Laboratory surveillance of Enterococcus spp. bacteraemia (England): 2023
Updated 24 February 2026
Applies to England

© Crown copyright 2026
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/enterococcus-spp-bacteraemia-voluntary-surveillance-2023/laboratory-surveillance-of-enterococcus-spp-bacteraemia-england-2023
Introduction
The following analysis is based on surveillance of voluntary reporting of Enterococcus spp. bacteraemia reported by laboratories in England since 2014. Voluntary surveillance data for England was extracted on 21 February 2024 from both the communicable disease reporting (CDR) and antimicrobial resistance (AMR) modules of the UK Health Security Agency’s (UKHSA) Second Generation Surveillance System (SGSS).
Rates of laboratory reported bacteraemia were calculated using mid-year resident population estimates for the respective year and geography (1). Geographical analyses were based on the patient’s residential postcode. Cases were further assigned to 1 of 9 local area regions (UKHSA Centres), formed from the administrative local authority boundaries (2).
The report provides data on AMR trends and the geographical distribution of Enterococcus spp. cases, with further breakdown by species, age and sex. Antimicrobial susceptibility trends are based on SGSS AMR data and reported for the five-year period: 2019 to 2023.
A web appendix is available featuring the data presented in this report.
It should be noted that SGSS is a live database and therefore data is subject to change. As such, the data presented here for earlier years may differ from that in previous publications.
Note: Scientific names are not italicised in this report to ensure it is accessible by all users and complies with web accessibility legislation and associated guidelines.
Main points
The principal conclusions of this report are that:
- following a consistent rise between 2014 and 2021, the overall rate of Enterococcus spp. bacteraemia in England appears to have plateaued since 2021, with a rate of 16.0 per 100,000 population in 2023
- regionally, Enterococcus spp. bacteraemia rates in England ranged from 13.9 per 100,000 population in the North East to 19.2 per 100,000 population in the South West in 2023
- as in previous years, those over 75 years of age had the highest reported rates of Enterococcus spp. bacteraemia (76.6 per 100,000 population); the rate of Enterococcus spp. bacteraemia differed between sexes with males over 75 years (117.1 per 100,000 population) having a higher rate compared to females over 75 years (45.7 per 100,000 population)
- overall, males had a higher rate of Enterococcus spp. bacteraemia in all age groups, except for the 15 to 44 year age group where rates were similar between the sexes (males: 3.6 per 100,000 population and females: 4.4 per 100,000 population)
- in 2023, 91.0% of isolates from enterococcal bloodstream episodes were identified to species level; among identified species, the dominant species in 2023 was Enterococcus faecium (44.6%) followed by Enterococcus faecalis (42.0%) consistent with the previous 2 years
- the percentage of E. faecium isolates resistant to vancomycin increased by 4.1% and to teicoplanin by 3.8%; resistance to linezolid remained low at 1.5% in 2023
- in 2023, AMR in E. faecalis bacteraemia remained rare, at around 2% resistance to several antimicrobial agents (ampicillin/amoxicillin, vancomycin, teicoplanin) and 1% to linezolid; these resistance rates are consistent with that reported in previous years
Trends
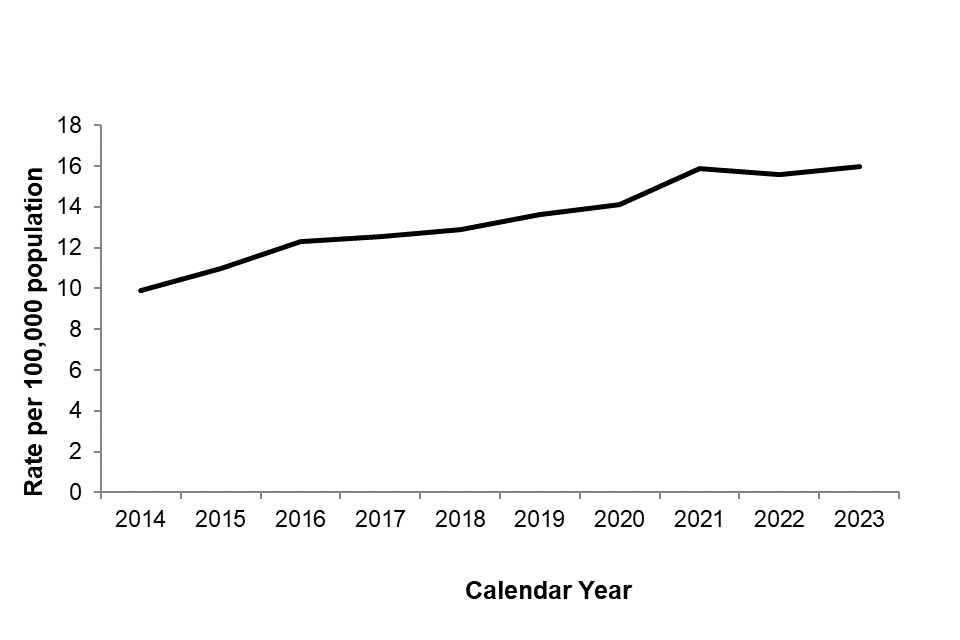
The rate of reported bacteraemia caused by Enterococcus spp. in England has increased year-on-year between 2014 and 2021 (Figure 1), from 9.9 per 100,000 population in 2014 to 15.9 per 100,000 population in 2021 (overall increase of 60.6%) but stabilised between 2021 and 2023. The rate of Enterococcus spp. bacteraemia in 2023 at 16.0 per 100,000 population. It should be acknowledged that the commencement of the COVID-19 pandemic in early 2020 influenced healthcare delivery and the overall composition of hospital patients in England (with an increased number of patients admitted to intensive care units (ICU) potentially affecting the rate of Enterococcus spp. bacteraemia.
Figure 1. Rate of Enterococcus spp. bacteraemia per 100,000 population in England: 2014 to 2023
Geographic distribution
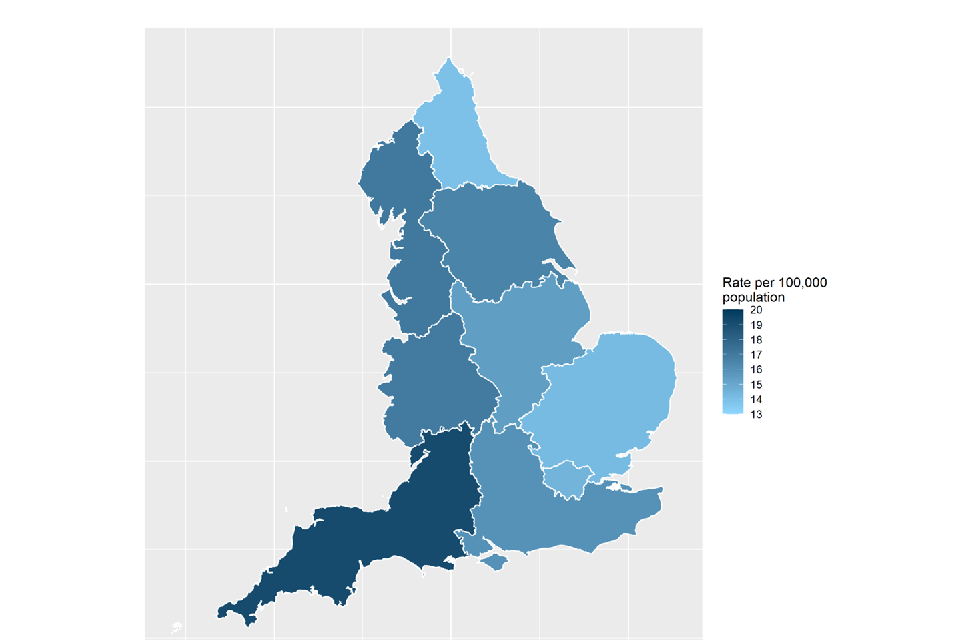
From a public health perspective, England is split into nine constituent geographical areas (local area region) and 4 geographical regions. In 2023, the local area region with the highest rate of Enterococcus spp. bacteraemia was the South West (19.2 per 100,000 population, representing an 8.5% increase compared to the previous year) (Figure 2, Table 1). The lowest reported rate in 2023 was in the North East (13.9 per 100,000 population).
Rates of Enterococcus spp. bacteraemia increased in all regions between 2019 and 2023, with Yorkshire and the Humber and the West Midlands having the highest percentage increases, with 35.8% and 32.1% increases respectively.
In the West Midlands, the rates of Enterococcus spp. bacteraemia increased by 10.4% between 2022 and 2023. To note, variation in reporting and the occurrence of local outbreaks, in addition to differences in local demographics, could potentially account for the differences between different regions observed.
Table 1. Enterococcus spp. bacteraemia per 100,000 population by region (England): 2019 to 2023
| Region / Local Area | Rate in 2019 | Rate in 2020 | Rate in 2021 | Rate in 2022 | Rate in 2023 |
|---|---|---|---|---|---|
| North East | 12.8 | 12.3 | 12.5 | 14.9 | 13.9 |
| North West | 15.3 | 15.9 | 17.6 | 17.0 | 17.0 |
| Yorkshire and Humber | 12.2 | 12.9 | 15.0 | 15.6 | 16.5 |
| East Midlands | 13.9 | 14.2 | 15.6 | 15.3 | 15.4 |
| East of England | 12.1 | 12.3 | 14.8 | 14.3 | 14.2 |
| West Midlands | 12.8 | 14.3 | 15.5 | 15.4 | 16.9 |
| London | 12.9 | 13.2 | 16.0 | 15.4 | 14.4 |
| South East | 13.8 | 15.0 | 15.6 | 14.6 | 15.9 |
| South West | 16.4 | 15.8 | 18.2 | 17.7 | 19.2 |
| England total | 13.6 | 14.1 | 15.9 | 15.6 | 16.0 |
Figure 2. Geographical distribution of Enterococcus spp. bacteraemia rates per 100,000 population (England): 2023
Species distribution
The most frequently reported species in 2023 was E. faecium (4,028 reports, 44.6%), followed by E. faecalis (3,792 reports, 42.0%) (Table 2).
Of the total Enterococcus spp. bacteraemia episodes reported in England in 2023, 91.2% were identified to species level, an increase from 2019 (89.2%) (Table 2).
Table 2. Reports of Enterococcus spp. bacteraemia by species (England): 2019 to 2023
| Enterococcus species | Reports (%): 2019 | Reports (%): 2020 | Reports (%): 2021 | Reports (%): 2022 | Reports (%): 2023 |
| Total | 7,620 (100.0) | 7,958 (100.0) | 8,973 (100.0) | 8,806 (100.0) | 9,038 (100.0) |
| E. avium | 60 (0.8) | 72 (0.9) | 80 (0.9) | 86 (1.0) | 73 (0.8) |
| E. casseliflavus | 77 (1.0) | 80 (1.0) | 85 (0.9) | 79 (0.9) | 119 (1.3) |
| E. durans | 16 (0.2) | 19 (0.2) | 22 (0.2) | 19 (0.2) | 12 (0.1) |
| E. faecalis | 3,289 (43.2) | 3,384 (42.5) | 3,636 (40.5) | 3,658 (41.5) | 3,792 (42.0) |
| E. faecium | 3,151 (41.4) | 3,364 (42.3) | 3,995 (44.5) | 3,992 (45.3) | 4,028 (44.6) |
| E. gallinarum | 97 (1.3) | 86 (1.1) | 117 (1.3) | 77 (0.9) | 101 (1.1) |
| E. raffinosus | 73 (1.0) | 72 (0.9) | 60 (0.7) | 84 (1.0) | 81 (0.9) |
| Enterococcus spp., other named ǂ | 16 (0.2) | 19 (0.2) | 19 (0.2) | 16 (0.2) | 18 (0.2) |
| Enterococcus spp., sp. not recorded | 841 (11.0) |
862 (10.8) |
959 (10.7) |
795 (9.0) |
814 (9.0) |
ǂ: Including E. canintestini, E. cecorum, E. columbae, E. gilvus, E. hirae, E. italicus, E. malodoratus, E. mundtii, E. phoeniculicola, E. saccharolyticus and E. thailandicus.
Age and sex distribution
As noted in previous annual reports, Enterococcus spp. bacteraemia is reported most frequently in younger and older age groups (Figure 3) (5).
Figure 3. Enterococcus spp. bacteraemia rates by age and sex (England): 2023
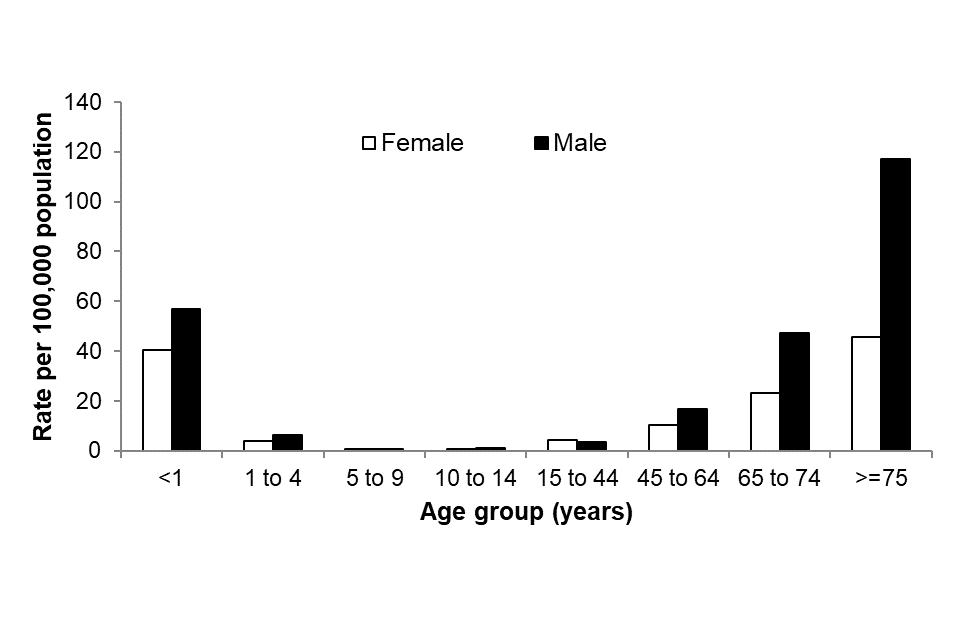
In 2023, as seen in previous years (6), the highest overall rate of bacteraemia caused by enterococci was in persons 75 years old and over (76.6 per 100,000 population). This was followed by under 1 year olds (51.1 cases per 100,000 population). In the rest of the paediatric population, the overall rate of Enterococcus spp. bacteraemia in the 1 to 4 year, 5 to 9 year and 10 to 14 year age groups was 5.1, 0.9 and 0.9 per 100,000 population, respectively (Figure 3). For more information on paediatric bloodstream infections, please refer to the Health Protection Report: Laboratory surveillance of paediatric bacterial bloodstream infections and antimicrobial resistance in England: 2018 to 2022 (6).
In all age groups, except in 15 to 44 years, males experienced a higher rate of Enterococcus spp. bacteraemia compared to females. Differences between rates in males and females were more prominent in the older age groups, particularly in the over 75 year olds (117.1 per 100,000 population compared to 45.7 per 100,000 population seen in females). Being male or being over 70 years old have both been associated with an increased risk of developing enterococcal bacteraemia (7).
Antimicrobial resistance
Resistance of Enterococcus spp. to glycopeptides (vancomycin or teicoplanin) is monitored in the English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) annual report (8).
The two most frequently isolated Enterococcus species are E. faecalis and E. faecium.
Between 2022 and 2023, the percentage of E. faecium isolates from bacteraemia episodes reported as resistant to vancomycin increased by 4.1% and teicoplanin by 3.8% (from 21.4% to 22.3% and from 22.9% to 23.8%, respectively). The percentage of E. faecium isolates that were resistant to linezolid remained low, at around 1.5% resistant in 2023 (Table 3a).
In 2023, resistance in E. faecalis bacteraemia remained rare with approximately 1-3% of isolates being reported as resistant to one of the selected antimicrobial agents (ampicillin/amoxicillin, vancomycin, teicoplanin and linezolid) (Table 3b).
The switch to E. faecium as the predominant species in England could have significant clinical and treatment implications in light of higher resistance rates compared to those seen in E. faecalis bacteraemia.
Table 3a. Antimicrobial susceptibility for E. faecium bacteraemia isolates (England): 2019 to 2023*
| ANTIMICROBIAL | 2019 | 2020 | 2021 | 2022 | 2023 |
|---|---|---|---|---|---|
| Ampicillin / Amoxicillin | |||||
| Number tested (n) | 2,877 | 2,917 | 3,501 | 3,385 | 3,108 |
| % susceptible | 9.1 | 7.6 | 7.9 | 8.5 | 7.8 |
| % susceptible, increased exposure | <1.0 | <1.0 | <1.0 | <1.0 | <1.0 |
| % resistant | 90.8 | 92.3 | 92.0 | 91.5 | 92.1 |
| Vancomycin | |||||
| Number tested (n) | 3,025 | 3,151 | 3,809 | 3,721 | 3,703 |
| % susceptible | 79.5 | 80.9 | 78.9 | 78.6 | 77.6 |
| % susceptible, increased exposure | 0.0 | 0.0 | 0.0 | 0.0 | 0. |
| % resistant | 20.5 | 19.1 | 21.1 | 21.4 | 22.3 |
| Teicoplanin | |||||
| Number tested (n) | 2,836 | 2,931 | 3,609 | 3,582 | 3,582 |
| % susceptible | 78.7 | 80.6 | 77.9 | 77.1 | 76.1 |
| % susceptible, increased exposure | 0 | 0 | 0 | 0 | 0 |
| % resistant | 21.3 | 19.4 | 22.1 | 22.9 | 23.8 |
| Linezolid | |||||
| Number tested (n) | 2,812 | 2,921 | 3,602 | 3,487 | 3,550 |
| % susceptible | 98.4 | 98.7 | 98.1 | 98.6 | 98.5 |
| % susceptible, increased exposure | 0.0 | 0.0 | 0.0 | 0.0 | <1.0 |
| % resistant | 1.6 | 1.3 | 1.9 | 1.4 | 1.5 |
*The isolates reported here have not all been confirmed by UKHSA’s Antimicrobial Resistance and Healthcare Associated Infections Reference Unit (AMRHAI). Isolates resistant to teicoplanin and susceptible to vancomycin are unusual and laboratories identifying this unusual combination should refer such isolates to AMRHAI.
Table 3b. Antimicrobial susceptibility for E. faecalis bacteraemia isolates (England): 2019 to 2023*
| ANTIMICROBIAL | 2019 | 2020 | 2021 | 2022 | 2023 |
|---|---|---|---|---|---|
| Ampicillin / Amoxicillin | |||||
| Number tested (n) | 2,906 | 2,796 | 3,164 | 2,998 | 2,922 |
| % susceptible | 98.4 | 98.2 | 97.8 | 98.3 | 97.8 |
| % susceptible, increased exposure | <1.0 | <1.0 | <1.0 | <1.0 | <1.0 |
| % resistant | 1.5 | 1.7 | 2.1 | 1.6 | 2.0 |
| Vancomycin | |||||
| Number tested (n) | 3,082 | 2,994 | 3,470 | 3,344 | 3,496 |
| % susceptible | 98.5 | 98.3 | 98.4 | 98.1 | 98.1 |
| % susceptible, increased exposure | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| % resistant | 1.5 | 1.7 | 1.6 | 1.9 | 1.9 |
| Teicoplanin | |||||
| Number tested (n) | 2,843 | 2,827 | 3,294 | 3,181 | 3,366 |
| % susceptible | 97.9 | 97.6 | 97.1 | 97.2 | 97.4 |
| % susceptible, increased exposure | 0.0 | 0.0 | 0.1 | 0.0 | 0.0 |
| % resistant | 2.1 | 2.4 | 2.8 | 2.8 | 2.5 |
| Linezolid | |||||
| Number tested (n) | 2,810 | 2,750 | 3,189 | 3,064 | 3,224 |
| % susceptible | 99.6 | 98.9 | 98.6 | 98.9 | 99.1 |
| % susceptible, increased exposure | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| % resistant | <1.0 | 1.1 | 1.4 | 1.1 | <1.0 |
*The isolates reported here have not all been confirmed by UKHSA’s Antimicrobial Resistance and Healthcare Associated Infections Reference Unit (AMRHAI). Isolates resistant to teicoplanin and susceptible to vancomycin are unusual and laboratories identifying this unusual combination should refer such isolates to AMRHAI.
Microbiology services
As noted previously, the ability to identify enterococci at the species level would assist in providing appropriate treatment regimes, in addition to monitoring trends of the most prevalent and emerging species (9).
Laboratories are requested to send any E. faecalis resistant to ampicillin/penicillin and any isolates with suspected linezolid or tigecycline resistance, and isolates that show resistance to teicoplanin but not vancomycin, to UKHSA’s Antimicrobial Resistance and Healthcare Associated Infections (AMRHAI) Reference Unit for further investigation (amrhai@ukhsa.gov.uk) (9, 10). AMRHAI will also examine isolates with suspected high-level daptomycin MICs (a daptomycin MIC for E. faecium >4mg/L and for E. faecalis >2mg/L), although it should be noted that there are no EUCAST clinical breakpoints.
For advice on treatment of antibiotic-resistant infections due to these opportunistic pathogens, laboratories should contact the AMRHAI Reference Unit in the first instance.
Acknowledgements
These reports would not be possible without the weekly contributions from microbiology colleagues in laboratories across England, without whom there would be no surveillance data. The support from colleagues within the UKHSA and UKHSA AMRHAI Reference Unit (10), in particular, is valued in the preparation of the report. Feedback and specific queries about this report are welcome and can be sent to hcai.amrdepartment@ukhsa.gov.uk
References
1. Office for National Statistics (ONS). Mid-year population estimates for England, Wales and Northern Ireland
2. UKHSA. UKHSA regions, local centres and emergency contacts
4. Buetti N and others (2021). COVID-19 increased the risk of ICU-acquired bloodstream infections: a case-cohort study from the multicentric OUTCOMEREA network. Intensive Care Medicine: volume 47 issue 2, pages 180 to 187
5. UKHSA (2021). Laboratory surveillance of Enterococcus spp. bacteraemia in England: 2020
6. UKHSA (2024). ‘Laboratory surveillance of paediatric bacterial bloodstream infections and antimicrobial resistance (England) 2018 to 2022’. Health Protection Report volume 18 number 10
7. Billington E and others (2014). Incidence, Risk Factors, and Outcomes for Enterococcus spp. Blood Stream Infections: A Population-Based Study. International Journal of Infectious Diseases: volume 26, pages 76 to 78
8. UKHSA (2022). English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) Report 2023-2024
9. PHE (2021). UK SMI ID4: identification of Streptococcus species, Enterococcus species and morphologically similar organisms
10. UKHSA (2022). UK Health Security Agency Reference Laboratories, Colindale: Bacteriology Reference Department user manual