluation who received support from an EA did so towards the start of programme roll out. There was good evidence in the Process Evaluation that processes earlier in the programme had not been streamlined, the service model lacked clarity and national training for EAs had not been rolled out. This means some areas identified for improvement by clients may be due to these earlier issues which have since been addressed.
Relatively small sample sizes (a by-product of the recruitment and consent process, as outlined earlier in this chapter) presented limitations in the analysis. For example, the sample sizes used in the estimation of impact are small and, as a result, only very large impacts would reach statistical significance. As a result, patterns of nonsignificant impacts are commented on in this report, even though the evidence they provide is relatively weak. Given these caveats, the estimates of impact should be treated as indicative only.
Limitations as outlined above are clearly flagged as and where relevant. Thoughts on how to address these limitations in the future are explored in the conclusions.
Furthermore, it is important to note that the sample is not representative of the wholeEAs in IAPT pilot population; not all sites engaged with the recruitment and consent process (and, thus, not all sites were included in the sample) and the sample is skewed towards those who took up EA support. This skew is due to EA clients being more likely than therapy-only clients to be asked to take part in the evaluation, although the extent of the bias is unknown as there is no reliable information on the population profile. Furthermore, sufficient population data for weighting against was not available. Reported findings should therefore be interpreted as findings for the research sample.
Another consideration when reviewing findings is that a ‘positive’ employment outcome and a ‘positive’ IAPT outcome may not always be aligned. For example, an individual may retain employment (considered a positive employment outcome) but this work could be negatively impacting their mental health and may result in future psychological treatment needs.
1.8. Structure of the report
Following this introduction, the report is structured into five chapters:
- Chapter 2 provides an overview of IAPT client profiles, including how EA clients differ from those who did not receive this support, and how the service was first introduced to clients;
- Chapter 3 explores the experiences of clients who took up EA support;
- Chapter 4 is a descriptive chapter exploring the longitudinal changes in work and health measures for clients who took up EA support, across the three key employment groups;
- Chapter 5 explores the impact of EA support by comparing Wave One clients to Wave Two counterfactuals; and
- Chapter 6 sets out conclusions and recommendations for future research on EAs in IAPT services.
2. Client profiles and introduction to the Employment Adviser (EA) service
This chapter presents the employment, demographic and health profiles of clients who took up Employment Adviser (EA) support, and how these characteristics compare to clients of the Improving Access to Psychological Therapies (IAPT) programme who either declined this support or were not offered it. It is important to note that, due to the methodological limitations described in the introduction to this report, findings are representative of the research sample only, rather than the wider population. The chapter also explores why individuals decided to take up EA support, with findings drawn from both the survey and qualitative interviews with clients, and, conversely, why this support was declined by some IAPT clients.
Chapter summary
* Referrals into EA support tended to be two-staged; clients self-referred into IAPT (usually following signposting from a GP), then the therapy team
referred them into Employment Adviser (EA) support following an assessment.
* Relative to sampled IAPT clients who did not access the EA service, EA
clients were more likely to be in overtly negative employment situations, such as employed but off work sick or looking for work (thus, less likely to be employed and working).
* Within the survey sample, there were no notable differences in health or
demographic characteristics between clients who took up support and those
who declined it, but individuals who were not offered (or do not recall being
offered) EA support tended to be older, have lower educational qualifications
and were more likely to be White British than those offered employment
support.
* For employed EA clients, many took the service up because they felt it could help them with difficulties at work, such as managing their health conditions (e.g. through reasonable adjustments or coping mechanisms) or poor
workplace relationships (including harassment and bullying).
* EA clients who were looking for work on referral mainly wanted help with the practicalities of applying for jobs, or with confidence building for re-entry into the job market if they had been out of the job market for a while or had left their previous job under stressful circumstances.
* That said, clients generally had low expectations for the extent to which the service would help them with their employment issues.
* Apparent for all clients was the relationship between employment and mental
health. Clients commonly described how the work situations for which they
were seeking EA support were both exacerbating and exacerbated by poor
mental health.
* For IAPT clients who declined the EA offer, reasons pertaining to a lack of
employment support needs were most common, although a large minority
said that they wanted to prioritise health over employment at the time.
2.1. Overview of referral process
Figure 2.1 provides an illustration of the possible pathways a client might follow from referral to the IAPT service and subsequently to an EA through to service exit.[footnote 22]
Possible client pathway through the EA in IAPT service
Step 1. Client referred to IAPT service by GP or self-referral. Go to Step 2.
Step 2. Client offered employment support at assessment. If, offer accepted, go to Step 4. If not, go to Step 3. If the client doesn’t accept support, they can still accept it at a later stage.
Step 3. Client receives therapeutic support.
Step 4. Client referred to EA service. Go to Step 5 to continue assessment.
Step 5. More detailed assessment of support needs is done by phone or face-to-face. Go to Step 6.
Step 6. Either employment support or therapy starts first. Go to Step 7.
Step 7. Support is delivered at the same time. Support provided includes post-therapy.
2.2. Take up of EA support by employment group
Within the survey sample, take up of EA support differed depending on the employment status of clients when they entered the IAPT service (see Figure 2.2). Comparing the three key employment groups EA services seek to support (those employed and working, employed but off sick, and those looking for work), those off work sick and those looking for work were more likely to accept support than those in work (79 and 73 per cent compared to 59 per cent, respectively). These groups were also slightly more likely to recall being offered the support in the first place.
As might be expected, those outside the three key employment groups for EA support (i.e. those off work due to other reasons and the retired/not looking to work in the future) were least likely to be offered EA support and subsequently take it up.
Figure 2.2 Offer and take up of EA support, by employment status on entry to IAPT
| Employment status | Took up EA suppoprt | Declined EA support | No recall of offer |
|---|---|---|---|
| Employed and working | 59% | 15% | 25% |
| Employed, off work sick | 79% | 9% | 12% |
| Employed, not working (other) | 44% | 35% | 22% |
| Looking for work | 73% | 10% | 17% |
| Retired/not looking to work in future | 26% | 20% | 54% |
2.3 Profile of clients who received EA support
This section presents the employment, demographic and mental health profiles of individuals in the sample who took up EA support, and how this compares to individuals who declined or were not offered this service.[footnote 23]
Employment and income
As shown in Table 2.1, overall, two-thirds (66 per cent) of individuals who took up EA support were employed. Clients who took up employment support were most likely to be employed and working (36 per cent) on entry to the IAPT service, with three in ten employed but off work sick (30 per cent). A similar proportion were looking for work (31 per cent). Small minorities were economically inactive i.e. retired or not looking to work in the future (two per cent) or employed but off work for non-health reasons (e.g. maternity or compassionate leave, one per cent).
Table 2.1 Employment status when started receiving IAPT support, by client group
| Employment status | Received EA suppport (%) | Declined EA suppoprt (%) | Not offered support (%) |
|---|---|---|---|
| Employed and working | 36 | 47 | 47 |
| Employed off sick | 30 | 18 | 13 |
| Employed off other | 1 | 4 | 1 |
| Looking to work | 31 | 23 | 23 |
| Retired / not looking to work | 2 | 10 | 15 |
| Base: All Wave 1 Time 1 survey respondents | 1,056 | 200 | 342 |
*Numbers in bold are statistically significant at a 95% confidence interval. Column figures may not sum to exactly 100 per cent due to rounding.
Among the employed, seven in ten (70 per cent) were working full time in a paid role for an employer, around a quarter (24 per cent) were working part time in a paid role for an employer and five per cent were self-employed.
Moving on to consider the employment status of clients that participated in EA support compared to those that did not, either because they declined the support or did not recall being offered it; the overall proportions in employment are broadly similar. However, the groups that did not access EA support were more likely to be employed and still working (47 per cent compared to 36 per cent). Both those who declined support and those who did not recall the offer were more likely to be inactive and not looking for work than those that did access support (10 and 15 per cent compared to two per cent). Both groups that did not access EA support were also less likely to be looking for work (23 percent for both those who declined support and those who did not recall the offer, compared to 31 percent of those who took up support).
This suggests that the EA support offer is reaching its intended target audiences i.e. individuals looking for work and those needing assistance to return to/maintain employment.
As shown in Table 2.2, EA clients tended to be on low incomes. EA clients generally had a lower income than the national average; two-fifths of EA clients (41 per cent) reported an individual annual income of £15,000 or below, while nationally £21,300 is the personal income limit for the 40th percentile (i.e. the salary at which 40 per cent of the population earn less).[footnote 24] This is broadly in line with the client groups that declined EA support and those not offered. However, clients who declined EA support were more likely to have an income of £45,000 or higher (nine per cent compared to five and four per cent for those who received or were not offered support, respectively).
Table 2.2 Total annual income (individual not household), by client group
| Annual income | Received EA support (%) | Declined EA support (%) | Not offered EA (%) |
|---|---|---|---|
| Less than £15,000 | 41 | 41 | 37 |
| £15,000 to £30,000 | 28 | 28 | 28 |
| £30,000 to £45,000 | 12 | 13 | 12 |
| £45,000+ | 5 | 9 | 4 |
| Don’t know / refused | 14 | 11 | 19 |
| Base: All Wave 1 Time 1 survey respondents | 1,056 | 200 | 342 |
*Numbers in bold are statistically significant at a 95% confidence interval. Column figures may not sum to exactly 100 per cent due to rounding.
Subgroup differences in employment status for EA clients
As shown in Table 2.3, there were some demographic and health differences among EA clients with different employment status at IAPT entry:
- Women were more likely than men to be employed (69 per cent compared to 62 per cent of males), although there were no significant gender differences in terms of whether individuals were working, off sick or off work for another reason.
- Clients with a long-term mental or physical health condition (i.e. one that had lasted 12 months of more) were more likely to be out of work (37 per cent) than clients without a long-term condition (28 per cent), while the latter were more likely to be employed but off work due to health reasons (35 per cent compared to 27 per cent with a long-term condition) at IAPT start.
- Likelihood of being employed and in work on entry to the service did not differ substantially by age, but clients aged 16 to 24 years old were much more likely to be looking for work than older clients (46 per cent compared to 29 per cent aged 25+), and the likelihood of being off work sick increased with age (from 14 per cent among 16 to 24 year olds to 44 per cent among the 60+).
Table 2.3 Demographic profile of IAPT clients, by EA offer and take up
| Demographic | Employed and working (%) | Employed off sick (%) | Employed off other (%) | Looking to work (%) | Retired / not looking to work (%) |
|---|---|---|---|---|---|
| Gender | |||||
| Male | 36 | 25 | <1 | 35 | 3 |
| Female | 36 | 32 | 1 | 29 | 2 |
| Age | |||||
| 16-24 | 36 | 14 | <1 | 46 | 3 |
| 25-34 | 41 | 23 | 1 | 35 | <1 |
| 35-49 | 38 | 33 | 1 | 26 | 2 |
| 50+ | 30 | 39 | <1 | 27 | <1 |
| Long-term health condition | |||||
| Yes | 36 | 27 | <1 | 33 | 3 |
| No | 37 | 35 | 1 | 27 | <1 |
| Base: Those who received EA support | 380 | 312 | 10 | 329 | 25 |
Demographic profile
Within the sample population, just under two-thirds of EA clients were women (62 per cent), a high proportion relative to the proportion of women nationally (51 per cent in England), although women are generally over represented in IAPT treatment. Clients tended to be aged 35 or older (63 per cent, with 34 per cent 35 to 49 years old). As expected, almost all EA clients were of “working age” (i.e. aged between 16 and 64, 99 per cent).
Most clients who saw an EA were white (86 per cent), predominantly White British (79 per cent); 12 per cent were Black, Asian, and minority ethnic (BAME).
Nearly half (46 per cent) had gained an education qualification at Level 5 or above, equivalent to undergraduate degrees, Higher National Diplomas, postgraduate certificates or higher.
As shown in 4, there were no differences in the demographic profile of those who received EA and those who declined support. However, there are some differences when comparing those offered support with clients who were not. This is perhaps indicative of the clients for whom employment advice was perceived most relevant, and possible assumptions in the IAPT service. IAPT clients who were not offered EA support were:
- More likely to be older (38 per cent were aged 50+ years, compared to 28 and 25 per cent among those who took up or declined support, respectively);
- Less likely to have Level 5+ educational qualification (35 per cent); and
- More likely to be White British (86 per cent).
Table 2.4 Demographic profile of IAPT clients, by EA offer and take up
| Demographic | Received EA support (%) | Declined EA support (%) | Not offered EA (%) |
|---|---|---|---|
| Gender | |||
| Male | 38 | 39 | 41 |
| Female | 62 | 62 | 59 |
| Age | |||
| 16-24 | 15 | 14 | 11 |
| 25-34 | 22 | 26 | 23 |
| 35-49 | 34 | 36 | 27 |
| 50+ | 29 | 25 | 38 |
| Ethnicity | |||
| White British | 79 | 83 | 86 |
| White Other | 7 | 7 | 4 |
| BAME | 12 | 11 | 10 |
| Level of qualifications [footnote 25] | |||
| Entry level qualifications | - | 1 | - |
| Level 1 qualifications | 3 | 5 | 3 |
| Level 2 qualifications | 16 | 17 | 23 |
| Level 3 qualifications | 22 | 21 | 21 |
| Level 4 qualifications | 4 | 2 | 4 |
| Level 5+ qualifications | 46 | 44 | 35 |
| Base: All Time 1 survey respondents | 1,056 | 200 | 342 |
*Numbers in bold are statistically significant at a 95% confidence interval. Subgroup column figures may not sum to exactly 100 per cent due to rounding.
Health and mental well-being
Around two-thirds (67 per cent) of individuals who saw an EA reported having longterm mental or physical health conditions or illnesses (i.e. which had lasted 12 months or more); this was in line with the proportion among those who declined (67 per cent) or were not offered (66 per cent) employment support.
As one might expect, mental health conditions were prevalent across all IAPT clients. At the point of entry to IAPT services, most clients – around nine in ten – reported experiencing anxiety and/or panic attacks (89 per cent), depression (85 per cent) and/or stress (92 per cent). This was broadly consistent across the three client groups, although individuals who declined EA support were slightly less likely to report having depression (78 per cent compared to 86 and 84 among those who received or were not offered EA support).
2.4 Reasons for taking up the EA service
Both the survey and qualitative elements of the research shed light on the reasons that clients took up EA support. Clients in the Time 1 survey were asked why they decided to take up the support from an EA, findings are shown in Figure 2.3.[footnote 26]
Figure 2.3 Most common reasons for taking up support from an EA
| Reasons for taking up EA support | Employed and working | Employed off sick | Looking for work | All |
|---|---|---|---|---|
| I felt it could help me get back to work | 21% | 24% | 74% | 39% |
| I was experiencing difficulties with relationships at work and wanted advice/support | 49% | 57% | 2% | 34% |
| My IAPT therapist encouraged me to | 24% | 25% | 24% | 24% |
| I liked idea of getting additional help and support | 12% | 15% | 31% | 20% |
| I liked idea of seeing someone about my employment needs | 12% | 9% | 14% | 12% |
| I just went along with what was suggested/happy to try anything | 6% | 11% | 12% | 10% |
| Help finding a new line of work/change of career | 16% | 6% | 3% | 9% |
| I really want a job | 5% | 3% | 19% | 9% |
| Other | 3% | 3% | 5% | 4% |
Base: Wave 1 survey - those who received EA support: All (1,056); Employed and working (380); Employed off sick (312); Looking for work (329).
Reasons given were largely dependent on whether an individual was employed (regardless of whether they were working, off sick or off for other reasons) or out of work (both those looking for work and the retired/not looking to work in the future).[footnote 27]
Clients who were looking for work when they entered the IAPT service typically felt that the EA support could help them back to work (74 per cent). Around a third (31 per cent) mentioned that they liked the idea of receiving additional help and support. These clients tended to be seeking practical support for job searching; for example, help with writing a CV and cover letter, knowing where to look for jobs and how to develop their interview technique. Some clients mentioned the need for general career guidance such as planning for a career change, or exploring different sectors or roles that they could work in.
Employed clients most commonly said that they were experiencing difficulties at work that they wanted EA support with; around half (49 per cent of those employed and working and 57 per cent of those off sick) were experiencing unspecified difficulties. Examples from the qualitative interviews of such difficulties included feeling overworked, difficulties attaining a work/life balance, and employer not aware or not supportive of their mental health needs. Around a third (32 per cent of those working and 38 per cent of those off sick) mentioned that difficulties pertained to work relationships.
Some clients mentioned experiencing difficulties relating to bullying, harassment at work, and employment-related disputes. Some sought employment-related legal advice which may have been related to these disputes.
Other difficulties at work were alluded to by individuals who anticipated that the service could help them negotiate reasonable adjustments (for example, reductions in working hours) and those who wanted to develop coping mechanisms such as stress-management and dealing with confrontation at work. Around a quarter of clients – both employed and out of work – mentioned that their IAPT therapist had encouraged them to take up the EA support (25 and 24 per cent, respectively).
The relationship between mental health and employment was evident in most situations and reasons for seeking support. Many clients who experiencing workrelated problems described how these issues were negatively impacting on their mental health during the interviews.
“The fact that the problem seemed to be work related, it was causing me a great deal of stress and anxiety and I was quite poorly at the time with it all as well and the reason why I didn’t look for another job was just lack of confidence, scared, I’m 50 something, who wants to employ me kind of feeling.” (Female, employed on referral)
In some cases, clients wanted to stay with their employer and resolve these problems but for others the preference was to find alternative employment. Commonly reported problems were:
- Anxiety made worse by being at work
- Anxiety and depression directly caused by a problematic work situation such as unsupportive manager or high workload
- Being off sick with work-related stress
- Work ‘taking over’ in life with little time or energy for anything else
- The impact of bullying or harassment at work
For some, their experiences at work had been extremely difficult:
“I was being victimised like a witch hunt…picked on basically, for whatever
reason” (Female, employed on referral)
“…it got to the point where I actually collapsed at work and got taken away in an ambulance” (Female, employed on referral)
Relatedly, some clients interviewed reported that their mental health condition was preventing them from finding or sustaining employment, and they did not feel they could overcome these challenges without support. For example, a few clients wanted to improve their confidence in applying for jobs or interacting with potential employers during the recruitment process. Some had also experienced a loss of confidence due to issues faced at work, or having been made redundant, and others felt that they were unable to find a job unsupported. This was the case for one client who stated:
“I didn’t make an effort to seek anything out. I didn’t want to do that by myself really” (Female, out of work on referral)
Some anticipated that improvements to their employment status as a result of this support would also positively impact their well-being; for example, through employment providing structure to their day and potentially reduce social isolation.
For some clients, their reasons for accessing support were complex and related to multiple barriers. This was particularly evident for a small number of clients, whose period of being out of work started by taking on caring responsibilities for a partner (see Maria’s case study, Chapter 4 page 102).
Expectations of support
Most clients did not expect that the service would have significant impacts on their employment status, health and well-being, and subsequent experience of EAs in IAPT support exceeded their initial expectations. For some, their initial expectations of the service were impacted by previous experiences of employment support including from Jobcentre Plus.
“My concern or my fear was that it would be something like it’s associated with the Jobcentre provision that I’d experienced many years ago about employment support, which I wasn’t really keen on, but it wasn’t like that at all” (Female, employed on referral)
A few clients interviewed noted that they only attended the EAs in IAPT service as their IAPT practitioner had advised them that it may help. These individuals tended to have no positive expectations of how the service could help them, however, many of these clients went on to improve their employment status or to experience improvements in well-being which they attributed to the EA in IAPT service. For some clients, their initial expectations can be attributed to having a sense of hopelessness around their employment situation, having tried to find employment without support previously, or in order to manage their own disappointment if the service could not help them.
Case study 1: Emma
Emma was employed as a live-in nanny on referral to the EA in IAPT service. She felt nervous about her first session with the EA. Her confidence was very low at the time, and she didn’t feel capable of thinking about her employment. She attended the first session because it was suggested by her IAPT practitioner and not because she particularly wanted to go.
Emma was supported by her EA to update her CV, search through job sites and to find alternative living arrangements as she wanted to have a separation between her home and work life. After 5 sessions with her EA, Emma had increased her confidence by being reminded of the skills she has to offer. She was able to find a permanent position through her own contacts, and says that she would not have pursued this job opportunity without having built her confidence through EA in IAPT service.
This and other examples from the qualitative interviews indicate that clients’ experiences of the service may exceed their expectations. This may indicate a need for therapists to be more explicit about how the service can help, potentially using case studies of how support has benefitted other clients to illustrate this.
2.5. Reasons for not taking up the EA service
Clients in the Time 1 survey who declined EA support were asked why this was the case. As shown in Table 2.5, just under half (47 per cent) reported that they did not take it up as they did not need employment support.
A substantial minority - 40 per cent - said that they wanted to focus on their health before thinking about employment, with this proportion increasing to 46 per cent among individuals with a long-term health condition (compared to 28 per cent without), and just over half (51 per cent) for men (compared to 33 per cent of women).
Just under one-fifth indicated that they were getting support elsewhere (17 per cent), for example from their union, employer or occupational health, while a minority (8 per cent) were unsure if or how the service could help with their needs.
Clients who were out of work were less likely to indicate that they had no need for employment support (30 per cent cited reasons pertaining to this, compared to 54 per cent among the employed), and were more likely to say that they were prioritising their health (50 per cent compared to 35 per cent).[footnote 28]
Table 2.5 Reasons for declining support from an EA by theme
| Reason | All (%) |
|---|---|
| No employment needs | 47 |
| I did not feel the need for employment support as I already had a job | 23 |
| I did not think I needed support remaining in work | 13 |
| I was not looking for employment due to other commitments | 8 |
| I did not think I needed support returning to work | 6 |
| I did not think I needed support finding work | 5 |
| Health reasons | 40 |
| I wanted to focus on my health before thinking about employment | 40 |
| Receiving support elsewhere | 17 |
| I was receiving support from my union | 10 |
| I was receiving support via occupational health or my employer | 6 |
| I want to see how the current support pans out and don’t want to have two things running | 2 |
| Negative / unclear perception of EA support | 8 |
| Didn’t think it would be able to help me with my employment needs | 8 |
| I didn’t understand what support was on offer | 1 |
| Other | 6 |
| Base: Wave 1 Time 1 survey who received EA support | 200 |
3. Client experience of the Employment Advisers in Improving Access to
Psychological Therapies (EAs in IAPT) service
This chapter explores the client experience of the Employment Adviser (EA) service, with findings taken from both the survey and client qualitative interviews around five months after clients entered Improving Access to Psychological Therapies (IAPT) services. The chapter focuses on activities undertaken, views of the service, aspects of support particularly valued and areas for improvement.
Chapter summary
* Client experience of the EAs in IAPT support was broadly very positive. The
majority of clients found the sessions useful, and most felt that their needs
were understood and the service was tailored to meet them. Positive views
were reported across the three key groups of interest (those in work, off sick, and those looking for work), although those out of work were slightly less positive.
* Clients tended to experience a range of employment-related support, which
included job search skills and practical activities, as well as confidence and motivational support. Various aspects of the EA service were identified as particularly valued by clients. These included:
* The structure (for instance length, content) and method (for instance via telephone or face-to-face) of the sessions, and flexibility of EAs in this regard.
* The friendliness of EAs and their provision of independent, non- judgmental advice
* The balance between practical, emotional and motivational support.
* The tailored nature of the support, which considered the skills, needs and preferences of each client.
* EAs challenging clients’ thought processes or assumptions around work and supporting them to ‘widen their horizons’ and think more broadly about what jobs they might do.
* Clients did not feel pressured into accepting a job offer or going back to work when there were opportunities to do so.
* EA support continued following a change to employment status, helpingindividuals sustain work. Although some clients commented that the sessions stopped when therapy was completed, which they felt was detrimental.
3.1. Initial impressions of the service
In qualitative interviews, a number of clients highlighted that the service was prompt, both in terms of initially contacting them after referral, and scheduling a first session without delays. They felt that this helped to build trust in the service from the start.
Many clients described their initial impression of their adviser as friendly and empathetic, and reported that they had put them at ease immediately. This was particularly important for clients with anxiety, who may be concerned about speaking to an EA for the first time.
“I thought that my anxiety and depression would make it difficult to meet with [the EA] as I didn’t know them. But when I went to my first appointment, [the EA] was very friendly and reassured me that they would go at my own pace.” (Female, out of work on referral)
Other clients noted that they were impressed that their EA was flexible in terms of the time and date of their first appointment. For some this set a positive tone for their first appointment and made them feel that their preferences and needs were prioritised, rather than constrained around the service.
Comparisons were made between the EA in IAPT service and previous support they had gained from Jobcentre Plus (JCP). One client noted that the EA showed them a wider range of job sites to search on compared to at JCP. Another client felt that the JCP took a “one size fits all” approach, in comparison her initial impression of the EA in IAPT service was that it was tailored to both her employment and mental health needs:
“[EA] reassured me by, a little bit by saying, they will help you with these things like managing your panic in interviews that’ll allow us time to work on other things in the counselling, that they’ll complement each other. From the very first phone call with [EA], I was reassured that this wasn’t a copy and paste service” (Female, employed on referral)
Negative feedback on the first appointment with an EA was more likely for those who had attended the service in the early days of set up. One client described the EA as friendly but seemingly lacking confidence in her role.
“She was really nice, sort of friendly, but she seemed a little bit, I don’t know, she seemed a little bit unsure of what she was doing unless she was new or something. It was more her manner that it was like she knew what she was supposed to be doing but it was more like going through the steps, didn’t seem that confident in it. At first I just thought, well I just wasn’t very optimistic about getting anything useful from it.” (Female, out of work on referral)
This likely relates to early challenges faced in the setup of the EA in IAPT service as detailed in the process report.[footnote 29] For example, EAs - particularly those without previous experience of delivering employment support - had to learn quickly and ‘on the job’. The national training offer was not available when Wave One went live, but has since been rolled out.
3.2. Types of support taken up
Clients who received support from an EA undertook a wide range of activities to help them find, return to, or stay in work. Approximately five months after entering IAPT services, more than two-thirds of EA clients (68 per cent) had undertaken at least four employment support activities; the most common activities are shown in Figure 3.1. Each of these activities are discussed in greater detail in this section, drawing on evidence from qualitative interviews. Just two per cent of respondents who received EA support reported that they did not undertake any of the given activities or could not remember doing so.
Figure 3.1 Most common activities undertaken as part of the EA service
| Common activities | Percentage |
|---|---|
| Developing an action plan | 77% |
| Understanding how skills that you already have could apply to other jobs | 74% |
| Information about other local support to help you stay in/return to/find work | 51% |
| Advice or guidance about what sorts of training you could do | 49% |
| Get information or help with Access to Work | 37% |
| Volunteering, work experience or a work placement | 33% |
| Help with job interview techniques | 32% |
| Identify changes that could happen in your workspace, to help you overcome difficulties | 27% |
| Got advice on pjased return to work | 23% |
| Other mechanisms to help you stay in/find/return to work | 44% |
Other mechanisms to help you stay in/find/return to work: unprompted responses
| Common activities | Percentage |
|---|---|
| Help with CV/cover letters | 15% |
| More help with my mental health/depression/anxiety | 5% |
| Information/advice about searching for a job | 5% |
Action plans
The most common activity undertaken was working with the EA to develop an action plan (77 per cent). This was most common among clients who were employed but off work due to health reasons (85 per cent).
In contrast to the survey, in the qualitative interviews few clients recalled creating an action plan. Where mentioned, clients found action plans helpful as they: focussed on a few key actions or goals; set out different employment options to consider; set concrete tasks to complete in a structured format. Action plans were also described as being a working document that could be adapted to the changing needs of the client. Benefits of actions plans given by clients interviewed are detailed in case study two.[footnote 30]
Case study 2: Lucy
Lucy was studying at university prior to being referred to the IAPT service. She had taken a year out from her studies due to depression and wanted to get a temporary job to support herself during her time off. She kept avoiding applying for jobs as she did not feel confident enough to do so. The EA created an action plan which set her tasks relating to applying for jobs to complete between their sessions. Lucy reflected that having this concrete task or “homework” to complete in her own time meant that she stopped avoiding this task. Through the EA support she increased her confidence in her skills and abilities and began to think of herself as a valuable employee who has something to offer potential employers.
“I felt empowered and like I could make choices and have preferences - it wasn’t all about what the employer wanted.”
The EA recommended that she apply for a part-time role at a major retailer, and the client got the job. The job enabled her to earn some money during her time off, get some work experience and further her confidence and sense of employability. At the end of her year out, she stopped working and returned to her studies full time as planned.
A few clients recalled their EA creating an action plan but did not feel that they benefited from it. Reasons given were that they preferred another support method (e.g. receiving feedback on their cover letter), or that they already had an action plan such as through engagement with the JCP.
Job search activities
Activities relating to job search and applications were very common; around threequarters of EA clients (74 per cent) in the survey explored how their skills could apply to other jobs and a third (32 per cent) had help with job interview techniques. Smaller proportions spontaneously recalled more activities such as CV and cover letter writing (15 per cent), general information/advice about job searching (five per cent) and updates concerning appropriate jobs (two per cent).
Although these types of activities were more common among individuals who were out of work at the start of their IAPT support, a substantial proportion of employed individuals undertook these activities too, highlighting the benefit of a client-led service where needs are defined by the individual, not their employment situation.
For example, 69 per cent of employed clients explored how their skills could apply to other jobs, compared to 84 per cent of clients who were out of work. This finding is in line with the reasons individuals took up support outlined in Chapter 2, which was that many employed clients were experiencing difficulties in work and wanted to explore options to change employer/job as a result.
“I haven’t had a CV or an interview for over 20 years. The jobs I’ve got have
been word of mouth. [I thought] where on earth do I start thinking about
another job?” (Female, employed on referral)
“So it was looking for work, practical advice. CVs were something because I’ve never done a job that needed a CV. All of my previous employment history
has been based on application forms so CV advice, particularly, like I say
advice on where to look for work, on how to look for work and just confidence
building really.” (Female, employed on referral)
Clients described specific elements of CV support as consisting of:
- Clients being shown examples of how to present their CV
- EAs reformatting clients’ CVs into a new template or supporting them to do this independently
- EAs and clients working together to identify skills and experiences to include in client’s CV
- EAs proofreading clients’ CVs, such as for one client where English was not their first language.
Clients also described how the EAs used reflective techniques to encourage them to identify their existing skills, areas to improve on, and how they could apply their transferrable skills to a (different) job. The tailored nature of such career guidance was also evident from the interviews. For example, as well as considering current skills, EAs also based advice on needs and personality. This included working around caring responsibilities, preferences for working outside of peak times and taking the location of jobs into consideration. Essentially, EAs were focussing on the ‘right job for the person in their current situation’.
Clients also described spending part of their face-to-face sessions searching through jobsites with the EA. Some also said that the EA flagged jobs the client could apply for in the session or in their own time, and sometimes emailed these jobs to them between sessions. There was also evidence of EAs using their local knowledge and contacts to flag job opportunities to clients which may indicate the benefit of having EAs situated within the community. Some clients were also signposted to job sites specific to their sector (e.g. arts jobs, charity jobs), were supported to set up job alerts or sign up to employment agencies. There were clients, particularly older clients, who required support in adapting to searching and applying for jobs online which the EA provided.
Once a client had found a relevant job, EAs worked with them on making an application. One client reported that the EA built them up to completing a job application gradually, initially completing an application together, then moving to the client filling in parts by herself and EA checking them, then finally the client filling in a whole application alone and asking for support where required (see case study three).
Case study 3: Anna
Anna was on long-term sick leave from her job as an events assistant due to
anxiety. Her company then went through a restructure and she felt that they had discriminated against her in this process. She is pursuing this case at an employment tribunal. Whilst this process was happening, Anna wanted to find another job and sought help from the EA in IAPT service, as she felt that her anxiety was making it challenging to complete job applications and attend interviews.
“[My anxiety] had a really bad impact on my self-esteem and my focus and
concentration as well, just, were completely shot to pieces.”
Anna found the prospect of filling in an application form by herself extremely daunting. Her EA built her up to completing a job application gradually: initially completing an application together, then moving to Anna filling in parts by herself and the EA checking it. Eventually Anna was able to fill in a whole application alone and asked for support where required.
Anna also received a range of additional support: her EA made some suggestions to further improve her CV; gave her techniques for managing panic by establishing a routine the night before and the morning of an interview; introduced methods of relaxation; conducted a mock interview with Anna; and practicing a series of distraction and refocusing techniques. Her EA and therapist worked jointly throughout her support and would discuss key points from their session (with her consent) with each other. They both discussed the idea of widening her job search to other sectors which Anna has pursued.
“The really practical stuff was very good because with my anxiety, the panic
overwhelms me and I don’t know what to do…one of my big things is tension
building the night before [an interview]. My previous response was to just spend all night preparing. I probably would get very little if any sleep, and be quite wound up, quite tense so [EA] gave me a little list of what to do instead, so instead of revising all night, actually you do one hour about 5 o’ clock and then no more, and instead of the stress and the tension, do different things like go have a relaxing bath…so an alternative routine to actually put me in a better frame of mind.”
As a result of the support Anna has continued to search for a job and is
volunteering at a local community organisation – where she recently organised a successful community day. She feels motivated to submit a few applications after each session with her EA and has felt her confidence increase. She now feels optimistic that she will find a job in future.
“A year ago, I didn’t think I could put a full stop in the right place. I have belief in my skills and experiences now and I know when I get a job I’ll be able to do it…”
Some clients were given practical advice and support on managing the interview process. This included acting out mock interviews with feedback; strategies for managing panic before and during interviews; brainstorming questions for the client to ask during an interview; and help on how to answer interview questions using the Situation Task Action Result (STAR) method.[footnote 31]
EAs were also reported to have used confidence building techniques. For example, one EA worked with a client on how to manage the disappointment of not getting a job she wanted, by discussing the positive points she could take from employers’ feedback on the interview, creating points for improvement based on feedback, and other distraction or refocusing techniques. Through this technique and wider support from the EA, she has widened her search for jobs and feels that “I now know and am accepting of the fact that the world doesn’t end if I’m not in the [sector] for a while, and I can do jobs outside of the sector as well”. The client was encouraged by her EA to secure a voluntary role and hopes to enter full-time employment in future. For many, the EA also provided general encouragement to keep going with job search and support to explore different options for employment.
Signposting and access to other services
Half of EA clients (51 per cent) received information on other local organisations/support that could help them with their employment needs such as legal advice relating to a conflict at work. This increased to 61 per cent among those out of work.
Around two-fifths (37 per cent) received information or help with Access to Work; this was slightly - albeit significantly - more common among the employed (42 per cent compared to 34 per cent of those who were out of work).
A small number of clients interviewed reported that their EA had referred or signposted them to other services, including Citizens Advice and the Advisory, Conciliation and Arbitration Service (ACAS),[footnote 32] to help build their skills or to receive support that was outside of the scope of the EA service such as legal advice relating to a conflict at work.
Education and training
Around half (49 per cent) of EA clients were given advice about the types of training they could do. This was more common among those out of work (61 per cent) than the employed (43 per cent). Although those aged 16 to 24 years old were the most likely to be offered advice in this regard (57 per cent), it was fairly common among older age groups too. For example, 46 per cent of clients aged 50+ also received this support.
In qualitative interviews, a few clients described obtaining support to access educational courses and apprenticeships, one client (employed at referral) was supported to attend a university open day.
A small number of clients noted that they had signed up for a course on the recommendation of their EA. Examples include an individual signing up to an English course with the aim of both improving job prospects and providing structure to the day, and another gaining a qualification from an eLearning Business Administration course as a result of identifying skills gaps with the EA.
Work experience
One third (33 per cent) of EA clients received advice or support in relation to volunteering, work experience or a work placement; increasing to more than half (55 per cent) among those out of work.
In qualitative interviews, clients explained that they were encouraged to apply for volunteer roles to build their skills and increase their confidence in applying for a paid role in future. Clients described applying for volunteer roles as being beneficial due to:
- Volunteer roles having similar recruitment and application processes as paid roles. This made some clients feel prepared for future applications, allowed them to familiarise themselves with this process, and increased their confidence in attaining a role in future.
- Developing work-related skills was a benefit reported by some clients, such as time management, commitment, and communication skills. Some also worked on a voluntary basis within the same role that they hoped to gain paid employment (e.g. teaching), enabling them to develop job-specific skills and relevant experience for their CV.
- Clients noted that volunteer roles set a manageable commitment that they could achieve and that it “gets me out of the house each week”, alluding to the latent benefits of employment.[footnote 33]
- Volunteer roles often had social benefits for clients, through training and volunteering with other people, making links with their local community, and interacting with people outside of their family and friends.
In work support
Two-fifths of employed individuals (40 per cent) received help to identify changes that could happen in their workspace, to help them overcome difficulties. Clients interviewed detailed examples of changes suggested, such as working reduced hours, sitting in a different part of the office, being referred to occupational health for an assessment or to make adjustments to their desk. Case study four demonstrates how an EA helped one client stay in work by support with workplace adjustments.
Case study 4: Helena
Helena is a contracts manager at a university. She initially agreed to have EA in IAPT support because she was concerned that her anxiety would affect her performance at work. She wanted support to ask for adjustments at work. Initially she thought that the employment advice would focus only on her CV but was pleased to know that her support needs were addressed:
“I guess my concern was that somebody was going to look at, want me to talk through my CV and my skillsets if you like in quite a mechanical way but it was a far more holistic approach and actually it was really quite nice to talk to somebody about where I was at and what I’d like to do. It was nice to have a reflective session.”
She felt that the EA provided positive reinforcement to remind her that she was competent at her job, and they discussed strategies she could use to manage her anxiety in the workplace.
She described receiving support from the EA in IAPT service as having “three legs to a stool, instead of one…you’ve got your own resources but they’re pretty diminished which is why you’re asking for support with the mental health issue…the counselling provides another leg and the [EA] provided a third leg of support”
Helena and her EA rehearsed a conversation in which Helena asked for adjustments at work. She then asked her manager for adjustments, such as the ability to work from home at short notice and working from home regularly:
“I had the opportunity to rehearse the conversation, to think it through and to not feel awkward, if you like, the guilt bit and the awkwardness bit had been alleviated because I’d already had that conversation once in my head and once in real life with someone and then I could have it again with my manager, which was really good.”
She has been supported to stay in employment and feels that she is able to fulfil her work commitments by having the flexibility to work from home when needed. She stated that she would not have felt confident asking for these adjustments without the support of her EA.
A small number of clients interviewed reported that their EA had offered to attend meetings at their workplace. For example, to provide support in asking for reasonable adjustments, making a formal complaint or attending an informal discussion about bullying or harassment in the workplace. All of these clients declined the offer of support with some noting that they felt able to attend the meeting by themselves.
“Although I did not take up advisers offer to attend meetings as had a union rep, [it] was good to have that offered as it takes away that feeling of being outnumbered and to have somebody that’s knowledgeable about legislation and the law as well” (Male, employed off sick)
Three-quarters (75 per cent) of clients who were employed but off sick at the start of their IAPT support received advice on phased return to work. Qualitative interviews revealed how many of these clients also sought emotional support from their EA, for example by discussing feelings of isolation from being out of the workplace for a long time.
Confidence building, emotional and motivational support
Clients also received support with softer skills. Clients who were in work described receiving support with motivation and focus in their current job, such as EAs advising clients on how to:
- Set short terms goals
- Prioritise work activities
- Keep a diary to monitor their motivation levels, record achievements and notice patterns in behaviour.
EAs also provided emotional support to some clients, through positive reinforcement of their abilities, encouraging them to stay with their employer where appropriate and reassuring the client that they would work together to address the difficulties with their employer. EAs provided advice on how to start difficult conversations with employers, for example, asking for adjustments at work through role play exercise.
Communication with employers and related agencies
In the five-month survey, EA clients were asked whether their adviser had contacted any of the following on their behalf:
- Their trade union
- Jobcentre Plus (JCP)
- Their current employer (or employer at the time)
- A potential employer or employers
- An employment agency or agencies
Around one-sixth (17 per cent) of clients stated that their EA had contacted at least one of these stakeholders. Most commonly, EAs contacted potential or current employers – each had been contacted for eight per cent of clients. An employment agency was contacted for five per cent of clients, the JCP for three per cent, and a trade union for one per cent.
Other types of support
A small number of clients interviewed reported that EAs had provided them with wider support, such as how to apply for DBS check (Maria’s case study, Chapter 4 page 102), completing forms for a Personal Independence Payment claim, how to find alternative housing, and mindfulness exercises and applications.
3.3. Client views of the EAs in IAPT service
Overall, views on sessions with EAs were very positive. Around eight in ten (78 per cent) EA clients agreed that the sessions had been useful, answering either 4 or 5 on a five-point scale. Half (51 per cent) rated the sessions as ‘very useful’. Only a small minority (seven per cent) felt the sessions were not useful, answering 1 or 2 on the same scale.
Figure 3.2 Usefulness of EAs in IAPT sessions
| Usefulness | Percentage |
|---|---|
| Not at all useful | 2% |
| Fairly useful | 5% |
| Neither not useful or useful | 14% |
| Useful | 28% |
| Very useful | 51% |
Base: Wave 1 time 1 survey - All those who received support from an EA (1,056)
Clients who were employed but off work sick on entry to IAPT services were more likely to have found EA sessions useful (84 per cent, compared to 75 per cent of clients employed and working, and 76 per cent of those looking for work).
These findings were supported in qualitative interviews with clients, in which views of the EAs in IAPT service overall were overwhelmingly positive. In particular, the following features of support received were commonly highlighted:
- Flexible support
- EA advisers being friendly
- EA advisers providing independent, non-judgmental advice
- Clients receiving tailored support
- Having a balance between practical, emotional and motivational support
These points are explored further below, with differences between the three main client groups (looking for work, employed and in work, and employed and off sick) highlighted where applicable.
Flexible support
Across all three key groups, clients interviewed reported that the support they received from the EA was flexible. This started from the point of referral, with clients commenting that they were offered an appointment in a location of their choice or close to home, without the need to travel very far. This set the tone for the rest of the appointments, with some reporting that the service was centred around their needs.
Others commented that they felt that the service dealt with them as a whole person, for example by allowing them to rearrange meetings potentially at short notice if they had caring responsibilities.
The option to have support by phone and email as well as face to face was also valued by clients in all three groups. Many clients started with face to face support once a week and then moved to telephone calls every two weeks, with emails in between if needed. The range of support modes was valued by clients as it reflected their differing needs as the sessions progressed, enabling them to reduce the intensity of support as they increased in confidence, and was flexible to the needs of the client.
“I like the fact that I could speak to the people within the service either over the phone or via email or face to face, that there wasn’t that pressure on you can only do so at this certain time in this building. That was one of the main benefits that I would say that they should try to keep.” (Male, employed on referral)
Some clients also reported that they felt they could keep in constant, or at least regular, contact with their EA by email. This allowed the client to flag issues as they occurred in the week, and for the EA to answer quick questions without the client having to wait for their weekly session. This was particularly useful for those who had been offered an interview for a job (potentially at short notice) and required reassurance beforehand.
Friendly advisers
Clients interviewed from across all groups emphasised that their EA was friendly, kind and that they got on well with them which made them feel at ease.
Some clients said that meeting with their EA felt like talking to a friend who would listen to their experiences, but with the ability to encourage but also constructively challenge more effectively than friends or family:
“Somebody to talk to that was like I say impartial…to be given some positive encouragement that actually no its not me…and also if I said something that he didn’t agree with then he’d tell me, so it wasn’t someone just nodding along.” (Female, employed on referral)
EAs were also described as being good listeners, who were calm, patient and kept their promises – such as keeping scheduled appointments, running to time, and sending further information by email when they said they would.
“She was lovely…very good, very calm, very patient with me…And always phoned when she was meant to, and all of that…Very professional, kind, [a] good listener… She could work out the situation, and almost kind of sum it up back to me quite well. And quite, yeah, she got a grasp of the situation very quickly I think. And was sensitive, or kind around it all, so kind of got an idea of what tone to bring to our meeting I think.” (Female, out of work on referral)
Very few clients interviewed differed from this view – however, one client felt that her EA could have spent the first face to face session getting to know more about her hobbies and interests, rather than looking at job adverts straight away.
Independent, non-judgmental advice
EAs were valued for their independent status. This was mentioned particularly by clients who were off sick and those who had a dispute with their employer, these clients valued the opportunity to speak to someone independent about the specific issue or dispute. For some, this encouraged them to be more open with the EA and to share the depth of their feelings and experiences without any negative repercussions.
“It was nice to talk to somebody completely outside of employment… It comes without judgement or any risk of it filtering back, sense of complete confidentiality and felt I could be more open and not feel embarrassed.” (Female, employed on referral)
Support from EAs was often contrasted with other forms of support, for example that available through their workplace human resources (HR) department or union representatives, which tended to be perceived as less independent. EAs were also contrasted to recruiters or agencies, who clients felt were more interested in getting candidates into any job, regardless of whether it suited their preferences, goals or ambitions. EAs were described as non-judgmental in contrast to friends and families as they didn’t ‘bring any history’ or bias to the table. Some clients felt reluctant to ‘burden’ their family and friends and felt relieved that they were able to talk to someone without feeling this pressure.
However, some conceptualised the EA as being “on their side” which contradicts the notion of EAs as independent. Nonetheless for some, this was particularly important as they felt supported by someone had an interest in their concerns, feelings and needs. This sense of support was particularly the case for those who were employed and working or employed but off sick, potentially as they did not feel that their current employer supported them in this way.
Tailored support
In both the qualitative interviews and the survey, EA clients felt that advisers both understood their needs, and adjusted support accordingly. As shown in Figure 3.3, the vast majority of EA clients – 92 per cent – felt the adviser was understanding of their needs, and four in five (82 per cent) felt that the support was tailored to their needs.
Figure 3.3 EA client views on how understanding and tailored support was
| Understanding/tailored to needs | Strongly disagree | Disagree | Neither disagree or agree | Agree | Strongly agree |
|---|---|---|---|---|---|
| Adviser was understanding of my needs | 1% | 1% | 6% | 16% | 77% |
| Support I got was tailored to my needs | 3% | 4% | 11% | 25% | 57% |
Base: Wave 1 Time 1 survey - All those who received support form an EA (1,056)
In keeping with these findings, clients interviewed from across the three key groups commented that the support they received from EAs was relevant and tailored to their needs. Clients described EAs taking the time to understand their specific needs and offering a range of support that could meet them. They were able to identify which methods of support would be more beneficial, even if the client could not recognise this themselves.
“They obviously know their craft very well and they can tell me areas to look at and things that I haven’t thought about. I think, to be fair, if you go in with an open mind, they’re quite good at helping you and tailoring what you may need even though you didn’t know you needed it, if that makes sense?” (Female,employed on referral)
Some clients, particularly those who were out of work, reported that they did not feel pressurised into accepting the first job that came their way. The process of finding a job was described as being collaborative and centred around conversations with the EA about their interests, skills, abilities and desires.
“He found jobs suitable for me. Not just a job, but a job that’s suitable for me. He didn’t go, oh, there’s a cleaner’s job here. He found the jobs that were suited to what skills I had, and, kind of, took into account of how far I could travel, and my situation basically.” (Female, employed on referral)
For those who were employed, they felt that the EA tried to find jobs that were suitable to their skill level and career goals.
“It felt tailored to my situation, it didn’t feel like there was a lot of tick boxes that had to be ticked, as in, I have a CV, I have these skills. That’s the kind of level I’m at, therefore I am matched with these kind of support mechanisms or services. It felt far more flexible than that and therefore much more useful.” (Female, employed on referral)
Balance between practical, emotional and motivational support
Many clients interviewed across the three groups, commented that the support provided was the right balance between practical, emotional and motivational support and that the combination of these three elements was key to achieving positive employment, health and well-being outcomes (outcomes are explored further in Chapter 4 and 5).
For some, the balance of these three forms of support also demonstrated that their mental health condition and/or needs were taken into account by the service; this was a key point of difference compared to general employment support services.
Some clients mentioned that they could find support for their CV and job search elsewhere, but that the EA also enhanced their well-being which was equally important. The following quotes are from a client who had used the EA in IAPT service twice, exemplifies how she valued the support received.
“There was a side of helping me look for and gain employment and in the case of the second time round, looking for career advancement and there’s another side where I see them as friends and its nice because they seem to care about my well-being and how I am and they would remember personal details even from
the first time I came and ask about that.”
“Even when they would check up on me to see how I have been getting on, part
of it is about checking my progress but part of it is also about genuinely seeing how I am at the same time” (Female, out of work on referral)
Others felt that the practical employment support was ultimately the most important aspect, but that the emotional support encouraged them to come back to the service for sustained support.
“Ultimately the practical side is more important. I am going to them for a reason that is I do have a goal in mind…but I think what I found there was the level of personal care they provided was…like an added bonus, it was just really nice and I think that’s actually the reason I kept going back to them because I have a good relationship with them and I have a level of trust…I trust their opinion and I respect what…critiques they have on my applications.” (Female, out of work on referral)
Some clients, mostly those who were out of work on referral, were motivated to continue job searching whereas they felt that they would have given up if they had been on their own.
For some, having a structured session with goals and milestones over time was motivational. Combined with confidence building from the EA and therapist, this encouraged some clients to have a more positive outlook on their employment prospects and their future in general.
How support concluded
As there were no set limits or guidelines for how long EA support should last, the length and intensity of support varied between providers and sites.
For many clients who were out of work on referral or who were in employment but were seeking a new employer, the EAs in IAPT support stopped once they found a job. In most cases this was mutually agreed between clients and EAs and for many the employment support phased out over time by moving from weekly face to face sessions to fortnightly, or moving to telephone catch-up calls every few weeks or months to check in. However, in a few cases clients reported being told that they had to stop EA support once their counselling ended.
“I’m still struggling at times because, yeah, both of them [therapy and EA support] finishing at the same time was quite a lot.” (Female, employed on referral)
However, at the end of their EA support, many felt reassured that they could get back in contact with their EA, should they require further support in future.
“What I liked most about the service is that I’ve still got that support, as long as I need it.” (Female, out of work on referral)
Integration within the IAPT service
As outlined in the introduction, a key feature of the EAs in IAPT delivery model was that it is an integrated service that brings together employment advice and support with IAPT provision. Therapists and EAs are expected to work collaboratively to deliver a personalised service to clients based on their individual needs.
The extent to which clients felt the support was integrated, and their resulting experiences, were explored in the qualitative interviews. Some clients noted that the support provided by different services (GP, IAPT service and EAs in IAPT) addressed their support needs holistically.
“There was overlap, it just went, when I finished with the telephone [support from IAPT service] then I had the face to face [support from EA] for the next purpose and it was like a continuation of that fortnightly cycle.” (Female, out of work on referral)
‘[The integration] definitely was [a benefit]. I felt that the whole thing, I was obviously seeing my GP as well, the one to one [therapy] and the work support, it all seemed quite holistic and joined up.” (Female, out of work on referral)
Some clients described a benefit of their therapist and EA working together as not having to repeat themselves multiple times. For some, there was a sense that the different elements of the support enhanced each other which created a ‘continuous cycle’ of support. For others, the support from their therapist and EA was experienced as distinct, but the client was able to ‘knit’ learning from these strands together.
“Employment adviser was practical counselling and counselling was the mental side so I could knit the two together.” (Female, employed on referral)
At the initial introduction stage, one client stated that their EA had had a discussion with his therapist prior to contacting him. This meant that the EA understood his specific needs from the outset and was able to provide tailored examples of how the EAs in IAPT service could help him during an initial telephone call. This also avoided the necessity of having to repeat details of his mental health and employment history, which as he explained could have been intrusive and unwanted:
“It wasn’t a blind call, as it would be with somebody who didn’t know anything about my history or anything like that. Sometimes, it [can be] an inconvenient time that somebody’s asking you personal questions. So, at least he understood my background and what was going on and what I actually wanted out of the system to then call and say, look, I can do X, Y and Z, come down and see me and then we can take it from there.” (Male, out of work on referral)
Others noted being aware of the two parts of the service working together during their employment support. For example, in one instance, a therapist and EA worked together with the client to think through workplace scenarios, including meetings and presentations, to help reduce anxiety experienced by the client. Others reported that their therapist and EA kept each other informed of relevant information:
“There were a few occasions where I emailed one or I spoke to one about something and they said they would let the other one know and by the time I saw the other one, they knew about it. So, I didn’t get the feeling that they were talking behind my back, but I did feel that they did communicate, so I found that a positive thing, not a negative thing.” (Female, out of work on referral)
This reinforces the finding from the process report that the co-location of EAs and IAPT therapists allows for closer collaboration between the two groups, showing benefits for clients.[footnote 34]
The complementary nature of the EA support and therapy is illustrated in case study five.
Case study 5: Alicia
Alicia worked in HR for a large company. She experienced anxiety related to her job as she felt that she was “living and breathing work” with little room for anything else. This was having an impact on her family life, her mood and physical symptoms such as headaches, as well as a loss of focus:
“I felt like a robot, I was doing things because I had to. I was working for the sake of working, I wasn’t enjoying it anymore…I was losing a bit of focus, I was here, there and everywhere and I ended up not being in control, [which is a] big thing for me as I like to be in control.”
The EA focused on unpicking why Alicia’s job was having a big impact on her life, and how she could improve the way she felt at work. She also had cognitive behavioural therapy (CBT) at the same time, which was focused on her overall well-being. Alicia felt that these two aspects of the service complemented each other.
Through CBT she recognised that “sometimes I just can’t control things, so I need to focus on what I can control which is my job”. She felt that the CBT allowed her to change her mindset to be more positive about her time at work. Through the EA support she made the decision to leave her current employer and found a temporary role at another HR company. She was then able to take two weeks’ holiday to rest which Alicia felt was a major milestone and something she had not been able to do without support. She has now accepted a permanent contract at the same company and feels that both parts of the service helped her to avoid burnout and to stay in employment.
3.4. Client views of EA service value
Overall, 57 per cent of EA clients reported that the support was valuable in helping them with staying in, returning to, or finding work. As shown in Figure 3.4, individuals who were employed when they started receiving IAPT support were more positive than those looking for work. Pointing to the value of in-work support, two-thirds (67 per cent) of clients who were employed but off sick agreed that the EA service had helped them return to work, and around three in five (57 per cent) clients who were in work agreed it helped them stay in work. This compares to around half (49 per cent) of those looking for work agreeing the service had helped them find work.
Figure 3.4 Agreement that employment support helped clients to achieve their intended employment outcomes
| Employment outcome | Strongly disagree | Disagree | Neither disagree or agree | Agree | Strongly agree | % agree |
|---|---|---|---|---|---|---|
| All (1,056) | 12% | 7% | 14% | 18% | 39% | 57% |
| Stay in work (employed and in work) (380) | 11% | 7% | 14% | 19% | 39% | 57% |
| Return to work (employed but off sick) (312) | 9% | 4% | 11% | 17% | 50% | 67% |
| Find work (out of work and looking for work) (329) | 18% | 9% | 16% | 19% | 29% | 49% |
Base: Wave 1 Time 1 survey - All those who received suppoprt from an EA (as shown)
Through qualitative interviews clients were able to identify which features of the EA support that they found particularly helpful and would want to keep in the service moving forward.
Clients reported the following aspects of the structure and method of the sessions as beneficial. Firstly, face-to-face support was a key aspect. It allowed clients to practice their communication skills, and for some it was the rare time they interacted with someone outside of family and friends, while for those who were socially isolated it was the one time a week when they had a reason to leave the house. Some clients reported looking forward to these sessions and that it gave structure to their week. Secondly, the regularity and consistency of sessions was beneficial, with the ‘keeping in touch’ calls between face-to-face sessions or after months of support making them feel accountable to someone.
As noted above, the balance between practical, emotional and motivational support was also a key aspect. Clients noted that EAs understood their mental health needs and that they valued not having to defend or explain these. Some felt motivated to fill in application forms and apply for jobs after each session.
For some, the sessions provided career/employment advice and support for the first time in their adult life and enabled them to think more broadly about what they might do as a job. The EA provided a view on ‘what was out there’ – opening up possibilities and widening horizons with regard to employment opportunities that helped people move from a fixed idea of limited choice.
The EA helped them to challenge their thought processes or assumptions and supported them to identify and recognise skills and experience. This helped to boost feelings of self-worth, increase motivation and generally help people to ‘feel good’ about themselves. For some it was felt this led to a mindset shift from it being ‘impossible to find work’ to searching for and gaining employment. For others, this gave them a sense of control in times of crisis, and the confidence to tackle one aspect of their lives in a structured way.
At the point that the employment status of the client had the potential to change they did not feel pressurised into accepting a job offer or going back to work. Rather the service enabled them to move at their own pace and not to take too much on too soon, which for some could have put them ‘back at square one’ by increasing their anxiety, overwhelming them or reinforcing the idea that they cannot cope in the workplace.
After their employment status had changed, many clients commented that the support did not stop which made them better able to sustain work. Others noted that the EA provided them with resources which they will use in future if they change jobs.
3.5. Areas for improvement
Although the majority of clients interviewed were positive about the service they had received, some offered suggestions for service improvement:
- As noted previously, a small number of clients noted that they would have liked to receive employment support for longer.
- One client mentioned that earlier access to the service should be encouraged before going off sick or before mental health has become problematic.
- A number of clients interviewed were unsure of the scope of the service, and how it might help them. Some examples of client confusion include: that the EAs in IAPT service would provide support to follow-on from the therapy sessions they had just finished; that the focus would be on gaining paid employment only; uncertainty about whether the service would be able to help them to reduce their hours or potentially leave employment altogether.
- A number of clients described “not knowing what to expect”. The unknown may be off-putting to some, particularly those who struggle to speak to strangers or experience anxiety. Lack of upfront information may have been an issue specific to the early stage of programme roll out. To avoid this being a persistent issue, services could consider making the scope and purpose of the service clearer to clients in their offer of referral.
- A few noted possible practical improvements to the setting of the sessions they felt would make them feel more comfortable to attend, for example, holding the sessions in a more relaxed environment (e.g. a coffee shop, or away from health services such as drug and alcohol treatment services).
- In terms of additions to the range of support, one client suggested a support group for people who are job searching as “looking for a job can be very isolating”.
- Another suggested it would be beneficial if EAs in all areas were; “engaging directly with employers and asking if they would take people on for work trials, voluntary work”, for example by building contacts with local employers and training providers as these activities were not widespread across all EA in IAPT sites.
4. Longitudinal outcomes for clients who saw an Employment Adviser
This chapter describes gross outcome changes[footnote 35] five and 12 months after entry to the Improving Access to Psychological Therapies (IAPT) service for clients in Wave One areas who saw an Employment Adviser (EA). It explores the longitudinal experiences for clients who took part in both surveys, measuring change in their employment, health and well-being status over time, from entry to IAPT to the fivemonth and 12-month point where available, and from the five-month to the 12-month point where no entry point data was collected. As throughout the report, all cited subgroup differences reported are significant unless explicitly stated otherwise.
It is important to note that gross change explored in this chapter is not necessarily attributable to the EAs; some may be attributable to the therapists, and some would have occurred without any intervention. On starting IAPT services most clients would be at a fairly low point, so some improvement over time for a proportion is to be expected. Estimates of the additional impact of seeing an EA, over and above IAPT support more generally, can be found in Chapter 5 where outcomes of EA clients have been compared to a constructed counterfactual.
Chapter summary
* More than two-thirds of EA clients surveyed experienced a positive
employment outcome – either staying in work, returning to work from sick
leave or moving into employment - in the time between entering IAPT
services and approximately 12 months later.
* Most clients who were working on entry were still working at 12 months. The
majority of these clients experienced positive in-work changes in this time, for example, greater job satisfaction and enjoyment, improved work relationships, or adjustments to their job role or hours to suit them better. The majority of clients (74 per cent) attributed these changes (at least in part) to support received through IAPT and EA services.
* Around seven in ten clients who were off sick from work when they entered
the IAPT service had returned to work by 12 months, although fewer than half
returned to the same role.
* Presenteeism (i.e. productivity loss in work due to health problems)
decreased for most clients who were employed on entry to IAPT and still
working 12 months later.
* Half of clients who were looking for work on entry to IAPT had found
employment 12 months later.
* Among those out of and looking for work at 12 months, many felt able and
wanted to return to work. Job search activity was relatively high within this
group, both in terms of the range and frequency of job search activities.
However, concerns relating to health and work (such as the idea of work
making individuals anxious) were common, and only a minority felt confident
in finding work. Furthermore, confidence and motivation decreased over time,
from five to 12 months after entry to IAPT services.
4.1. Overview of employment status over time
As shown in Figure 4.1, approximately five months after entry to the service employment among EA clients had increased by five percentage points, to 72 per cent and the proportion in employment was maintained at the 12-month point.
There was a substantial positive shift within the employed group, with the proportion of individuals off sick from work reducing from 30 per cent to just five and four per cent at five and 12 months (respectively).
The proportion of unemployed clients looking for work decreased by five percentage points between IAPT start and five months later (from 31 per cent to 26 per cent), and by a further six percentage points by 12 months. In this time, the proportion of retired individuals or those not looking to work in the future, increased by five percentage points.
Figure 4.1 Employment status of EA clients at IAPT start, and 5 months and 12 months after IAPT start
| Employment status | IAPT start | After 5 months | after 12 months |
|---|---|---|---|
| % employed | 67% | 72% | 72% |
| Employed and working | 36 % | 66% | 67% |
| Employed, off sick/other | 30% | 5% | 4% |
| Looking for work | 31% | 26% | 20% |
| Retired/not looking to work in future | 3% | 2% | 8% |
Base: All Wave 1 EA clients who completed the Time 1 and 2 surveys (712)
Relative to the type of employment on entry to IAPT services, a slightly higher proportion stated that they were working part-time for an employer at 12 months (28 per cent of all employed at 12 months compared to 24 per cent of all employed on IAPT entry); the proportion stating that they were working working full-time decreased slightly from 70 per cent to 66 per cent. The proportion in self-employment was broadly unchanged between the time points (five per cent on IAPT entry compared to seven per cent 12 months later). Individual changes in employment status over time Underlying these longitudinal shifts in employment was a positive employment outcome for more than two-thirds (68 per cent) of EA clients:
- 31 per cent had remained employed and in work;
- 16 per cent had moved into employment; and
- 21 per cent had returned to work after being off work (either for health or other reasons such as maternity leave) on entry to IAPT.
Among clients who did not experience the above positive employment outcomes, one in ten (10 per cent) had moved out of employment, while 18 per cent remained unemployed. A very small minority had either remained employed but off work (three per cent) or moved from working to being on sick leave (one per cent).
Figure 4.2 shows the proportion experiencing any positive employment outcome by gender, age group and health. Overall, positive outcomes were significantly more likely among:
- Women (70 per cent compared to 64 per cent for men);
- Clients aged 34 or younger (73 per cent compared to 65 per cent aged 35+); and
- Clients without a long-term health condition (78 per cent compared to 63 percent).
Figure 4.2 Proportions of EA clients with a positive outcome at 12 months, by gender, age and health condition
| Gender | Percentage |
|---|---|
| Men (281) | 64% |
| Women (431) | 70% |
| Age group | Percentage |
|---|---|
| 16-24 (106) | 70% |
| 25-34 (141) | 76% |
| 35-49 (247) | 68% |
| 50-59 (172) | 65% |
| 60+ (46) | 48% |
| Health condition | Percentage |
|---|---|
| Long-term health condition (473) | 63% |
| No long-term health condition (239) | 78% |
| Demographic | Percentage |
|---|---|
| All (712) | 68% |
Base: All Wave 1 EA clients who completed the Time 1 and 2 surveys (as shown)
Differences in the proportions of each group experiencing a change in employment status largely reflect differences in employment status when entering IAPT (as outlined in Section 2.3). For example, EA clients with long-term health conditions were less likely to have returned to work (17 per cent, compared to 29 without a longterm health condition). However, this group were less likely to have been off sick at IAPT start. Variations by demographic characteristics that do not seem to be driven by difference in employment status at entry included:
- Individuals with a long-term health condition being twice as likely to have moved out of employment (12 per cent compared to six per cent without a long-term health condition).
- Women being more likely to have returned to work after being off work sick (24 per cent compared to 17 per cent).
4.2. Outcomes for those working on entry to IAPT services
Stayed in work
The vast majority (87 per cent) of EA clients who were employed and working on entry to IAPT services were still working 12 months later. For two-thirds (66 per cent) of clients, this was in the same role that they were working in on entry to IAPT.
Motivation and confidence to stay in work among clients who had remained in work over the 12-months period was high. Both five and 12 months after IAPT start, around three-quarters of this group felt motivated to stay in work (75 and 74 per cent, respectively). Similar proportions felt confident they would do so: 77 per cent at five months and 78 per cent at 12 months.[footnote 36]
The following subsections explore whether these clients experienced positive changes in work and, where possible, when these changes occurred and the extent to which clients attribute in-work outcomes to support from EAs in IAPT services.
Note that these subsections provide a descriptive exploration of changes over time for these clients, and subjective opinions on the extent to EA support played a role in these; Chapter 5 explores evidence for an additional effect of receiving EA support on related outcomes using a counterfactual.
Positive changes in work
The vast majority of this group (91 per cent) had experienced at least one positive outcome at work during this time. As shown in Figure 4.3, the most common positive changes that clients had experienced were “softer” outcomes, relating to experiences of work, and workplace adjustments and relationships. Most commonly, clients stated they were enjoying their job more (59 per cent). More than half of EA clients had adjusted their hours to suit them better (55 per cent), were getting more job satisfaction (55 per cent) or had better relationships with colleagues (52 per cent). Similar proportions had adjusted their job role (49 per cent) or working environment (46 per cent) to better suit their needs.
“Harder” outcomes such as those relating to job level, pay and prospects were less common but still present. Just under two-fifths felt their future pay and promotion prospects had improved (39 per cent) or had experienced an increase in pay rate, salary or income (38 per cent). A small minority – seven per cent – had been promoted in this time.
Figure 4.3 In-work changes experienced between IAPT start and 12-month
follow-up survey
Experience of work
| Experience | Percentage |
|---|---|
| You are enjoying your job more? | 59% |
| Are you getting more job satisfaction? | 55% |
| Your employer has a better understanding of how to maximise the contribution you can make at work* | 48% |
Adjustments to job role
| Adjustments | Percentage |
|---|---|
| You have adjusted your working hours to suit you better | 55% |
| You have changed your roles and responsibilities to suit you better | 49% |
| Your employer has made adjustments to improve your working environment* | 46% |
In-work relationships
| Relationships | Percentage |
|---|---|
| Your relationships with colleagues have improved? | 39% |
| Has your pay rate, salary or income increased? | 38% |
| Do you have better job security? | 28% |
| You have increased your working hours? 24% | |
| Have you had a promotion? | 7% |
All in-work eperience responses
| All | Percentage |
|---|---|
| None/Don’t know | 9% |
Women who had remained in work were more likely than their male counterparts to have experienced a positive change for most “soft” work measures.
Findings also indicate that younger EA clients were more likely than older clients to have experienced positive in-work outcomes. Although true of most possible outcomes, differences by age were most prominent in relation to employer-related and “hard” job outcomes. For example, among clients who had remained in work, those aged 34 or younger were more likely to state that their relationship with their employer had improved between entry to IAPT and 12 months later (55 per cent, compared to 40 per cent of clients aged 35+) or that they had received an increased in pay rate, salary of income (51 per cent compared to 29 per cent).
Findings among EA clients who were also employed at the five-month point gave some indication of when these changes tended to occur. The majority of EA clients experiencing positive “softer” outcomes did so relatively soon after the start of IAPT support (i.e. within five months), while harder outcomes such as pay and prospects improvements tended to take longer to come to fruition (i.e. within 12 months).
To understand the perceived role of IAPT and/or EA support in such changes, EA clients were asked the extent to which the integrated service had contributed, if at all, to each positive outcome experienced. As shown in Figure 4.4, in most cases most clients attributed achieving the outcome, at least in part, to the IAPT and/or their EA.
Clients were most likely to state that adjustments to job roles/responsibilities and working hours could be directly attributed to the service (27 and 26 per cent, respectively), although at least one in five felt the support had a direct impact on:
- Their relationship with their employer (23 per cent) or colleagues (21 per cent)
- Job enjoyment (22 per cent)
- Their employer having a better understanding of how to maximise the EA client’s contribution at work (20 per cent)
This is in line with the support and guidance many clients described seeking and receiving through EAs in IAPT services (see Section 3.2).
Figure 4.4 Extent to which patients felt the support they received through IAPT/EA was directly responsible for positive changes at work
| Positive changes | The support helped | Directly because of the support | Helped to some extent | |
|---|---|---|---|---|
| Have you had a promotion? (16) | 63% | 25% | 88% | |
| Are you getting more job satisfaction? (121) | 66% | 19% | 85% | |
| You have changed your roles and responsibilities to suit you better (108) | 55% | 27% | 82% | |
| You are enjoying your job more? (131) | 58% | 22% | 80% | |
| Your relationship with your employer has improved? (102) | 54% | 23% | 77% | |
| Your relationships with colleagues have improved? (115) | 50% | 21% | 71% | |
| Your employer has a better understanding of how to maximise the contribution you can make at work (105) | 49% | 20% | 69% | |
| Your employer has made adjustments to improve the working environment for you (102) | 51% | 17% | 68% | |
| Have your future pay and promotion prospects improved? (87) | 51% | 16% | 67% | |
| You have adjusted your working hours to suit you better (122) | 40% | 26% | 66% | |
| Do you have better job security? | (61) | 51% | 11% | 62% |
| Has your pay rate, salary or income increased? (83) | 33% | 10% | 43% | |
| You have increased your working hours? (54) | 17% | 17% | 34% |
Base: All Wave 1 EA clients who experience each psitive change at work (as shown)
Presenteeism
Another possible change explored among the employed was presenteeism; the notion that continuing to work despite illness, such as anxiety, can often result in reduced productivity.
In line with the iMTA Productivity Cost Questionnaire’s measure for presenteeism (PCQ; see Section 1.6 for more information), clients who had remained in work were asked to recall the number of days that physical or psychological problems affected their ability to work, both retrospectively for the four weeks leading up to entry to IAPT services and the four weeks leading up to their twelve-month interview. This was analysed alongside efficiency ratings for days affected (on a scale of 0 to 10, where 0 meant ‘you were unable to do any work on these days’ and 10 meant ‘you were able to do as much work as you normally do’) to calculate the productivity loss.
In the four weeks before entering IAPT services, the vast majority (84 per cent) of individuals who were employed and working (and subsequently remained in work), had experienced days where they were bothered by physical or psychological problems at work. Among those that had experienced these problems, an average of 7.25 days’ worth of productivity had been lost at that time. This equates to an average of 6.10 days of lost productivity across all clients (i.e. both those who did and did not experience problems).
Twelve months after entry to IAPT services, not only had the proportion of individuals bothered by physical or psychological problems at work in the preceding four weeks decreased to 60 per cent, but the average productivity loss also decreased to 2.86 days. This equates to an average of 1.72 days of lost productivity across all clients.
Overall, this equates to nearly two-thirds (63 per cent) of clients who were working at both time points experiencing an improvement in presenteeism, i.e. either no longer experiencing relevant problems at work or experiencing a decrease in productivity lost due to these problems. Although presenteeism had increased for around one in five EA clients (19 per cent) employed and working on entry and 12 months later.
Figure 4.5 Changes in presenteeism between IAPT start and 12 months later for those who stayed in work
| Problems in work | IAPT start | After 12 months |
|---|---|---|
| Bothered | 84% | 60% |
| Not bothered | 14% | 37% |
| Don’t know | 2% | 3% |
| Presenteeism | IAPT start - days lost | After 12 months - days lost |
|---|---|---|
| Average for all | 6.10 days | 1.72 days |
| Average for those with presenteeism | 7.25 days | 2.86 days |
| Change in productivity loss over time | Percentage |
|---|---|
| Decrease | 63% |
| Stayed the same | 7% |
| Increased | 19% |
| Don’t know | 11% |
Base: All Wave 1 EA clients working on entry to IAPT and at end of 12 months (221).
Health state may underlie the increase in presenteeism for some; clients with a poorer health state 12 months after entry to the service were significantly more likely to see a worsening (increase) in presenteeism than those whose health stayed the same or improved (32 per cent compared to 15 and nine per cent, respectively).
Furthermore, those with a long-term health condition were more likely than those without to see an increase in presenteeism over time (24 per cent compared to nine per cent). This speaks to the notion that remaining in work, although a positive employment outcome, is not always the best outcome for an individual and their health; in some cases, work may be exacerbating health issues (as outlined in Chapter 3) and for others remaining in work does not give an individual the space to recover their health.
It is important to note that we cannot determine from the data the extent to which seeing an EA impacted presenteeism for those in work, as a robust comparisongroup among those who did not see an EA could not be identified (explored in Chapter 5).
Movement out of work
A small minority - eight per cent – of EA clients surveyed who were working on entry to IAPT services were unemployed but looking for work 12 months later. Even smaller proportions had moved to sick leave or leave of another nature (two and one per cent, respectively) or retired (two per cent). Case study six shows that a movement out of employment does not always represent a negative outcome.
Case study 6: Samantha
Samantha had taken on additional responsibilities after her manager went on sick leave. Samantha felt that her workload had become unmanageable and felt under pressure from a Director of the company. She went on sick leave due to stress and accessed the EA in IAPT service for employment support. Samantha and her EA created an action plan together which detailed three employment options and the outcomes and actions associated with each. The first was to address her workrelated issue and to stay with her employer, the second was to escalate the grievance to her union, and the third was to retire and leave her employer.
Samantha found that systematically considering each option and the outcomes of each, helped her to organise her thoughts and consider the long-term outcomes of each. She eventually decided to retire from her employment and Samantha used the points in the action plan to discuss this with her employer.
Since Samantha was supported by EA in IAPT service to leave her job, she
describes that she no longer experiences anxiety.
“I wouldn’t have considered an option that leaving might be the best thing and actually it’s the best thing I’ve ever done in my life, is walk away from it…for me, the biggest thing is what you think you might want isn’t always the best thing for you. A good outcome isn’t always to go back to what you’ve been to.”
Although she has retired, she thinks there may be a point where she is able to do some more volunteering or a part-time role. As Samantha described, without intervention she feels that there would have been detrimental effects on her health and wellbeing:
“If I didn’t have [Employment Advisor] there, I think I possibly would have gone back to work, I think I might have even still been there but I think I might have been very ill, I might have been personally in a different situation.”
4.3. Outcomes for those off sick on entry to IAPT services
Returned to work
Around seven in ten (69 per cent) clients who were off sick on entry to IAPT services had returned to work.[footnote 37] It is important to note, however, that the subsequent impact chapter indicates that this change cannot be attributed to EA support. In fact, the broad pattern of non-significant results suggest that they are less likely to be employed and working after 12 months than those who receive therapy only (see Chapter 5).
Fewer than half (43 per cent) of clients who had returned to work from sickness absence had returned to the same job role.
At the 12-month point, most clients who had moved in to employment after being off sick felt motivated (84 per cent) and confident that (82 per cent) they would stay in work. These motivation and confidence levels were an increase from the five-month point (75 and 71 per cent, respectively), which may point to these clients feeling more stable in work as time goes on.
Seven in ten (71 per cent) clients who had returned to work enjoyed their work at least ‘most of the time’, with more than one-fifth (22 per cent) enjoying it ‘all the time’. A quarter (25 per cent) enjoyed their job ‘some of the time’, and a small minority – three per cent – ‘did not enjoy their ’job’.
Presenteeism
The questions relating to presenteeism (health related productivity loss) were also asked of clients who were employed but off work sick on entry to IAPT but had since returned to work, with these individuals asked to think about their productivity in the four weeks at work leading up to their sick leave (equating to their last period in work prior to entry to IAPT), and the four weeks leading up to their twelve-month interview.
This client group were more likely than those who remained in work to have been bothered by physical or psychological problems in their last period of work prior to IAPT; more than nine in ten agreed that this was the case (91 per cent compared to 84 per cent of those employed and in work). Among those that had experienced problems, an average of 8.72 days of productivity had been lost in this time, equating to an average of 7.91 days for all clients who had returned to work after being off sick (this compares to 6.10 days lost for those remaining in work).
Twelve months after entry to the service, the proportion of individuals who had returned to work in this time and were bothered by physical or psychological problems at work in the previous four weeks had decreased to less than half (46 per cent), and the average productivity loss among those experiencing difficulties also decreased to 2.62 days. This equates to an average of 1.21 days’ productivity loss for all those who returned to work, a lower productivity loss at 12 months than those who remained in work (1.72), despite starting with a greater loss before IAPT.
Overall, this equates to more than three-quarters (75 per cent) of clients who had returned to work experiencing a decrease in presenteeism. Presenteeism had increased for eight per cent of these clients. This demonstrates a greater improvement than for those who were working at both time points (63 per cent improved, 19 per cent worsened).
Figure 4.6 Changes in presenteeism between IAPT start and 12 months later for those who returned to work from leave
| Problems in work | IAPT start | After 12 months |
|---|---|---|
| Bothered | 91% | 46% |
| Not bothered | 4% | 53% |
| Don’t know | 5% | 1% |
| Presenteeism | IAPT start - days lost | After 12 months - days lost |
|---|---|---|
| Average for all | 7.91 days | 1.21 days |
| Average for those with presenteeism | 8.72 days | 2.62 days |
| Change in productivity loss over time | Percentage |
|---|---|
| Decrease | 75% |
| Stayed the same | 4% |
| Increased | 8% |
| Don’t know | 12% |
Base: All Wave 1 EA clients off sick on entry to IAPT and working at 12 months (146).
Remained employed but not working
A small minority – eight per cent – of individuals who were off sick on entry to IAPT services were still off work for health reasons 12 months later, and two per cent were off work for other reasons.
Movement out of employment
Just over one-fifth (22 per cent) of clients who were off sick on entry to IAPT were economically inactive 12 months later. This was often due to retirement (11 per cent of all who were off sick at IAPT start), although a similar proportion had moved out of work (10 per cent).
4.4. Outcomes for those unemployed and looking for work on entry to IAPT
Found work
Half of EA clients (50 per cent) who were looking for work on entry to IAPT services had found work 12 months later (note that impact findings in Chapter 5 indicate that such movement into work was more likely among IAPT clients who received support from an EA).
Found work tended to be full-time paid work for an employer (58 per cent), with the remaining one-third (33 per cent) working part-time in paid work for an employer and nine per cent becoming self-employed.
Clients who had found work within 12 months tended to be very motivated and confident to stay in work. Around nine in ten (89 per cent) felt motivated to stay in work, with 62 per cent very motivated. A slightly lower proportion – 85 per cent – felt confident that they would, with more than half (55 per cent) very confident.
Just over seven in ten (72 per cent) clients who had found work enjoyed this work at least most of the time, with one-fifth enjoying their work all the time (22 per cent). Just over a quarter (27 per cent) enjoyed their job some of the time, and a small minority – two per cent – did not enjoy their job.
Remained out of work
Half (50 per cent) of EA clients who were out of work on entry to the service had remained so 12 months later.
In qualitative interviews, those who were out of work (but looking to work in the future) 12 months after entry to the IAPT services gave the following range of reasons:
- Entering education instead. Some clients had entered full-time education after receiving support from their EA. One client described the EAs in IAPT service as the “catalyst” for seeking out higher education. His EA supported him to find temporary employment at a supermarket over the Christmas holidays. After this, and a couple of months of therapy with a private provider outside of the IAPT service, he realised that he wanted to study maths and computing at university instead of going into employment. He is now a student at university and feels more confident that he can find a job after he graduates.
- Taking voluntary work instead. Three clients in this group completed voluntary work after receiving support from their EA. Between them they volunteered at a food bank, charity shop and community centre, and one as a teaching assistant. One of these clients noted that she felt that the support from the EA helped her to feel more confident to gain a voluntary role, and she is slowly increasing her hours over time. She felt confident that she would find paid employment at some point in the future. “I think that this support has helped me keep that aim in mind and not buckle under pressure. Not get overwhelmed, and it’s keeping me focused.”
- Health reasons preventing job search. For example, one client had a combination of physical and mental health conditions which were a barrier to seeking employment. “I’ve got fibromyalgia and arthritis, so with my depression and my anxiety it’s even a stretch just to get to the benefits office.”
- Caring responsibilities. One client had become a full-time carer for her mother whose health had deteriorated.
- Lack of success in finding a suitable job. One client had found a job as a social worker with support from her EA, however, due to problems with her manager and high workloads, she subsequently decided to leave. She was working on improving her mental and physical health and planned to start looking for employment shortly. Another client, also a social worker, was looking to work in a different employment sector. She noted that after support from her EA, for every five jobs she applied for, she was offered interviews. However, she felt that her age and a lack of recent experience in her desired area of employment were together acting as barriers to receiving a job offer.
Case study seven provides detail of one client’s experience of remaining out of work.
Case study 7: Anya
Anya worked as a librarian and then on a temporary contract in a call centre. She has been unemployed since May 2018. She wanted support from EA in IAPT service to build up her confidence to apply for a voluntary role as a stepping stone to finding paid employment.
“I wanted help to get voluntary work as I don’t think I’m fit enough to get a job now at the moment as I would end up losing it because of the stress and anxiety, so I’m looking for voluntary work.”
At the same time as receiving EA support, Anya took part in a stress management course and an anxiety management course. The EA took stock of this and decided that small pieces of employment support would be beneficial, so as not to overwhelm Anya with lots of intensive support at the beginning. Anya was supported to write a personal statement at the top of her CV, to explore volunteering opportunities and received ‘keeping in touch’ calls in between face-to-face appointments with her EA.
She feels that the face-to-face support helped her to feel confident enough to apply for voluntary work, whilst the telephone calls reminded her to keep motivated with applications. She is currently unemployed and attributes that to her depression and anxiety.
“The support was very appropriate [for my needs] because I’ve got somebody who understands mental health issues and whereas other organisations might not be so understanding. What I liked most about the service is that I’ve still got that support, as long as I need it.“
4.6. Perceived ‘active ingredients’ of EA support
Among all groups, clients tended to agreed that EA support helped them achieve their employment aims. Just under two-thirds (63 per cent) of EA clients who stayed in work agreed that support from their EA had helped them do so, with more than two-fifths (42 per cent) ‘strongly agreeing’. Nearly two-thirds (65 per cent) of clients who had found work agreed that IAPT services had helped them do so, with 48 per cent ‘strongly agreeing’. More than three-quarters (77 per cent) of clients who had returned to work from sickness absence since joining IAPT felt the service had helped them to do so, with more than half (56 per cent) ‘strongly agreeing’.
Qualitative interviews gave further insight into the specific ways in which support received from EAs led to positive employment and well-being outcomes. For those who remained in employment, the key aspects of the support received were:
- Identifying coping mechanisms to deal with stress at work: This included writing down key details of their work day rather than trying to remember everything, understanding factors that are in and out of their control, and breaking tasks down into achievable micro tasks:
“I can identify the triggers now so I know when not to get emotionally involved and where things are out of my control. I now focus on things I can control, whereas before I used to take everything on and used to take everything personally and emotionally.” (Female, employed on referral) “The concept of stepping back and listing things to do, and breaking things down into microtasks instead of looking at the bigger picture and panicking…to be more reflective and calm when you have moments of huge pressure.” (Female, employed on referral)
- Support to start difficult conversations with employer such as asking for adjustments at work, carrying out a role play of how employer might respond to their request, and EAs attending meetings with employers:
“I now have the ability to ask for breaks when needed, work from home and be able to say I am just feeling mentally fragile or not resilient and need support to manage my workload and for that to be ok.” (Female, employed on referral)
- Providing useful resources such as a handbook of practical exercises on mindfulness in the workplace:
“…mindfulness is definitely something I’m using now, because it’s important to step back and look at what’s going on and understand that sometimes it’s normal to feel overwhelmed.” (Female, employed on referral)
- Advice from EA helped to set priorities and goals in work such as identifying when tasks are due and which tasks are within their job role.
- Support to reduce hours at work, for example, to improve their work-life balance:
“I can’t do 10, 12 hours a day and get up at 4 o’clock. And I’ve accepted that I’m going to do fewer hours and earn less but that’s fine I’ve worked it all out financially…It’s all positive in my eyes. My well-being and my future is what I’m looking at now.” (Male, employed on referral)
Emily’s experiences, shown in case study eight demonstrate the impact that the EA in IAPT service had on enabling her to remain with her employer.
Case study 8: Emily
Emily works as a call handler for the emergency services. She found the job very stressful and accessed IAPT service for help. She wanted to stay with her current employer but felt that she needed support to do so.
Emily felt that the most beneficial part of the support was helping her to start the conversation with her employer, to say that she was struggling at work. The EA suggested that she write a list of things she wanted to say to her employer. She assured Emily that it was fine to say that she was struggling and to ask for adjustments to be made. They then went through mock scenarios of how her employer might respond to her requests and how she could prepare for each scenario. The therapist and EA also both worked with Emily to find coping mechanisms for stress at work.
As a result of the support, her employer has been “very accommodating”, and has restricted her duties to triaging calls only. Her employer has provided her with a mentor and therapist, with the view to transition back to handling calls in future. Her work-assigned therapist is now building on developing her coping mechanisms and stress management which she started with her IAPT therapist and EA. Emily noted that “the IAPT service and the Employment Adviser were everything in helping me to stay in work”
For those who wanted to find employment elsewhere, key parts of the support were related to:
- CV writing and interview technique
- EA’s help in “widening their horizons” or opening them up to other options, industries and careers:
“I now know to research the company before applying, and to tailor my CV and covering letter to the job I’m applying for…I felt much more confident in my skills and experience than [before support from EA], so have been able to sell myself more effectively.” (Male, unemployed on referral)
“[Current job] that was entirely them, they helped me get that…[they] helped with the application and did a mock interview and they found the position for me. Without them I don’t think I would have considered applying…[EA] contacted me to make sure I was getting on with the role ok which I appreciated.” (Female, unemployed on referral)
Clients who had returned to employment noted that key aspects of the EA in IAPT support related to confidence building and emotional support from their EA such as:
- Understanding what was triggering stress and anxiety at work and how this could be mitigated such as by reducing hours or workload.
- Creating a plan with the client of hours and duties the client felt able to manage alongside confidence building to understand that they would not be expected to “do everything straight away”.
- Supporting clients to ask for adjustments. This was done by meeting with their line manager to work out a phased return to work plan. Where the client preferred to attend this meeting alone, the EA gave them an overview of what to expect. EAs also advised clients not to feel guilty when asking for adjustments, as demonstrated by this client’s experience:
“I hadn’t thought of this as a possibility prior to EA and the adviser helped to present this as reasonable thing to ask for and not feel guilty. I rehearsed the conversation with the adviser prior to discussing with my manager to help overcome the guilt and awkwardness aspect adjustments made were ability to work at home at quite short notice and on a regular basis- I think without the service I would have asked for this somewhere down the line but due to the support I don’t feel guilty and feel it’s justified.” (Female, employed on referral)
Confidence building was mainly achieved by helping to identify clients’ existing and transferable skills. Identifying job opportunities outside of their current organisation also helped them to feel less trapped, giving them alternative options should they decide to leave. This is illustrated by Jennifer’s and Agnes’ experiences below.
Case study 9: Jennifer
Jennifer worked at a childcare centre and had a period of time off sick due to stress at work. Her EA worked with her on interview technique, as she wanted to look at opportunities outside of her current workplace. This helped her to identify her transferable skills. Her EA also supported her to get specialist equipment in her workplace to help with her dyslexia.
Jennifer then decided to stay with the same company but to move locations. She felt that her manager at the new location “allowed more autonomy which meant I could be more creative in the way I worked, and I think that makes a big difference”. She now feels more confident asking for adjustments, and to voice her opinion in meetings and with other colleagues. She said that her increased happiness at work has had a positive effect on her home life.
“I have chosen not to move on but I kind of feel a little bit more like yeah I can move on and I’ve got choices and it’s my choice to still be here…it’s quite empowering isn’t it knowing you’ve got choices and what they are.”
Case study 10: Agnes
Agnes works in finance and was moved from her local council to work in a central government department four years ago. After moving location, she felt that she could not do her job anymore:
“The move from the council to [government department] felt extremely stressful and it just gradually built up until I could basically, felt like I could no longer do it”.
She was off work for 8 or 9 months with work-related anxiety and depression.
Agnes accessed the EAs in IAPT service for support with her loss of confidence at work and because she thought she might want to leave. She hadn’t written a CV in 20 years and had limited experience of using the internet to apply for jobs.
“I only knew how to search for and apply for internal jobs within the council intranet”.
Her EA showed her how to search for jobs online and helped her to create a CV.
Agnes’ felt that:
“providing support around looking for new job opportunities helped
me build confidence that I could do something else if I decided I wanted to. That lessens your anxiety about going back to work because it’s like, well if I do go back and I feel like I can’t cope with it then I could do something else. It’s not like, what am I going to do, I’m just going to be a mess forever”. She also described the EA as being “really approachable and really friendly”.
The face to face support was key, and she didn’t feel pressured into going back to her employer or accepting a new job.
Agnes had a phased return to work and noted that her line manager had been
particularly supportive and arranged for her to start with a low case load and build up to full time. She felt that she had settled back into her role “my manager seems pleased with me and has put me forward for a scheme to be involved in some projects to start developing leadership skills”, and that she did not require any further support to sustain her employment.
4.7. Unemployment and job search 12 months after entry to IAPT
Perceptions around working in the future among unemployed clients
All EA clients who were out of work but looking to work in the future (regardless of status on entry; 20 per cent of all EA clients) were asked various questions around their perceptions about returning to work.
At 12 months, just under half (46 per cent) of EA clients who were out of work felt motivated to find work, while only one-fifth (21 per cent) felt confident in doing so.
Half (50 per cent) of EA clients who were out of work at the 12-month point felt they could return to work if the right job was available, just over a third (34 per cent) were slightly less sure, stating that they could consider a return to work on some days, and 15 per cent felt their health condition/disability ruled work out as an option at that point in time.
That said, the majority (70 per cent) wanted to return to work ‘to a great extent’, and a similar proportion (68 per cent) felt they could return to work in the next six months.
All EA clients who were out of work at the 12-month point were also asked about the extent to which they agreed with various statements relating to their health and working. Work-related concerns and anxieties were quite common among this group.
Almost half of those out of work at 12 months felt anxious at the idea of work (48 per cent), and around two-fifths were worried that work would make their health condition worse (41 per cent), or lacked confidence in applying for jobs (39 per cent).
Clients were also asked whether they agreed employers could accommodate their health needs; just under half (45 per cent) agreed employers could, while one-fifth (20 per cent) felt they could not and just over a quarter (27 per cent) neither agreed nor disagreed.
Job search activity among unemployed clients and those employed but looking for work
All EA clients who were out of work at their 12-month point or employed but looking to change job roles or increase hours[footnote 38] were asked about job search activities they had undertaken in the past two weeks. Job search activities were not covered in the five-month survey hence there is no longitudinal data available for this measure.
The Finnish Institute of Occupational Health (FIOH) Job Seeking Activity Scale (Revised), a seven-item job search activity scale, was used to measure this activity.
This measures how often individuals undertake job search activities. A rating for each activity from ‘not at all’ to ‘every day’ over the past two weeks is used to create a scale from 1 (no job search) to 4 (scoring ‘every day’ on all seven items). Activity is measured using both the mean scale score and a binary variable where those scoring 1.0 to 1.6 are coded as doing ‘lower levels of job search activity’ job search and those scoring higher than 1.6 are coded as doing ‘higher levels of job search activity’[footnote 39] (for more information on this outcome, see Section 1.6).
Clients across both groups (i.e. out of work clients and those looking to change role) had a mean score of 1.7 on this scale, indicating that both were doing ‘higher levels of job search activity’ at similar levels.
The prevalence of job search activity among those looking to change role suggests that those looking to increase their hours aimed to do so by moving to a new role, rather than in their existing role. Furthermore, as shown in Table 4.3, nearly twothirds (63 per cent) of those employed and looking to change roles said they were looking for vacancies not linked to their current job or profession.
Table 4.1: Job search activity of EA clients by employment status at 12 months
| Job search activity | Employed and looking to increase hours/change role (%) | Not employed but looking to work in the future (%) | All (%) |
|---|---|---|---|
| You have been searching for job vacancies advertised on the internet/ web | 85 | 76 | 81 |
| You have been looking for vacancies not linked to your previous job or profession | 63 | 52 | 58 |
| You have been asking friends and neighbours about job opportunities | 37 | 50 | 44 |
| You have been searching for job vacancies using a smartphone app | 44 | 38 | 41 |
| You have contacted employers who have not advertised job vacancies | 14 | 22 | 18 |
| You have been looking at job vacancies advertised in newspapers | 12 | 16 | 14 |
| You have been looking for job vacancies at the Job Centre | 5 | 13 | 9 |
| Not at all | 4 | 26 | 13 |
| Base: All employed and looking to increase hours/change role and/or not employed but looking to work | 119 | 143 | 262 |
In relation to job applications and CVs submitted to job search sites:
- Out of work clients, on average, had applied to 3.6 job vacancies in the past two weeks, while the employed had applied to an average of 2.2.
- Out of work clients, on average, had submitted 1.5 CVs to job search sites in the past two weeks, while the employed had submitted an average of 1.3.
Nearly a quarter (24 per cent) of clients who were out of work had spent an average three hours or more on job search each day in the past week, while 11 per cent of employed clients looking to change role had.
4.8. Health and Well-being outcomes
All clients (regardless of their employment status) were asked a number of questions about their health and well-being. This section looks at the changes in these measures over time.
Health state
The EQ-5D-3L was used to determine health states for clients both five months and 12 months after entry to IAPT services. The measure comprises five questions, each of which asks about a different aspect of someone’s health (mobility, self-care, performing usual activities, pain and discomfort, and anxiety and depression).
Responses to the five questions can be aggregated to provide an overall health state score between 0 to 1, where a higher score denotes better health. More information on this measure can be found in Section 1.6.
Health state values were broadly aligned at the five and 12-month points (0.74 and 0.73, respectively).
Clients who were employed and working at 12 months exhibited the highest health values (0.78), followed by those looking for work (0.66). Those off work sick had the lowest (0.55).
For most clients, health states had either been maintained (31 per cent) or improved (32 per cent) between the five- and 12-month points. Just over one third (37 per cent) experienced a decrease in health state in this time. Clients who were more likely to experience a decrease in health state included those with a long-term health condition or disability (40 per cent) and clients aged 50-59 on entry to the service (44 per cent).
Well-being
Two standardised measures were used to explore well-being:
- The ONS4 Subjective Well-being measures, collected at both 5 and 12 months
- The World Health Organisation 5 Well-being Index (WHO)-5, collected at 12 months
Details on each standardised measure can be found in Section 1.6. Broadly, the ONS4 subjective well-being measure asks individuals to rate themselves on four different aspects of well-being on a scale of 0 to 10. Table 4.2 shows the mean scores across each of the statements. A higher score indicates better well-being, apart from the anxiety measure where a lower score indicates better well-being.
Table 4.2 ONS4 well-being measure mean scores, 12 months after entry to IAPT
| Level of well-being | Mean score |
|---|---|
| How satisfied are you with your life nowadays | 6.1 |
| To what extent do you feel the things you do in your life are worthwhile? | 6.4 |
| How happy did you feel yesterday? | 6.2 |
| How anxious did you feel yesterday? | 5.7 |
| Base | 712 |
Figure 4.7 shows how subjective well-being as measured by ONS4 changed for individuals, between five and 12 months after joining IAPT services. Changes over time were broadly aligned for each of the statements, with around two-fifths experiencing a worsening over time for each. This could indicate that any positive impacts on well-being that may be present shortly after the support is received are usually sustained or improved, but this is not always the case. That said, without baseline levels it is hard to determine whether there was an initial uplift in well-being among EA clients.
Across all measures, individuals who were employed but off sick at 12 months were the most likely to experience a decrease in well-being over time, while clients who were employed and working were the least likely. For example, the average score across the four statements at the five- and 12-month points indicate a decreased in well-being for 71 per cent of those employed but off sick at 12 months, compared to 50 per cent of those unemployed and 48 per cent of those employed and working (48 per cent).
Figure 4.7 Changes in ONS4 subjective well-being between 5 and 12 months
after entry to IAPT
| Well-being | Improved | Stayed the same | Worsened |
|---|---|---|---|
| Overall, how satisfied are you with your life nowadays? | 32% | 25% | 43% |
(707)
| Well-being | Improved | Stayed the same | Worsened |
|---|---|---|---|
| Overall, to what extent do you feel the things you do in your life are worthwhile? | 33% | 26% | 41% |
(704)
| Well-being | Improved | Stayed the same | Worsened |
|---|---|---|---|
| Overall, how happy did you feel yesterday? | 36% | 23% | 41% |
(709)
| Well-being | Improved | Stayed the same | Worsened |
|---|---|---|---|
| Overall, how anxious did you feel yesterday? | 39% | 20% | 41% |
(708)
Base: All Wave 1 EA clients who gave a score in Time 1 and Time 2 surveys (as shown)
The WHO-5 is a five-item measure of well-being which asks people to consider how often in the previous two weeks they have experienced particular feelings in order to generate a total score out of 25, with a higher mean score denoting better well-being.
Twelve months after entry to IAPT, EA clients had a mean well-being score of 12.2, a score on the border of ‘poor’ and ‘good’ well-being.
Engagement with health services
To explore changes in engagement with health services, clients were asked – at both five and 12 months after entry to IAPT services – the extent of their contact with the following:
- Their GP over the previous two weeks
- Mental health services, excluding IAPT over the previous two weeks
- Casualty over the previous three months
- Outpatients[footnote 40] over the previous three months (excluding straightforward ante- or post-natal visits)
Likelihood of having seen a GP decreased slightly between the five- and 12-month points - from 31 per cent to 28 per cent – but among those who had seen a GP the number of visits increased from 1.2 to 1.4.
Likelihood of contacting other mental health services also decreased slightly, from 13 per cent to eight per cent, as did the amount of contact for those who had (from an average of 1.6 times to 1.4 times in the two weeks previous).
Conversely, likelihood of attending a hospital as a patient at the casualty or outpatient department increased between the five- and 12-month points, from 18 per cent to 22 per cent. For those who had attended either outpatients or casualty, attendance was more likely as an outpatient at 12 months, with an average of 1.9 such visits compared to 0.41 casualty visits. Outpatient visits also increased between five and 12 months (from 1.7) while casualty visits decreased (from 0.6).
As shown in Table 4.3, individuals who were employed but off sick at the start of IAPT showed more positive changes over time; this group had greater percentage point decreases for the proportions who saw a GP or other mental health services, and the smallest percentage point increase for casualty/outpatient visits.
Table 4.3 Engagement with health services and 5 and 12 months, by employment on entry to IAPT
| Health service | All | Employed and working (%) | Employed off sick (%) | Looking for work (%) |
|---|---|---|---|---|
| GP | ||||
| 5 months | 31 | 28 | 37 | 29 |
| 12 months | 28 | 30 | 26 | 25 |
| Percentage point change over time | -3 | +2 | -11 | -4 |
| Other mental health services | ||||
| 5 months | 13 | 13 | 15 | 11 |
| 12 months | 8 | 7 | 7 | 9 |
| Percentage point change over time | -5 | -5 | -8 | -2 |
| Casualty/outpatient visit | ||||
| 5 months | 18 | 17 | 18 | 19 |
| 12 months | 21 | 19 | 19 | 26 |
| Percentage point change over time | +3 | +2 | +1 | +7 |
| Base: All clients in Time 2 survey | 712 | 253 | 213 | 219 |
Reasons for improved in well-being and related factors
The qualitative interviews explored impacts of EA in IAPT service on health, wellbeing and related outcomes in more depth.
Some clients interviewed reported improvements in well-being and related factors.
For some, the emotional and motivational support provided by EAs resulted in improvements in health and well-being. For others, finding employment or changing employers with support of the EA, was reported to have led to these improvements.
The most commonly reported outcome was increased sense of self-worth. This was attributed to the combination of factors already discussed, namely: working with the EA to identify existing skills; reassurance from the EA that the client was of value to current and potential employers; and positive reinforcement and encouragement to slowly build the client up to undertaking more challenging tasks.
One client felt that the EAs in IAPT service had stopped him reaching a point of crisis:
“The fear and the horror and the worry that I was at that point of low, I wouldn’t like to say what I was going to do. It just came, [EA name] just came at the very right time for me and I’m truly grateful.” (Female, employed on referral)
The following client reported multiple changes in his well-being as a result of the EAs in IAPT service:
“I’m more relaxed and I start to understand my life need[s] to continue in a positive way and I start to be more confident in my possibilities, you know, and do something with my life because in that, in the last few years I lost this confidence. So that’s very good, very good for me to meet [therapist] and after that [the] adviser, gave me more confidence in me and I started to, you know, step by step to be me, like before.” (Female, employed on referral)
Wider improvements to clients’ well-being were also reported such as:
- Reduced social isolation by changing mindset to say ‘yes’ to opportunities such as voluntary work, community groups, training opportunities
- Positive outlook on life by staying in employment, having structure to their day, and through therapy
- Increased confidence which was beneficial for their working and home life. This was achieved by EAs in multiple ways as discussed previously in the report (see Chapter 3), including but not restricted to: spending time with clients to identify their skills and abilities; starting with intensive support when applying for jobs and then decreasing this gradually to enable the client to complete application forms with minimal supervision; encouraging clients to take part in voluntary work which enabled them to familiarise themselves with application and interview processes.
Clients who were unemployed on entry to IAPT also reported that they felt empowered to find a job. One client described the EA as a “supportive hand” guiding her and building her confidence.
“The [EA] gave me the reassurance that employment needs to work for the employee as well as the employer. This made me feel empowered and like I could make choices and have preferences and that it wasn’t all about what the employer wanted.” (Female, unemployed on referral)
This client also described how the EA support had changed the way she thought about her employment options and the job searching process. This was echoed by others who were unemployed on referral, and who had, in some cases, been job searching for a long period of time. For example, one client blamed herself for not getting interviews or job offers from employers, which affected her self-confidence and led to her feeling rejected. The EA gave her feedback on her cover letter and encouraged her to think about other factors affecting her job search which positively affected her mindset about job searching:
“She brought a point back home that it’s not necessarily that what I’m writing is awful or my CVs don’t, aren’t up to scratch, it is in fact that a lot of positions are over subscribed for when they are interviewing and I am someone with not as much experience as other people may have.” (Female, unemployed on referral)
Some clients interviewed reported reduced anxiety and depression as a result of finding a job. For example, a client who was employed on referral wanted support to help stay with his employer. He reported using the stress reduction techniques (for example, counting to ten) that the EA had taught him every day at work. The client described how he had reduced anxiety and a more positive outlook on life as a result:
“I’m a lot more employable than I realised but [the support] also made me more aware of myself and what questions I am asking, I previously would be very quiet and won’t put myself forward but now I do and this was affected by my depression and anxiety. The adviser suggested to me count to ten, focus on that one person and ask your questions”
Wider benefits included improved optimism for the future partly due to having a sense of direction and areas to focus on through working with EA.
“She helped me to make firmer plans about what I wanted to do…the lady challenged me on that a couple of times, saying, maybe you don’t want to work? And that was, to me, really useful…seeing what my reaction to that was…I’m looking into teaching now. So, my goal now, thanks to [adviser] … is to get on and do that PGCE in September basically.” (Female, unemployed on referral)
Optimism around securing future employment was sometimes accompanied by reported increases in resilience. One client described how voluntary work and EA support have made her more resilient to challenging workplace situations and that this would be useful in future.
“I am more resilient to people in situations than I used to be, you know I’d just go to pieces and although sometimes…my anxiety gets to a high level…if I was in that situation over a year ago I just would have crumbled and not come out again for a while.” (Female, unemployed on referral)
Another client reported that she was more resilient when faced with rejection from job applications remained motivated to continue applying for jobs when she would have lost motivation in the past.
Some clients who were unemployed on referral experienced marked improvements in their self-reported health and well-being. For example, Maria (see case study eleven) described the support as helping her to ‘break the cycle of hopelessness’ which covered different aspects of her life. The therapy and employment support were a springboard for Maria to make wider changes in her life to improve her health and well-being. Although her employment status did not change, a reduction in social isolation and improvements in her mobility were key outcomes for her.
Case study 11: Maria
Maria left her job as a teacher eight years ago to care for her husband who had terminal cancer.
A year after her husband’s death four years ago, Maria became almost completely housebound and walked with a stick due to hip pain. She had a phobia of doctors and hospitals which prevented her from seeking treatment for her hip. She felt increasingly isolated and lonely. Maria also experienced financial difficulties due to unemployment and felt unable to renew her passport or get an DBS check which was a prerequisite for getting a teaching job. She felt restricted by her weight and struggled with her selfconfidence as a result.
“It was just a nightmare to just try and, actually, it was just too daunting to go back out. I couldn’t do, I felt like I couldn’t move…when I started at the [IAPT service] I couldn’t cross the road by myself, I couldn’t walk across a space. I just felt like I was going to fall over all the time. And to ever think that I would get a bus by myself, I would have laughed at anybody that told me that I could do that.”
Through therapist from the IAPT service, Maria was supported to get a hip
replacement and to start walking outside and taking public transport. Her therapist then referred her to the EA service to work towards finding employment.
“[The EA adviser] told me about voluntary work, and so I started getting volunteer DBSs. And I had enough about me to go, I joined Weight Watchers and got my passport in the same day, because I just needed to break the cycle of hopelessness, really. I felt hopeless. And she just helped me with my CV, she helped me with the volunteer groups. She’s just been there whenever I’ve needed her. She’s just been absolutely fantastic.”
Maria signed up to volunteer for the NHS and Help for Heroes. Neither progressed to an employment opportunity but they gave her experience in applying for jobs and attending interviews and training. She is now volunteering as a tutor for a supply teaching service for eight hours a week. She has lost four stone in weight and is now able to walk and be more active outside of her home.
“I’d got it in my head that nobody could find me work, and I was just going through the motions to be told that you’re too old and too fat…And I think the fact that [Employment Adviser] helped me to see that I could, even if it was volunteer work, and then I wouldn’t be stuck in the house so much, I wouldn’t be so lonely, I would be getting exercise, it made me think about the possibilities that were there, and the only person that could do anything about it, ultimately, was myself”
5. The impact of Employment Advisers (EAs) in IAPT
This chapter measures the impact of seeing the Employment Advisers (EAs) by comparing the 12-month outcomes of Improving Access to Psychological Therapies (IAPT) clients seeing an EA against those of a matched comparison group of IAPT clients who did not. Impact on employment, job search activity, and well-being and health is explored for two client groups: those unemployed and looking for work on entry to the IAPT service, and those employed but off work sick on entry.
Chapter summary
* Modest sample sizes, particularly in the matched comparison group, depress
the potential to observe statistically significant impacts of EA support.
Nonetheless, there is statistically significant evidence of EA support having a positive impact on those who were unemployed and looking for work when
they started IAPT.
* Those who were looking for work when they started IAPT entry are
significantly more likely to be employed and in-work after 12 months
and significantly less likely to have seen their GP within the previous
two weeks.
* For those still seeking work after 12 months, there is non-significant evidence of those who had EA support doing more job search activity and having a stronger desire to find work. However, counter to this, they also appear to be less confident that they will find work and to have lower levels of well-being than the matched comparison group (although not statistically significant).
* In contrast, while there is very little statistically significant evidence of EA support having an impact on those employed but off sick on IAPT entry: the broad pattern of non-significant results suggest that they are in fact less likely to be employed and in work after 12 months than the matched comparison group.
* Overall, the pattern of results on these clients’ well-being suggest that those who had seen an EA have lower levels of well-being after receiving the
support, but they also have (statistically significantly) lower levels of anxiety.
* It did not prove feasible to measure the impact of EA support on employed
and working clients at the time they started IAPT. To find a robust matched
comparison group for the self-selected group of those who chose to see an
EA despite being in work, notably this would require data on any health or
non-health related issues in their work.
5.1. Introduction
Overview
The previous chapter focused on the extent to which the employment, job search, health and well-being outcomes of those seeing Employment Advisers (EAs) within Improving Access to Psychological Therapies (IAPT) changed over time, comparing the short-term outcomes measured at five months with those reported after 12 months. This chapter measures the impact of seeing the EA by comparing the 12- month outcomes of IAPT clients seeing an EA against those of a matched comparison group of IAPT clients with similar pre-IAPT baseline characteristics who had not seen an EA.[footnote 41] The matched comparison group of IAPT clients who had not seen an EA was drawn from areas not yet offering the enhanced ratio of EAs (the Wave Two areas).
In line with the IAPT clients offered EA, the original intention was to measure the impact on three client groups:
1. Those not employed but wanting to work at the time they began IAPT support (for shorthand referred to in this chapter as ‘looking for work’, including those registered as unemployed and others looking for work);
2. Those employed (including self-employed) and going to work at the time they began IAPT support (for shorthand referred to in this chapter as employed and working);
3. Those employed (including self-employed) but off work for health reasons at the time they began IAPT support (for shorthand referred to in this chapter as ‘off work sick’).
However, the impact analysis reported here focuses only on those looking for work and those off work sick when they began IAPT. It has not proved feasible to identify a plausible comparison group for those employed and working (see Section 5.2) and, as such, it is not possible to estimate impacts on this group. Even for the two groups (those looking for work and off work sick) where impact estimates have been made, concerns remain that the matched comparison group may have started with different employment problems and well-being than the EA group. If this is the case the impacts reported on in this chapter may be biased, and some of the reported impacts may be spurious.
The sample sizes on which the analysis in this chapter is based on are small (see Section 1.4 for information about the challenges of consent and follow-up). For the group looking for work there are 223 people who saw an EA, but just 68 in the comparison group. The numbers are very similar for the off work sick group, with 227 seeing an EA and just 70 in the comparison group. The small sample sizes, particularly for the comparison groups, and the fact that the survey sample is not representative of the whole EAs in IAPT pilot population, limit the conclusions that can be drawn.
Outcomes
The primary employment outcome for the impact evaluation of EA support within IAPT is the propensity for an IAPT client to be employed and working after 12 months. The chapter also includes the impact on a more nuanced outcome measure dividing 12-month employment status into those employed and working; off sick; looking for work; or not looking for work.
For all employed (including both those working and those off sick) at the 12-month follow up, there are a series of secondary outcomes around job enjoyment and motivation and confidence about staying in work. There is also a measure of presenteeism at work, which relates to the notion that continuing to work despite illness, such as anxiety, can often result in reduced productivity. Reporting on these outcomes is restricted to those who were off work sick at baseline. The sample sizes are too small for similar analysis for the looking for work group.
For those looking for work at the 12-month follow up, there are a series of secondary outcomes around levels of job seeking activity and job search self-efficacy and confidence. Reporting on these outcomes is restricted to those who were looking for work at baseline.[footnote 42]
A range of outcome variables are used to measure the impact of EA support on IAPT clients’ well-being and health, including the World Health Organisation-Five Wellbeing Index (WHO-5), the Office for National Statistics (ONS) well-being questions (ONS4), the EQ-5D health status scale and use of health services.
Further detail of all the outcome measures can be found in Section 1.6.
Chapter structure
This chapter is structured into four main sections:
- Section 5.2 describes the impact study design in more detail, including the implications of small sample sizes and the infeasibility of measuring the impact of EA support on those employed and working (Section 5.2);
- Section 5.3 explains the table format and statistical testing (Section 5.3);
- Section 5.4 presents the impact estimates for those who were looking for work on IAPT entry (Section 5.4);
- Section 5.5 presents the impact estimates for those employed but off work sick on IAPT entry (Section 5.5).
Appendix C provides estimates of the impact of EA support against a ‘nonintervention’ model in Wave Two areas (that is, including the 20 per cent of clients in the Wave Two sample who had seen an EA prior to the increase rolled out for this trial). Appendix D gives details of how the matched comparison groups were generated.
5.2. The approach to measuring impact
To estimate the impact of seeing an EA, outcomes for those seeing an EA in Wave One areas are compared to outcomes for a comparison group. In this study, a comparison group has been identified from IAPT clients responding to the 12-month follow up survey in Wave Two areas, after excluding those Wave Two respondents who said they had seen an EA (20 per cent of the total). This gives an estimate of the impact of seeing an EA, relative to a counterfactual of not seeing an EA. Appendix C presents an alternative counterfactual labelled ‘Non-Intervention’. Under the nonintervention model, a proportion of the comparison group will have seen an EA. This attempts to measure the impact of the additional investment of the ‘EAs in IAPT’ pilot, with the intervention being characterised by an increased number and range of people seeing an EA but not from a starting position of zero.
For unbiased estimation of impact, the comparison group that is selected needs to have the same set of pre-IAPT characteristics as the EA group. If this condition is met, any difference between outcomes for the EA and comparison group can reasonably be attributed to the EA. If the condition is not met, then any difference might be in part an EA effect, but also might in part be attributable to the underlying differences between the two groups.
The difficulty in this instance is that there were no baseline data collected prior to clients starting IAPT.[footnote 43] Rather, the characteristics of IAPT clients were collected (for Wave One respondents only) in the Time 1 survey after five months and (for both Waves One and Two) at the Time 2 survey at the 12 month point. A few questions were added to capture respective information on employment prior to the start of IAPT, the health condition they presented with, and their level of qualifications, so these give a ‘baseline’ on some characteristics. However, no baseline information could be collected on well-being or on the level of problems that an individual was experiencing with work on IAPT entry. Furthermore, retrospective questions cannot be considered to give as reliable data as a genuine baseline survey would.
Why a comparison group for those employed and working is not feasible
This lack of comprehensive baseline data is problematic, particularly for the ‘employed and working’ sub-group. The five-month Time 1 survey in Wave One areas suggests that 59 per cent of people in this sub-group had seen an EA, but 41 per cent did not. Of those who did see an EA, 67 per cent said they took up the offer of support by an EA because they were experiencing difficulties at work. This implies that those in work and not off work sick who saw an EA were likely to have been 43 It was not feasible to carry out a baseline survey in either Wave One or Wave Two areas predominantly drawn from the group who were having problems at work and were, it is assumed, most at risk of losing their job or going off sick. For a convincing estimate of impact for this group it would be necessary to identify a comparison group from the Wave Two respondents who were also having problems at work. However, data on this were not collected. For this reason, it is not feasible to estimate impacts on this group robustly, and they have been excluded from the analysis. In addition, there is a very small group (two per cent) of respondents in Wave One areas who saw an EA but classified themselves as ‘retired or unemployed and not looking to work in the future’. For similar reasons it is not feasible to identify a plausible comparison group for these respondents, so they are excluded from the analysis in this chapter.
For the other two groups (those looking for work and those off work sick, at the start of IAPT support), there are similar problems, but for these two, plausible comparison groups can be constructed, although still with some caveats.
Identifying a comparison group for the group who were looking for work: approach and caveats
For the group who were looking for work, clearly this group were all out of work at the start of IAPT services, so not having baseline data on the level of problems being experienced at work is not an issue. For this group a matched comparison group has been constructed using the available data on baseline characteristics, namely age, gender, level of qualifications, work history, length of time unemployed before the start of IAPT, whether they have a mortgage, whether they have a partner, whether they have children, and any mental health conditions or impairments to wellbeing at the start of IAPT (anxiety; stress; depression). This gives a matched comparison that is very similar to the EA group on all these characteristics. Nevertheless, it is not possible to rule out the possibility that other, non-observed characteristics, in particular, well-being or levels of anxiety at baseline, may be different between the EA and matched comparison group. If the comparison group started from a better position than the EA group on these outcomes, then any positive impacts of the EA support may be underestimated; if the comparison group started from a worse position than the EA group, then any positive impacts of the EA support may be overestimated. Given these caveats, the estimates of impact presented in this chapter should be treated as indicative only.
For the ‘off work sick at the start of IAPT’ group, it is a reasonable assumption that the vast majority of this group will have been experiencing some problems at work, although the nature and degree of those problems may be different for those who take up EA support compared to those who do not. For this group, a comparison group has been constructed using age, gender, level of qualifications, work history, length of time off sick before the start of IAPT, presenteeism score before the start of IAPT, whether they have a mortgage, whether they have a partner, whether they have children, and mental health conditions at the start of baseline (anxiety; stress; depression). As with the group looking for work, this gives a matched comparison that is very similar to the EA group on all these characteristics. Although again, it is not possible to rule out that other, non-observed characteristics such as well-being or levels of anxiety at the start of IAPT, may be different between the EA and matched comparison group. If there are any such differences, the impact estimates may be biased. As with the looking for work group, the estimates of impact presented in this chapter should be treated as indicative only.
Propensity score matching
For the two groups where a matched comparison group has been generated (those looking for work and those off work sick) this has been achieved using propensity score matching. Essentially, Wave Two respondents who had not seen an EA who have characteristics very similar to Wave One respondents who had seen an EA are given a large (propensity score) weight, and Wave Two respondents who are dissimilar are given a much smaller weight. After applying the weights to the Wave Two respondents, the weighted data act as a matched comparison group. Further details on generating the matched comparison samples can be found in Appendix D.
5.3. Table format, statistical tests and p-values
The tables in this chapter use the same format. The tables present the results for each 12-month outcome for those receiving EA support in Wave One areas and those in the matched comparison group in Wave Two areas who did not receive EA support. Each outcome is presented in either percentages or mean scores, with the percentage point or mean score difference provided.
The tables show for each outcome the p-value significance level of the difference between the EA and matched comparison groups. The p-value is the probability of an observed difference being due to chance alone, rather than being a real underlying difference for the population. A p-value of less than five per cent is conventionally taken to indicate a statistically significant difference (p<0.05). The p-values have been calculated in the complex samples module of SPSS. Where the differences between the two groups are statistically significant (that is the p-value is less than 0.05), these are highlighted in red and with an asterisk. The term ‘statistically significant’ is often abbreviated in the text to ‘significant’.
Given the small sample sizes, the differences between the two groups (EA and matched comparison) have to be around 15 percentage points to reach significance.[footnote 44] But the text also includes discussion of patterns of impacts, notably where the percentage point difference between the EA and matched comparison group is eight or more.
The unweighted sample sizes are cited at the end of each table.
5.4. Impact on those looking for work at baseline
Employment outcomes[footnote 45]
Among those who were looking for work when they began IAPT, those who saw an EA are statistically significantly more likely than the matched comparison group to be employed and working 12 months later (Table 5.1). Half (48 per cent) of those who saw an EA are employed and working compared to three in ten (29 per cent) of the matched comparison group (a percentage point difference of 19).[footnote 46]
Table 5.1 Impact of Employment Advisers on IAPT clients’ employment status and conditions among those looking for work at baseline
| Employment status | Employment Adviser group (%) | Matched comparison group (%) | Percentage point difference | p-value |
|---|---|---|---|---|
| Employed and working | 48 | 29 | 18.9 | .015* |
| Working status | .101 | |||
| Employed and working (including on leave for reasons other than health) | 48 | 29 | 18.9 | |
| Employed but off sick | 2 | 3 | -0.9 | |
| Looking for work | 42 | 54 | -11.9 | |
| Retired or not in work and not intending to work in future | 9 | 15 | -6.0 | |
| Base: all looking for work at baseline | 223 | 68 |
Job search activity
Those who were still looking for work 12 months after starting IAPT were asked a series of questions about their job search activity and job search self-efficacy (as described in Section 1.6). Job search activity (Table 5.2) is measured by:
- The Finnish Institute of Occupational Health (FIOH) Job Seeking Activity Scale (Revised).The impact of EA support is measured using both the mean scale score and a binary variable where those scoring 1.0 to 1.6 are coded as doing ‘lower levels of job search activity’ job search and those scoring higher than 1.6 are coded as doing ‘higher levels of job search activity’.
- The number of vacancies applied for and CVs submitted within the past fortnight, with each outcome split into ‘none’, ‘fewer than five’ and ‘five or more’.
- The number of hours of job search within the past week, split into ‘less than an hour’, ‘one to two hours’ and ‘three hours or more’.
Job search self-efficacy[footnote 47] and confidence (Table 5.3) is measured by:
- The extent to which health is perceived to be a barrier to employment, dividing people into those who perceive their condition ‘ruling out’ work as an option versus those who could consider working;
- The extent to which someone wants to return to work (using a four-point scale from ‘to a great extent’ to ‘not at all’) alongside when they think this might be (from ‘within the next six months’ to ‘never’);
- Level of motivation to find work (using a five-point scale from ‘very’ (5) to ‘not at all’ (1), with those scoring 4 or 5 rated as having ‘higher levels of motivation’);
- Level of confidence in finding work (again using a five-point scale from ‘very’ (5) to ‘not at all’ (1), with those scoring 4 or 5 rated as having ‘higher levels of confidence’);
- Level of agreement (using a five-point scale from ‘agree strongly’ (5) to ‘disagree strongly’ (1)) to a series of five statements about clients’ feelings about looking for and finding suitable work, with those scoring as 4 or 5 rated as ‘agreeing’ with the statement).
In Table 5.2 those who are not looking for work at 12 months have been filtered out, with the percentages based just on those still looking for work at 12 months.[footnote 48] This makes comparison across the two groups clearer. However, it should be borne in mind that focussing just on those still looking for work means comparing the 42 per cent who were still looking for work after seeing an EA with the 54 per cent who were still looking for work in the comparison group. Given this 42 per cent are still looking for work at 12 months, despite the EA support, it is important to highlight that they are likely to be those who, on average, have more substantial barriers to re-employment than those in the comparison group. It should also be noted that the sample size for the comparison group is very small at just 41.
Although there is no statistically significant evidence of EA support having an impact on job search activity, there is a consistent positive pattern of non-significant results (Table 5.2). For instance, IAPT clients who had seen an EA but still looking for work at 12 months are more likely to report higher levels of job search activity than those in the matched comparison group (48 per cent compared to 38 per cent). They are also more likely to report submitting CVs within the past fortnight (60 per cent had sent none compared to 74 per cent of the matched comparison group) and to have done three or more hours of job search activity within the past week (29 per cent compared to ten per cent in the matched comparison group).
Table 5.2 Impact of Employment Advisers on IAPT clients’ job search activity among those looking for work at baseline
| Job activity | Employment Adviser group (%) | Matched comparison group (%) | Percentage point difference | p-value |
|---|---|---|---|---|
| Job search activity scale | .343 | |||
| Higher levels of job search | 48 | 38 | 10.0 | |
| No or lower levels of job search (or missing data) | 52 | 62 | -10.0 | |
| Number of vacancies applied for | .631 | |||
| Five or more | 18 | 21 | -3.1 | |
| Fewer than five | 24 | 16 | 7.4 | |
| None | 58 | 62 | -4.3 | |
| Number of CVs submitted | .225 | |||
| Five or more | 9 | 10 | -1.6 | |
| Fewer than five | 31 | 16 | 15.1 | |
| None | 60 | 74 | -13.5 | |
| Job search hours | .056 | |||
| Less than an hour | 39 | 54 | -15.5 | |
| One to two hours | 32 | 36 | -3.3 | |
| Three hours or more | 29 | 10 | 18.9 | |
| Base: All looking for work at baseline and follow up | 93 | 41 |
The pattern of evidence on job search self-efficacy and confidence is more mixed (with, again, none of the impacts reaching statistical significance) (Table 5.3). As with Table 5.2, those not looking for work have been filtered out, and the percentages are based just on those still out of work at 12 months.
Those receiving EA support appear to be more likely to think that they could consider entering work than the matched comparison group (85 per cent compared to 77 per cent) who, in turn, are more likely to think that their health condition rules out a return to work (23 per cent compared to 15 per cent). Those receiving EA support are also more likely than the matched comparison group to have a strong desire to want to return to work (would like to work ‘to a great extent’ or ‘to some extent’) within the next six months (61 per cent compared to 45 per cent). They are also less likely to agree with a statement that ‘I am worried that working could make my health condition worse’ (41 per cent versus 51 per cent) and more likely to agree that ‘I think employers could accommodate my health needs’ (44 per cent versus 35 per cent).
However, despite non-significant evidence that those who received EA support were more likely to want to enter work than the matched comparison group, they appear less confident that they will find work. They are less likely than the matched comparison group to rate themselves as having higher levels of confidence in finding work (18 per cent compared to 35 per cent). They are also more likely to agree with the statement ‘I don’t feel confident about applying for jobs’ (38 per cent compared to 25 per cent). This may partly reflect the fact that those still looking for work at 12 months in the EA support group are likely to be a harder to help group. Although it may be that having seen an adviser but still not having found work may reduce confidence.
Table 5.3 Impact of Employment Advisers on IAPT clients’ job search selfefficacy and thoughts on entering work among those looking for work at
baseline
| Thoughts on entering work | Employment Adviser group (%) | Matched comparison group (%) | Percentage point difference | p-value |
|---|---|---|---|---|
| Whether feels able to return to work | .322 | |||
| Health condition rules it out | 15 | 23 | -7.8 | |
| Could consider going into work or reports currently being in work[footnote 49] | 85 | 77 | 7.8 | |
| Whether and when wants to return to work | .102 | |||
| Yes, to a great or some extent, within six months | 61 | 45 | 16.4 | |
| Yes, to a great or some extent, within 12 months | 18 | 13 | 5.6 | |
| Yes, to a great or some extent, not within 12 months | 15 | 27 | -12.1 | |
| Does not want to return to work or only a little | 5 | 15 | -9.9 | |
| Motivation to find work | .939 | |||
| Higher level of motivation | 45 | 44 | 1.1 | |
| Lower level of motivation | 55 | 56 | -1.1 | |
| Confidence about finding work | .053 | |||
| Higher level of confidence | 18 | 35 | -16.5 | |
| Lower level of confidence | 82 | 65 | 16.5 | |
| % agreeing or agreeing strongly that | ||||
| “I am worried that working could make my health condition worse” | 41 | 51 -10.0 | .325 | |
| “The idea of working makes me feel anxious” | 48 | 45 | 3.5 | .718 |
| “I think employers could accommodate my health needs” | 44 | 35 | 9.3 | .362 |
| “I don’t know what suitable jobs are available” | 39 | 31 | 7.4 | .464 |
| “I don’t feel confident about applying for jobs” | 38 | 25 | 13.1 | .145 |
| Base: all looking for work at baseline and follow up | 93 | 41 |
Well-being and health outcomes
Among those who were looking for work on IAPT entry, there is very little statistically significant evidence of EA support having an impact on clients’ well-being or health after 12 months (Tables 5.4 and 5.5). See Section 1.6 for a detailed description of the well-being and health measures.
However, using the ONS4 well-being questions, there is a pattern of non-significant results suggesting that those who saw an EA had lower levels of well-being at 12 months than the matched comparison group (Table 5.4). Within the combined ONS4 well-being scale, there is a nine percentage point negative difference in the proportions scoring as ‘very high’ (on a four-point scale from ‘very high to ‘low’) between those who had seen an EA (six per cent) and the matched comparison group (15 per cent). Likewise, those had seen an EA were less likely than the matched comparison group to score as having higher levels (seven or more on a scale from 0 to 10) of life satisfaction and happiness, and were more likely to report feeling anxious (six or more on a scale from 0 to 10). This pattern of findings may reflect a genuine negative impact despite non-significance, but as discussed in Section 5.2, the fact that the EA and matched comparison groups could not be matched on baseline well-being scores, there is a strong possibility that these findings partially reflect a pre-existing difference between the two groups that has not been controlled for.
However, this pattern is not replicated with the WHO-5 well-being scale, which shows very little difference between those who saw an EA and the matched comparison group.
Table 5.4 Impact of Employment Advisers on IAPT clients’ well-being among
those looking for work at baseline
| Level of well-being | Employment Adviser group | Matched comparison group | Percentage point/mean score difference | p-value |
|---|---|---|---|---|
| WHO-5 well-being Index | ||||
| Mean score (out of 5) | 3.67 (sd 1.17) | 3.64 (sd 1.31) | 0.0 | 0.906 |
| % | % | 0.854 | ||
| Unimpaired wellbeing | 43 | 42 | 1.2 | |
| Impaired well-being | 21 | 22 | -1.2 | |
| Likely depression | 35 | 35 | -0.9 | |
| ONS4 well-being measures | ||||
| Mean scores (out of 10) | ||||
| Overall well-being score | 5.71 (sd 2.11) | 6.05 (sd 2.59) | -0.3 | 0.416 |
| Life satisfaction | 6.64 (sd 2.41) | 6.88 (sd 2.75) | -0.2 | 0.579 |
| Feeling life is worthwhile 7.11 (sd 2.46) | 7.23 (sd 2.87) | -0.1 | 0.795 | |
| Happiness | 6.80 (sd 2.65) | 7.20 (sd 2.98) | -0.4 | 0.384 |
| Anxiety | 5.64 (sd 2.86) | 5.11 (sd 2.98) | 0.5 | 0.239 |
| % | % | |||
| Overall well-being score | .195 | |||
| Very high | 6 | 15 | -8.7 | |
| High | 26 | 30 | -4.0 | |
| Medium | 31 | 25 | 6.4 | |
| Low | 36 | 30 | 6.3 | |
| Higher score on life satisfaction | 43 | 51 | -7.9 | .317 |
| Higher score on life being worthwhile | 51 | 49 | 2.0 | .783 |
| Higher score on happiness | 44 | 54 | -9.2 | .223 |
| Higher score on anxiety | 42 | 34 | 8.1 | .270 |
| Base: all looking for work at baseline | 223 | 68 |
The picture is somewhat different in relation to clients’ use of GP services (Table 5.5). Those who had seen an EA are statistically significantly less likely to have reported visiting a GP within the previous two weeks (74 per cent have not done so compared to 59 per cent of those in the matched comparison group). There is no statistically significant evidence that seeing an EA has an impact on the reported visits to hospital outpatient departments or Casualty.
There is no evidence of EA support having an impact on overall health-related quality of life as measured by the EQ-5D-3L.
Table 5.5 Impact of Employment Advisers on IAPT clients’ health and use of health services among those looking for work at baseline
| Use of health service | Employment Adviser group | Matched comparison group | Percentage point/mean score difference | p-value |
|---|---|---|---|---|
| EQ-5D-3L Value Index | ||||
| Mean score | 0.69 (sd 0.25) | 0.66 (sd 0.27) | 0.03 | 0.480 |
| % | % | |||
| GP visits in past two weeks | .002* | |||
| Yes, more than once | 5 | 22 | -16.8 | |
| Yes, once | 21 | 19 | 1.6 | |
| No | 74 | 59 | 15.2 | |
| Contact with mental health services in past two weeks | .086 | |||
| Yes, more than once | 4 | 11 | -7.8 | |
| Yes, once | 5 | 4 | 1.7 | |
| No | 91 | 85 | 6.0 | |
| Been to Casualty in past three months | .491 | |||
| Yes, more than once or can’t remember how many times | 3 | 3 | -0.5 | |
| Yes, once | 6 | 12 | -5.5 | |
| No | 91 | 85 | 6.0 | |
| Been to Outpatients in past three months | .694 | |||
| Yes, more than once or can’t remember how many times | 12 | 16 | -4.3 | |
| Yes, once | 11 | 9 | 2.1 | |
| No | 77 | 75 | 2.1 | |
| Base: all looking for work at baseline | 223 | 68 |
5.5. Impact on those off work sick on IAPT entry
Employment outcomes[footnote 50]
Among those who were off sick when they began IAPT, there is no statistically significant evidence that EA support impacts on their propensity to be in employment (Table 5.6) or on their engagement with paid work (Table 5.7) 12 months later.
However, there is non-significant evidence to suggest that those who saw an EA as part of IAPT are less likely to be employed and working after 12 months. Seven in ten (72 per cent) of those who saw an EA were employed and working compared to eight in ten (81 per cent) of the matched comparison group.
A non-significant difference should not be over-interpreted, but, as discussed in Section 5.2, one possible explanation for the observed difference is that it may reflect a potential bias in the matched comparison group, with the EA group perhaps starting with more problems at work than the matched comparison group. As data on problems at work at the start of IAPT were not collected, this was not included in the matching. An alternative hypothesis is that the EA group may be slower to re-enter work because liaison with employers is ongoing.
Table 5.6 Impact of Employment Advisers on IAPT clients’ employment status and conditions among those off work sick at baseline
| Employment status | Employment Adviser group | Matched comparison group | Percentage point difference | p-value |
|---|---|---|---|---|
| % | % | |||
| Employed and working | 72 | 81 | -8.9 | .175 |
| Working status | .529 | |||
| Employed and working (including on leave other than health reasons) | 72 | 81 | -8.9 | |
| Employed but off sick | 7 | 4 | 3.5 | |
| Looking for work | 10 | 8 | 2.1 | |
| Retired or not in work and not intending to work in future | 11 | 8 | 3.4 | |
| Base: all off work sick at baseline | 227 | 70 |
Amongst the sub-set of those who had re-entered work after 12 months, there is nonsignificant evidence that those who had seen an EA are less likely to be affected by physical or psychological health problems in work than those who did not see an EA (Table 5.7). Using the Productivity Cost Questionnaire (PCQ) to measure ‘presenteeism’, taking account of the number of days where and the amount to which their work was affected by physical or psychological health problems (see Section 1.6 for more detail on its derivation), 68 per cent of those who had seen an EA and have re-entered work have a presenteeism score of less than a day, compared to 60 per cent of those re-entering work in the matched comparison group.
There is little evidence of EA support having an impact on IAPT clients’ attachment to their paid work, across the following outcomes:
- Level of enjoyment of the job (a four-point scale from ‘all of the time’ (4) to ‘none of the time’ (1) with higher levels of enjoyment measured as scoring 3 or 4);
- Level of motivation to stay in or return to their work (a five-point scale from ‘very’ (5) to ‘not at all’ (1) with higher levels of motivation measured as scoring 4 or 5);
- Level of confidence that they will stay in or return to their work (again, a five-point scale from ‘very’ (5) to ‘not at all’ (1) with higher levels of confidence measured as scoring 4 or 5);
- Plans to change jobs or their working hours (‘yes’, ‘no’, or ‘don’t’ know’).
More details on these measures can be found in Section 1.6.
Table 5.7 Impact of Employment Advisers on IAPT clients’ presenteeism and
attachment to work among those off work sick at baseline
| Presenteeism and those off sick | Employment Adviser group | Matched comparison group | Percentage point/mean score difference | p-value |
|---|---|---|---|---|
| Presenteeism | ||||
| Mean score | 1.17 (sd 1.98) | 1.63 (sd 2.91) | -0.45 | 0.330 |
| % | % | |||
| Less than a day | 68 | 60 | 7.5 | .363 |
| A day or more | 32 | 40 | -7.5 | |
| Base: all employed but off work sick at baseline who employed and working at follow up | 158 | 55 | ||
| Job enjoyment | .519 | |||
| Enjoy job all or most of the time | 66 | 71 | -4.8 | |
| Enjoy job some or none of the time | 34 | 29 | 4.8 | |
| Motivation to stay in or return to work | .790 | |||
| Higher level of motivation | 79 | 81 | -1.9 | |
| Lower level of motivation | 21 | 19 | 1.9 | |
| Confidence about staying in or returning to work | .962 | |||
| Higher level of confidence | 78 | 77 | 0.5 | |
| Lower level of confidence | 22 | 23 | -0.5 | |
| Whether want to change jobs or hours | .701 | |||
| Yes | 17 | 14 | 2.3 | |
| No | 83 | 86 | -2.3 | |
| Base: all employed but off work sick at baseline who are in employed (including off sick) at follow up | 180 | 60 |
Well-being and health outcomes
Among those who were off sick on IAPT entry, there is very little statistically significant evidence of EA support having an impact on clients’ well-being or health (Tables 5.8 and 5.9) (see Section 1.6 for a description of these measures).
However, across the ONS4 life satisfaction measures, the general pattern of – albeit largely non-significant – results are that those who saw an EA have lower levels of well-being than the matched comparison group (Table 6.8). Within the combined ONS4 well-being scale, there is a ten percentage point negative difference in the proportions scoring as ‘very high’ (on a four-point scale from ‘very high to ‘low’) between those who had seen an EA (14 per cent) and the matched comparison group (24 per cent). Likewise, those who had seen an EA are less likely than the matched comparison group to score as having higher levels (seven or more on a scale from 0 to 10) of feeling worthwhile. However, those who had seen an EA are statistically significantly less likely to report feeling anxious (defined as a score of six or more on a scale from 0 to 10). Three in ten (29 per cent) score as having a higher level of anxiety compared to 43 per cent of the matched comparison group (a 14 percentage point difference). This pattern of results may reflect the lower re-entry to work rates for the EA group, but as with the group looking for work it is not possible to rule out bias in the matched comparison group without the ability to match the EA and comparison groups on baseline measures of well-being.
The pattern is not replicated with the WHO-5 scale, which shows very little difference between those who saw an EA and the matched comparison group.
Table 5.8 Impact of Employment Advisers on IAPT clients’ well-being among
those off work sick at baseline
| Status of well-being | Employment Adviser group | Matched comparison group | Percentage point/mean score difference | p-value |
|---|---|---|---|---|
| WHO-5 | ||||
| Mean score (out of 5) | 3.37 (sd 1.22) | 3.41 (sd 1.24) | 0.0 | 0.827 |
| % | % | |||
| Unimpaired wellbeing | 57 | 53 | 3.9 | 0.873 |
| Impaired well-being | 16 | 18 | 1.6 | |
| Likely depression | 26 | 29 | 2.3 | |
| ONS4 well-being measures | ||||
| Mean scores (out of 10) | ||||
| Overall well-being score | 6.57 (sd 2.16) | 6.58 (sd 2.54) | 0.0 | 0.991 |
| Life satisfaction | 7.48 (sd 2.37) | 7.71 (sd 2.54) | -0.2 | 0.562 |
| Feeling life is worthwhile | 7.93 (sd 2.36) | 8.41 (sd 2.28) | -0.5 | 0.171 |
| Happiness | 7.68 (sd 2.67) | 7.42 (sd 3.10) | 0.3 | 0.585 |
| Anxiety | 4.80 (sd 2.89) | 5.22 (sd 3.51) | -0.4 | 0.443 |
| % | % | |||
| Overall well-being score | ||||
| Very high | 14 | 24 | -10.2 | .381 |
| High | 33 | 27 | 6.9 | |
| Medium | 30 | 29 | 1.6 | |
| Low | 22 | 20 | 1.8 | |
| Higher score on life satisfaction | 59 | 62 | -2.2 | .774 |
| Higher score on life being worthwhile | 63 | 75 | -11.8 | .102 |
| Higher score on happiness | 60 | 64 | -4.5 | .556 |
| Higher score on anxiety | 29 | 43 | -14.4 | .049* |
| Base: all off work sick at baseline | 227 | 70 |
Among those off sick on IAPT entry, there is no statistically significant evidence of EA support having an impact on clients’ overall health-related quality of life, as measured by the EQ-5D-3L (see Section 1.6). Likewise, there is no statistically significant evidence of impact - and little percentage point difference - between IAPT clients’ use of GP, mental health services, casualty or outpatients (Table 5.9).
Table 5.9 Impact of Employment Advisers on IAPT clients’ health and use of health services among those off work sick at baseline
| Use of health service | Employment Adviser group | Matched comparison group | Percentage point/mean score difference | p-value |
|---|---|---|---|---|
| EQ-5D-3L Value Index | ||||
| Mean score 0.75 (sd 0.24) | 0.76 (sd 0.26) | 0.0 | 0.814 | |
| % | % | |||
| GP visits in past two weeks | ||||
| Yes, more than once | 8 | 6 | 2.1 | .775 |
| Yes, once | 19 | 23 | -3.9 | |
| No | 73 | 71 | 1.8 | |
| Contact with mental health services in past two weeks | ||||
| Yes, more than once | 3 | 5 | -2.7 | .276 |
| Yes, once | 4 | 1 | 2.6 | |
| No | 93 | 93 | 0.1 | |
| Been to Casualty in past three months | ||||
| Yes, more than once or can’t remember how many times | 1 | 1 | 0.0 | .631 |
| Yes, once | 4 | 2 | 2.2 | |
| No | 95 | 97 | -2.1 | |
| Been to Outpatients in past three months | ||||
| Yes, more than once or can’t remember how many times | 8 | 6 | 1.7 | .796 |
| Yes, once | 8 | 10 | -1.9 | |
| No | 84 | 84 | 0.3 | |
| Base: all off work sick at baseline | 227 | 70 |
6. Conclusions and recommendations
This chapter reflects on the findings of the report to determine key conclusions from the client research. It also considers the limitations of the current research in making recommendation for further evaluation work.
Conclusions
A challenge of this evaluation was securing access to patient contact details and profiles for primary research. The arrangements made with Improving Access to Psychological Therapies (IAPT) services meant that patients had to give explicit consent to be approached for the research and the consent questions were administered by IAPT staff. It has not been possible to compare volumes and profiles of individuals providing consent with the population of IAPT patients to establish representativeness. However, the variation in volumes of contact details provided (with some services returning none at all) raises concerns about the consistency with which the process was applied. Furthermore, overall volumes of sample received were low, particularly for the matched comparison groups, limiting the conclusions that can be drawn. These caveats means that the survey findings need to be treated with some caution.
That said, the conclusions that can be drawn from the EA clients surveyed and interviewed are that:
- Those engaging with an Employment Adviser were more likely to be in employment than looking for work and hence – to a large extent – EA support was related to making an existing job better suited to the client’s needs. There was a reasonably even split between those working, those employed but off sick and those looking for work.
- Generally, it appeared that EAs empowered clients to address their employment situation themselves rather than intervening directly. In a minority of cases, EAs contacted employers, trade unions and other organisations on behalf of clients but the proportions of clients achieving change extended well beyond this group.
- A close link between employment and mental health was evident among most patients seeking EA support. Regardless of employment situation, patients who accessed an EA commonly described how the situations they were seeking support with were both exacerbating and exacerbated by poor mental health.
- From a client perspective, EA support seems to have been delivered well. Although qualitative research indicated that clients often attended EA support with very low expectations, the survey found that for most the experience was very positive. Most found the support useful (and half ‘very useful’), while threequarters felt that their adviser had a good understanding of their needs and almost three-in-five strongly agreed that the support was tailored to their needs.
- Across all client groups, qualitative research indicated that what really seemed to work in delivering EA support was the combination of practical, emotional and motivational support. Patients felt that their EAs were effective in building an empathetic relationship which then meant that they were able to challenge pre-conceptions (e.g. around the employment options open to the client; around their ability to change their current relationship with their employer) in a constructive manner. Others talked about practical support around developing CVs and practicing interview techniques.
- A key intended outcome of the EAs in IAPT programme was to achieve an integrated service and it would appear that this was generally achieved. Qualitative research indicated that a highly integrated service was experienced by some where it was clear to the client that their therapist and EA had exchanged notes and formulated joint action plans. In other cases, liaison between therapists and EAs was less obvious and clients experienced the two elements of the support as being distinct from one another, however, clients still found that the two parts of the service fit together and reinforced each other.
Initial impacts on those looking for work
Preliminary impact estimates provided evidence of EA support having a positive impact on entry to work for clients who were looking for work on entry to IAPT. Around twelve months after entry to IAPT, these clients were significantly more likely to be in employment (compared to IAPT clients in Wave Two areas who had not seen an EA). Clients looking for work were also significantly less likely to have seen their GP within the previous two weeks than the comparison group.
There was indicative (but non-significant) evidence of EA support having a positive impact on job search activity for those still looking for work at 12 months. For those still seeking work after 12 months, there was non-significant evidence of those who had EA support doing more job search activity and having a stronger desire to find work. However, there was also some indicative (but nonsignificant) evidence of EA support being linked to lower levels of confidence in finding work among those still looking for work.
Impacts on those employed off sick
Impact estimates did not find a positive impact on the likelihood to have returned to work among those who were off work sick. In fact, there was nonsignificant evidence that those who saw an EA were less likely to be back at work than the matched comparison group after 12 months. The lack of significant impact on the employment situation of those who were off work sick would seem to suggest that the additional support of an EA does not add greatly to that of IAPT therapists in terms of securing a return to work. This may be because of the role that employers play in controlling the end to a period off sick.
It is possible that, although the numbers returning to work are not significantly better among those who saw an EA, those who saw an EA had a better experience of returning to work than would otherwise have been the case. From the impact analysis, there was significant evidence that those who had seen an EA had lower levels of anxiety than the matched comparison group after 12 months. There was also non-significant evidence of reduced presenteeism. Longitudinal analysis comparing experiences at 5 and 12 months would also seem to support a reduction in presenteeism (and therefore increases in productivity).
Impacts on those in-work
It was not possible to make impact estimates for those who were employed and in-work on entry to IAPT because of difficulties in identifying a suitable matched comparison group without data on work-related problems on service entry. The final impact estimates will attempt to make estimates for this subgroup by using a richer range of data to identify a suitable comparison group.
Longitudinal analysis points to many of this group securing positive employment-related outcomes and this client group was the most likely to agree that their EA helped them with their employment goal (i.e. to stay in work). For example, many of this group report having secured adjustments to their workplace environment or to the terms of and conditions of their job role (and the majority of those securing these changes attribute them – at least in part – to the input of their EA). In addition, there are marked reductions in presenteeism among this group (and therefore increases in productivity). However, without the ability to compare results to an appropriate comparison group it is not possible to say whether these are changes that would have occurred independently of IAPT support altogether or as a function just of the therapist input.
Impacts on well-being
There is also some evidence of EA support being linked to lower levels of well-being at the 12-month point among both those looking for work and those off work sick when they began IAPT. However, given the absence of baseline data on these measures, it is not possible to rule out the conclusion that IAPT clients taking up EA support entered with lower levels of well-being and confidence. These results should be possible to explore further with access to the IAPT data which will provide detail of the level of anxiety and depression on entry to IAPT for all IAPT clients.
Further planned evaluation activity
The final strand of this evaluation will conduct impact analysis of IAPT patient data. This will make it possible to robustly estimate the impact of receiving combined employment support and therapy for some outcomes, such as levels of anxiety and depression and out of work benefit receipt relative to a matched control group who only received IAPT treatment. It will provide aggregate data for all IAPT clients, for one large EA in IAPT provider, and provide baseline measures as well as data at the point of leaving the IAPT service.
Appendix A: Consent process
The following sections were presented to the relevant participating Clinical Commissioning Groups (CCGs) at the evaluation onset, to inform them of the required consent process for clients.
Non-case study CCG areas – quantitative survey research only
There are three main steps of recruitment in non-case study CCG areas.
Step 1: Clients will be introduced to the evaluation either by their Employment Adviser (EA) in their first EA appointment (for those who take up EA support in each wave), or by their therapist in their fourth therapy session (for those who do not take up EA support). The EA or therapist will explain the purpose of the evaluation, with the aid of a Client Information Sheet. The Client Information sheet used in non-case study areas will describe the quantitative survey strand. The EA or therapist will establish whether the client consents to have their details securely transferred to IFF (CI) and record this on the IAPT system.
The process for transferring client details for survey will differ between Wave One and Wave Two areas. In Wave One areas, between October 2018 and March 2019, client details will be transferred to IFF (CI) on a monthly basis by the data controller at the IAPT provider. In Wave Two, there will be two data transfers of client details:
For clients starting treatment between 1st July and 30th September 2018, the data transfer date will be January 2018;
For clients starting treatment between 1st October and 31st January 2018, the data transfer date will be March 2019.
Step 2: An “information and opt-out letter” will be sent to each client that consented for their details to be securely transferred to IFF. The letter will provide details of how to opt out of the evaluation and explain that, if they do not opt out, then an interviewer from IFF will call the client to ask if they would like to participate in the quantitative survey.
Step 3: An IFF interviewer will call all clients that did not opt out after receiving the letter.
The interviewer will ask if the client would like to participate in a survey interview and if the client agrees, the interviewer will arrange a convenient time to conduct the interview.
Case study areas: qualitative and quantitative evaluation
Step 1: Step 1 is identical to that described above for the non-case study areas. The Client Information Sheet describes both the quantitative and the qualitative strands and explains that consenting clients will be randomly allocated to one strand or the other.
The process for recording client consent and transferring client details to IFF (CI) is as described above.
Step 2: Once details of consenting clients have been received by IFF, they will be randomly allocated to either the qualitative or the quantitative strand of the research (sample size requirements are discussed elsewhere in this document).
Step 3: Those clients in the quantitative sample will receive the ‘information and opt out’ letter from IFF as described above. Those clients in the qualitative sample will be sent an ‘information and opt-out’ letter about the qualitative research. The opt out process for both strands will be managed by IFF (CI).
Step 4: An IFF or ICF researcher (depending on the case study CCG area) will call those clients that did not opt out after receiving the letter. The researcher will ask if the client is happy to take part in a qualitative interview.
Appendix B: Sample outcomes
The following tables present the full breakdown of sample outcomes across the Time 1 and Time 2 surveys. For Time 2 surveys, the breakdown is shown at overall level (B.2), and broken down by Wave 1 (B.3) and Wave 2 (B.4) outcomes.
Table B.1 Final sample outcomes for the Wave 1 Time 1 survey
| Sample | Total count | % sample received | % starting sample |
|---|---|---|---|
| Useable sample received | 3,268 | 100 | - |
| Opt outs | 218 | 7 | - |
| Starting sample | 3,050 | 93 | 100 |
| Completed interviews | 1,609 | 49 | 53 |
| Still ‘live’ at the end of fieldwork[footnote 51] | 66 | 1 | 2 |
| Refusals | 423 | 13 | 14 |
| Exhausted / unusable[footnote 52] | 952 | 29 | 31 |
Table B.2 Final sample outcomes for the Time 2 survey (all)
| Sample | Total count | % sample received | % starting sample |
|---|---|---|---|
| Useable sample received | 2,099 | 100 | - |
| Opt outs | 51 | 3 | - |
| Starting sample | 2,048 | 97 | 100 |
| Completed interviews | 1,364 | 65 | 67 |
| Still ‘live’ at the end of fieldwork | 348 | 17 | 17 |
| Refusals | 193 | 9 | 9 |
| Support not recalled | 4 | <1 | <1 |
| Did not see an EA (W1 only) | 35 | 2 | 2 |
| Exhausted / unusable | 104 | 5 | 5 |
Table B.3 Final sample outcomes for the Time 2 survey (Wave 1 only)
| Sample | Total count | % sample received | % starting sample |
|---|---|---|---|
| Useable sample received | 1,087 | 100 | - |
| Opt outs | 7 | <1 | - |
| Starting sample | 1,080 | 99 | 100 |
| Completed interviews | 755 | 69 | 70 |
| Still ‘live’ at the end of fieldwork | 170 | 16 | 16 |
| Refusals | 84 | 8 | 7 |
| Support not recalled | 1 | <1 | <1 |
| Did not see an EA | 35 | 3 | 3 |
| Exhausted / unusable | 42 | 4 | 4 |
Table B.4 Final sample outcomes for the Time 2 survey (Wave 2 only)
| Sample | Total count | % sample received | % starting sample |
|---|---|---|---|
| Useable sample received | 1,012 | 100 | - |
| Opt outs | 44 | 4 | - |
| Starting sample | 968 | 96 | 100 |
| Completed interviews | 609 | 60 | 63 |
| Still ‘live’ at the end of fieldwork | 178 | 18 | 18 |
| Refusals | 116 | 16 | 12 |
| Support not recalled | 3 | <1 | <1 |
| Exhausted / unusable | 62 | 6 | 6 |
Appendix C: Impact tables where counterfactual is ‘nonintervention’ in Wave Two areas
The following tables present the impact estimates of Employment Adviser (EA) support within Improving Access to Psychological Therapies (IAPT) comparing the outcomes of those taking up EA support in Wave One areas to all IAPT clients interviewed in the Wave Two comparison areas, including 20 per cent who took up EA support. The broad pattern of results follows those in Chapter 5 which measure the impact of EA support against a counterfactual of no EA support. However, as expected, the differences between the two groups are smaller and the impact among those looking for work on being in paid employment after 12 months is no longer statistically significant.
Impact on those looking for work when they started IAPT
Table C.1: Impact of Employment Advisers on IAPT clients’ employment status and conditions among those looking for work at baseline
| Employment status | Employment Adviser group | Matched comparison group | Percentage point difference | p-value |
|---|---|---|---|---|
| % | % | |||
| Employed and working | 48 | 36 | 11.7 | .094 |
| Working status | .257 | |||
| Employed and off work for reasons other than health | 48 | 36 | 11.7 | |
| Employed but off sick | 2 | 1 | 0.9 | |
| Looking for work | 42 | 55 | -13.0 | |
| Retired or not in work and not intending to work in future | 9 | 8 | 0.4 | |
| Base: all looking for work at baseline | 223 | 102 |
Table C.2: Impact of Employment Advisers on IAPT clients’ job search activity among those looking for work at baseline
| Job search activity | Employment Adviser group | Matched comparison group | Percentage point difference | p-value |
|---|---|---|---|---|
| % | % | |||
| Job search activity scale | .749 | |||
| Higher levels of job search | 48 | 46 | 2.6 | |
| No or lower levels of job search (or missing data) | 52 | 54 | -2.6 | |
| Number of vacancies applied for | .753 | |||
| Five or more | 18 | 24 | -5.5 | |
| Fewer than five | 24 | 22 | 1.5 | |
| None | 58 | 54 | 4.0 | |
| Number of CVs submitted | .074 | |||
| Five or more | 9 | 8 | 0.3 | |
| Fewer than five | 31 | 15 | 16.3 | |
| None | 60 | 77 | -16.6 | |
| Job search hours | .054 | |||
| Less than an hour | 39 | 52 | -12.9 | |
| One to two hours | 32 | 37 | -4.6 | |
| Three hours or more | 29 | 11 | 17.6 | |
| Base: all looking for work at baseline and follow up | 93 | 63 |
Table C.3: Impact of Employment Advisers on IAPT clients’ job search self-efficacy and thoughts on entering work among those looking for work at
baseline
| Thoughts on entering work | Employment Adviser group | Matched comparison group | Percentage point difference | p-value |
|---|---|---|---|---|
| % | % | |||
| Whether feels able to return to work | .843 | |||
| Health condition rules it out | 15 | 16 | -1.3 | |
| Could consider going into work or reports currently being in work[footnote 53] | 85 | 84 | 1.3 | |
| Whether and when wants to return to work | .570 | |||
| Yes, to a great or some extent, within six months | 61 | 50 | 10.9 | |
| Yes, to a great or some extent, within 12 months | 18 | 20 | -2.0 | |
| Yes, to a great or some extent, not within 12 months | 15 | 20 | -4.5 | |
| Does not want to return to work or only a little | 5 | 10 | -4.4 | |
| Motivation to find work | .168 | |||
| Higher level of motivation | 45 | 57 | -12.2 | |
| Lower level of motivation | 55 | 43 | 12.2 | |
| Confidence about finding work | .031* | |||
| Higher level of confidence | 18 | 34 | -16.1 | |
| Lower level of confidence | 82 | 66 | 16.1 | |
| % agreeing or agreeing strongly that | ||||
| “I am worried that working could make my health condition worse” | 41 | 51 | -10.0 | .248 |
| “The idea of working makes me feel anxious” | 48 | 48 | 0.0 | .967 |
| “I think employers could accommodate my health needs” | 44 | 30 | 13.8 | .094 |
| “I don’t know what suitable jobs are available” | 39 | 25 | 14.1 | .071 |
| “I don’t feel confident about applying for jobs” | 38 | 27 | 10.6 | .181 |
| Base: all looking for work at baseline and follow up | 93 | 63 |
Table C.4: Impact of Employment Advisers on IAPT clients’ well-being among those looking for work at baseline
| Well-being status | Employment Adviser group | Matched comparison group | Percentage point/mean score difference | p-value |
|---|---|---|---|---|
| WHO-5 well-being index | ||||
| Mean score (out of 5) | 3.67 (sd 1.17) | 3.59 (sd 1.27) | 0.1 | .629 |
| % | % | |||
| Unimpaired well-being | 43 | 44 | -0.7 | .692 |
| Impaired well-being | 21 | 23 | -2.1 | |
| Likely depression | 35 | 33 | 1.9 | |
| ONS-4 well-being measures | ||||
| Mean scores (out of 10) | ||||
| Overall well-being score | 5.71 (sd 2.11) | 6.16 (sd 2.32) | -0.4 | .141 |
| Life satisfaction | 6.64 (sd 2.41) | 7.19 (sd 2.42) | -0.6 | .079 |
| Feeling life is worthwhile | 7.11 (sd 2.46) | 7.39 (sd 2.66) | -0.3 | .403 |
| Happiness | 6.80 (sd 2.65) | 7.28 (sd 2.77) | -0.5 | .178 |
| Anxiety | 5.64 (sd 2.86) | 5.21 (sd 2.96) | 0.4 | .276 |
| % | % | |||
| Overall well-being score | .248 | |||
| Very high | 6 | 13 | -6.3 | |
| High | 26 | 31 | -4.9 | |
| Medium | 31 | 27 | 3.6 | |
| Low | 36 | 29 | 7.6 | |
| Higher score on life satisfaction | 43 | 55 | -12.3 | .063 |
| Higher score on life being worthwhile | 51 | 50 | 0.7 | .928 |
| Higher score on happiness | 44 | 52 | -7.8 | .239 |
| Higher score on anxiety | 42 | 34 | 7.3 | .242 |
| Base: all looking for work at baseline | 223 | 102 |
Table C.5: Impact of Employment Advisers on IAPT clients’ health and use of health services among those looking for work at baseline
| Use of health service | Employment Adviser group | Matched comparison group | Percentage point/mean score difference | p-value |
|---|---|---|---|---|
| EQ5D-3L Value Index | ||||
| Mean score | 0.69 (sd 0.25) | 0.71 (sd 0.24) | 0.0 | .460 |
| % | % | |||
| GP visits in past two weeks | .045* | |||
| Yes, more than once | 5 | 14 | -8.9 | |
| Yes, once | 21 | 17 | 4.1 | |
| No | 74 | 70 | 4.8 | |
| Contact with mental health services in past two weeks | .318 | |||
| Yes, more than once | 4 | 8 | -4.4 | |
| Yes, once | 5 | 6 | -0.9 | |
| No | 91 | 86 | 5.3 | |
| Been to Casualty in past three months | .849 | |||
| Yes, more than once or can’t remember how many times | 3 | 4 | -0.9 | |
| Yes, once | 6 | 8 | -1.8 | |
| No | 91 | 88 | 2.6 | |
| Been to Outpatients in past three months | .120 | |||
| Yes, more than once or can’t remember how many times | 12 | 13 | -1.3 | |
| Yes, once | 11 | 4 | 6.7 | |
| No | 77 | 83 | -5.4 | |
| Base: all looking for work at baseline | 223 | 102 |
Impact on those off work sick when they started IAPT
Table C.6: Impact of Employment Advisers on IAPT clients’ employment status and conditions among those off work sick at baseline
| Employment status | Employment Adviser group | Matched comparison group | Percentage point difference | p-value |
| % | % | |||
| Employed and working | 72 | 81 | -9.1 | .103 |
| Working status | .394 | |||
| Employed and off work for reasons other than health | 72 | 81 | -9.1 | |
| Employed but off sick | 7 | 5 | 1.8 | |
| Looking for work | 10 | 7 | 2.3 | |
| Retired or not in work and not intending to work in future | 11 | 6 | 4.9 | |
| Base: all off work sick at baseline | 227 | 112 |
Table C.7: Impact of Employment Advisers on IAPT clients’ presenteeism and attachment to work among those off work sick at baseline
| Presenteeism and those off sick | Employment Adviser group | Matched comparison group | Percentage point/mean score difference | p-value |
|---|---|---|---|---|
| Presenteeism | ||||
| Mean score | 1.17 (sd 1.98) | 1.37 (sd 2.40) | -0.2 | .527 |
| % | % | |||
| Less than a day | 68 | 62 | 6.1 | .396 |
| A day or more | 32 | 38 | -6.1 | |
| Base: all employed but off work sick at baseline who are employed and working at follow up | 158 | 88 | ||
| Job enjoyment | .841 | |||
| Enjoy job all or most of the time | 66 | 68 | -1.4 | |
| Enjoy job some or none of the time | 34 | 33 | 1.4 | |
| Motivation to stay in or return to work | .126 | |||
| Higher level of motivation | 79 | 70 | 9.4 | |
| Lower level of motivation | 21 | 30 | -9.4 | |
| Confidence about staying in or returning to work | .807 | |||
| Higher level of confidence | 78 | 76 | 1.4 | |
| Lower level of confidence | 22 | 24 | -1.4 | |
| Whether want to change jobs or hours | .826 | |||
| Yes | 17 | 18 | -0.9 | |
| No | 83 | 82 | -0.9 | |
| Base: all employed off work sick at baseline who are employed (including off sick at follow up) | 180 | 97 |
Table C.8: Impact of Employment Advisers on IAPT clients’ well-being among those off work sick at baseline
| Well-being status | Employment Adviser group | Matched comparison group | Percentage point/mean score difference | p-value |
|---|---|---|---|---|
| WHO-5 well-being index | ||||
| Mean score (out of 5) | 3.37 (sd 1.22) | 3.27 (sd 1.18) | 0.1 | .520 |
| % | % | |||
| Unimpaired well-being | 57 | 61 | -4.2 | .730 |
| Impaired well-being | 16 | 16 | -0.2 | |
| Likely depression | 26 | 22 | 4.4 | |
| ONS-4 well-being measures | ||||
| Mean scores (out of 10) | ||||
| Overall well-being score 6.57 (sd 2.16) | 6.83 (sd 2.27) | -0.3 | .366 | |
| Life satisfaction | 7.48 (sd 2.37) | 7.92 (sd 2.19) | -0.4 | .115 |
| Feeling life is worthwhile | 7.93 (sd 2.36) | 8.31 (sd 2.16) | -0.4 | .167 |
| Happiness | 7.68 (sd 2.67) | 7.81 (sd 2.78) | -0.1 | .705 |
| Anxiety | 4.80 (sd 2.89) | 4.71 (sd 3.37) | 0.1 | .822 |
| % | % | |||
| Overall well-being score | .270 | |||
| Very high | 14 | 23 | -8.6 | |
| High | 33 | 34 | -0.1 | |
| Medium | 30 | 28 | 2.4 | |
| Low | 22 | 16 | 6.3 | |
| Higher score on life satisfaction | 59 | 69 | -9.4 | .129 |
| Higher score on life being worthwhile | 63 | 75 | -12.2 | .032* |
| Higher score on happiness | 60 | 67 | -6.8 | .277 |
| Higher score on anxiety | 29 | 38 | -9.2 | .116 |
| Base: all off work sick at baseline | 227 | 112 |
Table C.9: Impact of Employment Advisers on IAPT clients’ health and use of health services among those off work sick at baseline
| Use of health services | Employment Adviser group | Matched comparison group | Percentage point/mean score difference | p-value |
|---|---|---|---|---|
| EQ5D-3L Value Index | ||||
| Mean score | 0.75 (sd 0.24) | 0.80 (sd 0.22) | 0.0 | .100 |
| % | % | |||
| GP visits in past two weeks | .980 | |||
| Yes, more than once | 8 | 8 | -0.3 | |
| Yes, once | 19 | 18 | 0.8 | |
| No | 73 | 74 | -0.5 | |
| Contact with mental health services in past two weeks | .200 | |||
| Yes, more than once | 3 | 3 | -0.4 | |
| Yes, once | 4 | 2 | 3.1 | |
| No | 93 | 96 | -2.7 | |
| Been to Casualty in past three months | .091 | |||
| Yes, more than once or can’t remember how many times | 1 | 6 | -4.7 | |
| Yes, once | 4 | 3 | 1.4 | |
| No | 95 | 91 | 3.4 | |
| Been to Outpatients in past three months | .752 | |||
| Yes, more than once or can’t remember how many times | 8 | 10 | -2.5 | |
| Yes, once | 8 | 7 | 1.0 | |
| No | 84 | 83 | 1.5 | |
| Base: all off work sick at baseline | 227 | 112 |
Appendix D: Generating the matched comparison samples for those looking for work and those off work sick
Chapter 5 of the report compares outcomes for those looking for work and those off work sick in Wave One areas who have seen an Employment Adviser (EA) within Improving Access to Psychological Therapies (IAPT) with those of a matched comparison group. The matched comparison group is essentially a weighted version of the Wave Two survey sample for the relevant group, excluding those who have seen an EA, with the purpose being to generate a weighted sample that, at baseline, has a very similar profile to the EA group. The matched comparison group is then assumed to give an estimate of the counterfactual for those seeing an EA – that is, what their profile of outcomes would have been without the EA support - with any significant differences being evidence of impact.
The matched comparison groups for those looking for work and those off work sick were both generated using propensity score matching (psm), the main steps of which are:
- The probability (or propensity) of an individual being in the EA group (rather than the Wave Two group) is estimated from a logistic regression model of the data. The binary outcome variable in the model is the group (1=EA; 0=comparison), and the predictors are all the available baseline characteristics.
- The Wave Two comparison group is then weighted so that the distribution of propensity scores in the Wave Two sample is the same as in the EA group.
The technical details of the matching undertaken are as follows:
- The logistic regression model was fitted within SPSS with forward stepwise selection of variables.
- The weights for the control group were calculated as inverse propensity weights (i.e. p/1-p). Comparison group members that are very similar to participants, and hence have a high propensity score are given a large weight; comparison group members that are dissimilar to participants, and hence have a low propensity score are given a small weight.
The matching variables included in the survey propensity score models differed somewhat for the looking for work and off work sick groups.
Matched comparison group for those looking for work
For the looking for work group the matching variables were:
- Demographic characteristics: age; gender; whether has a partner; whether has children; qualifications
- Employment history and finance: length of time unemployed before the start of IAPT; summary of work history prior to the start of IAPT; whether has a mortgage or other debt;
- Health: whether has any mental or physical health conditions or illnesses that have lasted 12 months or more: whether had anxiety or panic attacks at the start of IAPT; whether had depression at the start of IAPT; whether had stress at the start of IAPT; whether had any other mental health condition at the start of IAPT.
A reasonable test of whether the propensity score matching has generated a good matched comparison group is to compare the profiles of the two groups: participant and matched comparison. The matching is judged to have been successful is there are no statistically significant differences between the two groups on any of the matching variables – which is the case. Table D.1 shows the profile of the two groups.
Table D.1: Baseline differences between the EA looking for work and matched comparison groups
| Comparison group | EA looking for work group | Matched comparison group | p-value |
|---|---|---|---|
| % | % | ||
| Gender | 0.936 | ||
| Male | 45 | 45 | |
| Female | 55 | 55 | |
| Age | 0.555 | ||
| 16-24 | 24 | 24 | |
| 25-34 | 21 | 27 | |
| 35-49 | 29 | 25 | |
| 50-59 | 22 | 15 | |
| 60-65 | 5 | 9 | |
| Whether has a partner | 0.190 | ||
| Yes | 19 | 38 | |
| No | 80 | 55 | |
| Not answered | 1 | 0 | |
| Whether has children | 0.992 | ||
| Yes | 23 | 22 | |
| No | 77 | 78 | |
| Qualifications | 0.261 | ||
| Level 5 or over | 40 | 28 | |
| Levels 3 or 4 | 23 | 30 | |
| None or up to level 2 | 37 | 42 | |
| Length of time unemployed before start of IAPT | 0.101 | ||
| Less than 12 months | 51 | 35 | |
| More than 12 months or never worked | 33 | 41 | |
| Not answered | 16 | 24 | |
| Summary of work history | 0.894 | ||
| Never been in paid work | 6 | 5 | |
| Spent most of my time out of paid work | 15 | 18 | |
| Spent about as much time in paid work as not | 20 | 17 | |
| Spent most of my time working | 59 | 60 | |
| Whether has a mortgage or debt | 0.495 | ||
| Yes | 44 | 41 | |
| No | 55 | 59 | |
| Not answered | 1 | 0 | |
| Longstanding health condition | 0.729 | ||
| Yes | 72 | 75 | |
| No | 28 | 25 | |
| Whether had anxiety at start of IAPT | 0.926 | ||
| Yes | 86 | 87 | |
| No | 14 | 13 | |
| Whether had depression at start of IAPT | 0.884 | ||
| Yes | 89 | 90 | |
| No | 11 | 10 | |
| Whether had stress at start of IAPT | 0.527 | ||
| Yes | 87 | 90 | |
| No | 13 | 10 | |
| Whether had other mental health condition at start of IAPT | 0.313 | ||
| Yes | 18 | 25 | |
| No | 82 | 75 | |
| Bases: | 223 | 68 |
Although, none of the baseline characteristics are statistically significantly different between the EA looking for work group and the matched comparison group, there are still a few large differences that could, in principle, bias the estimates of impact. In particular, the percentage unemployed for less than 12 months is 51 per cent in the EA looking for work group but just 35 per cent in the matched comparison group.
Similarly, the percentage in the EA looking for work group with qualifications of Level 5 or above is 40 per cent, but just 28 per cent in the matched comparison group. The small sample size in the matched comparison group means that these do not reach significance. To test whether these differences are affecting the impact estimates presented in Chapter 5, a series of logistic regression models have been run for a range of the outcomes presented recalculated as binaries. For each of these regressions, the effect of the EA is estimated using the matching comparison group (that is, applying the propensity score weights) but also controlling for age, gender, length of time unemployed and qualification level. These tests suggest that the estimates of impact are not, in fact, markedly affected by the relatively poor match on length of unemployment and qualifications. Table D.2 shows the standard PSM estimates of impact against the regression adjusted estimates for three binary outcomes: employed and working; with likely depression (as measured by the WHO-5); and seen a GP in the past two weeks.
Table D.2: Impact of Employment Advisers among those looking for work as
measured by psm and by psm with regression adjustments
| Employed and well-being | Impact measured using just psm (percentage point difference) | Impact measured using psm plus regression adjustment (percentage point difference) |
|---|---|---|
| Employed and working | 19 | 19 |
| Likely depression (WHO-5) | -1 | 2 |
| Seen a GP in last two weeks | -15 | -15 |
Off work sick group matched comparison group
For the off work sick group, the matching variables were:
- Demographic characteristics: age; gender; whether has a partner; whether has children; qualifications
- Employment history and finance: length of time off sick before the start of IAPT; whether in full time or part time employment at the start of IAPT; presenteeism at the start of IAPT; summary of work history prior to the start of IAPT; whether has a mortgage or other debt;
- Health: whether has any mental or physical health conditions or illnesses that have lasted 12 months or more: whether had anxiety or panic attacks at the start of IAPT; whether had depression at the start of IAPT; whether had stress at the start of IAPT; whether had any other mental health condition at the start of IAPT.
Table D.3 shows the profile for the off work sick and matched comparison groups.
Table D.3: Baseline differences between the EA off work sick and matched
comparison groups
| Comparison group | EA off work sick group | Matched comparison group | p-value |
|---|---|---|---|
| % | % | ||
| Gender | 0.865 | ||
| Male | 66 | 67 | |
| Female | 34 | 33 | |
| Age | 0.978 | ||
| 16-24 | 5 | 4 | |
| 25-34 | 17 | 21 | |
| 35-49 | 39 | 29 | |
| 50-59 | 29 | 27 | |
| 60 and over 66 | 9 | 9 | |
| Whether has a partner | 0.126 | ||
| Yes | 45 | 39 | |
| No | 55 | 61 | |
| Whether has children | 0.887 | ||
| Yes | 33 | 38 | |
| No | 67 | 62 | |
| Qualifications | 0.681 | ||
| Level 5 or over | 51 | 44 | |
| Levels 3 or 4 | 26 | 30 | |
| None or up to level 2 | 23 | 26 | |
| Length of time off sick before start of IAPT | 0.948 | ||
| Less than a month | 24 | 26 | |
| More than a months but less than 6 months/missing | 54 | 56 | |
| Six months or more | 19 | 18 | |
| Number of hours worked per week before start of IAPT | 0.717 | ||
| 30 or more | 79 | 83 | |
| 16-30 | 19 | 14 | |
| Fewer than 16 hours | 2 | 3 | |
| Presenteeism in four weeks prior to start of IAPT | 0.846 | ||
| No days | 22 | 24 | |
| Up to 5 days | 12 | 10 | |
| 5 to 10 days | 23 | 29 | |
| 10 days or more | 34 | 28 | |
| Missing | 10 | 10 | |
| Summary of work history | 0.386 | ||
| Spent most of my time out of paid work | 1 | 1 | |
| Spent about as much time in paid work as not | 4 | 4 | |
| Spent most of my time working | 95 | 96 | |
| Whether has a mortgage or debt | 0.516 | ||
| Yes | 62 | 55 | |
| No | 37 | 44 | |
| Not answered | - | 1 | |
| Longstanding health condition | 0.853 | ||
| Yes | 60 | 61 | |
| No | 40 | 39 | |
| Whether had anxiety at start of IAPT | 0.584 | ||
| Yes | 91 | 93 | |
| No | 9 | 7 | |
| Whether had depression at start of IAPT | 0.476 | ||
| Yes | 85 | 81 | |
| No | 15 | 19 | |
| Whether had stress at start of IAPT | 0.603 | ||
| Yes | 93 | 95 | |
| No | 7 | 5 | |
| Whether had other mental health condition at start of IAPT | 0.462 | ||
| Yes | 15 | 10 | |
| No | 86 | 90 | |
| Bases: | 227 | 70 |
As with the EA looking for work matched comparison group, there is a fairly large difference between the EA off work sick group and the matched comparison group in terms of qualifications. In the EA off work sick group the percentage with qualifications of Level 5 or above is 51 per cent, but just 44 per cent in the matched comparison group. Again, the small sample size in the matched comparison group means that these do not reach significance. A similar series of logistic regression models have been run for a range of the outcomes presented recalculated as binaries. For each of these regressions, the effect of the EA is estimated using the matching comparison group (that is, applying the propensity score weights) but in this instance also controlling for age, gender, length of time off work sick, presenteeism, and qualification level. As with the looking for work group, these tests suggest that the estimates of impact are not, in fact, markedly affected by the relatively poor match on length of qualifications.
Table D.4 shows the standard psm estimates of impact against the regression adjusted estimates for three binary outcomes: employed and working; with likely depression (as measured by the WHO-5); and seen a GP in the past two weeks.
Table D.4: Impact of Employment Advisers among those off work sick as
measured by psm and by psm with regression adjustments
| Off work sick and well-being | Impact measured using just psm (percentage point difference) | Impact measured using psm plus regression adjustment (percentage point difference) |
|---|---|---|
| Employed and working | -9 | -10 |
| Likely depression (WHO-5) | 2 | 1 |
| Seen a GP in last two weeks | -2 | -2 |
-
Hogarth et al. (2013) Evaluation of Employment Advisers in the Improving Access to Psychological Therapies programme. ↩
-
Loveless, L and others (2019) Employment Advisers in Improving Access to Psychological Therapies: process evaluation report ↩
-
Using propensity score matching. ↩
-
Hogarth et al. (2013) Evaluation of Employment Advisers in the Improving Access to Psychological Therapies programme ↩
-
Van Stolk et al. (2014) Psychological Wellbeing and Work ↩
-
IPS is an employment support service integrated within community mental health teams for people who experience severe mental health conditions. It provides intensive, individual support to people to help them to move towards and into or stay in employment. ↩
-
Loveless et al. (2019) Employment Advisers in Improving Access to Psychological Therapies: process evaluation report ↩
-
This was as opposed to a random sample of IAPT clients being shared with research partners andcontacted directly about the evaluation. ↩
-
Some records were duplicated or did not include useable contact information (i.e. a valid address or phone number). ↩
-
Some records were duplicated or did not include useable contact information (i.e. a valid address or phone number). ↩
-
Advance letters were not sent to individuals who took part in the Time 1 survey. ↩
-
Note that these were CCGs as they stood at the time of project inception, some mergers have taken place since, including with Camden CCG. Read more information on CCGs ↩
-
As a relative measure, ‘high deprivation’ was taken to include those CCGs sitting within the upper quartile (the upper 25 per cent) of the deprivation index, and ‘low deprivation’ as those within the lower quartile. Case studies were selected against a range of Indices of Multiple Deprivation (IMD) scores to include low, high and moderately-deprived areas. ↩
-
One client did not consent to a recording, so detailed notes were taken instead. ↩
-
Developed by Jane Richie and Liz Spencer (for use in large scale policy research, the approach utilises a matrix output: rows (cases – usually an individual research participant), columns (codes), and ‘cells’ of summarised data. This provides a structure into which the researcher can systematically reduce the data, in order to analyse it by case and by code. Richie, J. and Spencer, L. (1994) Qualitative data analysis for applied policy research. Analyzing qualitative data, Chapter 9 pages 173-194. ↩
-
Vuori, J. and Tervahartiala, T. (1994). Active job search and subjective health among the unemployed. Studies in Labour Policy 91. Helsinki: Ministry of Labour.; and Vuori, J. and Vesalainen, J. (1999). Labour market interventions as predictors of re-employment, job seeking activity and psychological distress among the unemployed. Journal of Occupational and Organizational Psychology, 72(4), 523-538. ↩
-
Birkin, R. et al. (2004) Can the activity matching ability system contribute to employment assessment? An initial discussion of job performance and a survey of work psychologists views. Corpus ID: 142375149; and Birkin, R. and Meehan, M. (2016). ↩
-
The WHO-5 has been shown to identify people with likely depression. ↩
-
IAPT services collect the Work and Social Adjustment Scale (WASAS) and not EQ-5D. ↩
-
Scoring was derived according to the utility weights developed by Dolan: Dolan, P.(1997) Modeling valuations for EuroQol health states. Med Care 1997 Nov;35(11):1095-108. doi: 10.1097/00005650-199711000-00002. ↩
-
This pathway was identified in the process learning phase. ↩
-
It is important to note that these three groupings are defined by client responses in the Time 1 survey; there is therefore a chance of recall error in terms of offers and take up of EA support. ↩
-
Note that this is based on UK data, not England. Data taken from the Survey of Personal Incomes ↩
-
Level 1 qualifications include GCSEs graded D-G, NVQs at level 1, Key Skills level, Skills; Level 2 include 5 GCSEs Grades A -C, GCEs O Level, CSEs Grade 1, NVQ Level 2, Level 2 VQs; Level 3 include two A levels, three AS levels, Advanced Extension Awards, International; Level 4 covers NVQs at level 4, Key Skills level 4, Certificates of higher education, BTEC; Level 5 or above covers undergraduate degrees (BSc, BA etc.), HNDs, Postgraduate certificates. ↩
-
Respondents were able to provide multiple responses, if applicable. ↩
-
When necessary, respondents were prompted from a list of possible reasons. They were also able to provide ‘other’ responses which were then coded to identify and group where there was commonality in ‘other’ responses. ↩
-
These findings should be taken with some caution due to relatively low base sizes - 136 for employed individuals who declined support and 64 for out of work individuals who declined support. ↩
-
Loveless et al. (2019) Employment Advisers in Improving Access to Psychological Therapies: process evaluation report ↩
-
Throughout this report case study names have been changed to protect participant anonymity and confidentiality. ↩
-
A structured method of replying to interview questions describing the Situation, Task, Action and Result (STAR). ↩
-
The Advisory, Conciliation and Arbitration Service (Acas) aims to improve organisations and working life through better employment relations, working with employers and employees to solve problems and improve performance. ↩
-
The latent benefits include social contact, time structure, status/identity, collective purpose, and enforced activity. ↩
-
Loveless et al. (2019) Employment Advisers in Improving Access to Psychological Therapies: process evaluation report ↩
-
For instance, the volume of change at the individual level (how often individual outcomes shifted positively, negatively, or not at all) over time. ↩
-
Indicated by a score of ‘4’ or ‘5 – Very’, on a five-point scale when asked how motivated they felt to stay in work. ↩
-
Note, however, that Chapter 5 presents no statistically significant evidence that EA support impacts on their propensity to be in employment 12 months later. ↩
-
Just under a quarter (23 per cent) of clients employed at the 12-month point were looking to change their role. ↩
-
A binary variable created based on the comparison group data to produce roughly equal splits between high and low activity groups. ↩
-
An outpatient appointment is when a patient is hospitalised for less than 24 hours. They do not necessarily need to stay overnight. This includes for example consultations, tests and scans. ↩
-
Appendix C provides impact estimates comparing EA support with the offer of EA support in areas without enhanced EA support. That is, these are estimates of EA support against a ‘business as usual’ model of offering EA support. The pattern of results is very similar to that presented here albeit, as expected, with smaller differences between the two groups. ↩
-
Although these outcomes were collected for those off work sick at the start of IAPT who subsequently became unemployed, the sample sizes are too small for analysis. ↩
-
It was not feasible to carry out a baseline survey in either Wave One or Wave Two areas ↩
-
For binary outcomes of around 50 per cent. ↩
-
Although those who were looking for work when they started IAPT but employed at the 12-month follow up were asked about their employment conditions and attachment to their job, the sample sizes are too small to report here. ↩
-
The 95% confidence interval around this estimate of 19 percentage points is very wide at (5pp,33pp). This reflects the small sample sizes. ↩
-
Job-search self-efficacy is the strength of an individual’s belief that they have the skills to undertake a range of job-search tasks. ↩
-
In the context of an impact study, there should be no filtering of samples based on outcomes, but to include ‘in work’ or ‘not looking for work’ as an extra category for each out of work statistic tended to obscure any differences for the out of work categories and the findings were difficult to interpret. ↩
-
Although those saying in this question that they are in work are not coded as in work at the employment status question. ↩
-
Although those who were off sick when they started IAPT but looking for work at the 12-month follow up were asked about job search activities, the sample sizes are too small to report here. ↩
-
Records with no definite outcome (i.e. they had neither converted to interview nor refused or been classified as unusable. ↩
-
Records that were attempted the maximum number of times (10), were not reached in the necessary call window (i.e. within two months of loading them into the survey; this ensured distance from IAPT start remained as consistent as possible), or numbers produced a deadline / were not valid on calling. ↩
-
Although those saying in this question that they are in work are not coded as in work at the employment status question. ↩