Evaluating the Support for Migrant Victims (SMV) Pilot: Findings from a process evaluation
Published 4 August 2023
Applies to England and Wales

© Crown copyright 2023
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/evaluating-the-support-for-migrant-victims-smv-pilot/evaluating-the-support-for-migrant-victims-smv-pilot-findings-from-a-process-evaluation
Key terms and abbreviations
Acronyms
BIT: Behavioural Insights Team
DDVC: Destitution Domestic Violence Concession
DVILR: Domestic violence route to indefinite leave to remain
EEA: European Economic Area
ILR: Indefinite Leave to Remain
MV: Migrant Victim
NRPF: No Recourse to Public Funds
SMV: Support for Migrant Victims
Helpful terms
DDVC / DVILR: Destitution Domestic Violence Concession (DDVC) allows people who may be eligible to apply for ILR under the Domestic Violence Rule to access public funds whilst they make their application, if they can meet the basic initial test for domestic violence and destitution.
Section 17 : When Section 17 is referred to in this report, it relates to Section 17 of the Children’s Act 1989. This act places a general duty on all local authorities to ‘safeguard and promote the welfare of children within their area who are in need.
Core delivery partners
Southall Black Sisters[footnote 1] (London & South-East)
Founded in 1979 Southall Black Sisters is a non-profit London-based organisation which aims to challenge gender-based violence against women. They offer specialist advice, information, casework, advocacy, counselling and self-help support services in several community languages. Although originally set up to help black and minority women, they now support any women in need of emergency help.
Ashiana Sheffield (North East, Yorkshire and Humberside, and East Midlands)
Ashiana is an independent registered charity based in Sheffield and providing support to Black, Asian, Minority Ethnic and Refugee (BAMER) women across England. Through a mixture of in-house and partner provided support, Ashiana provide support with accommodation, personal safety, finance, parenting, substance misuse, domestic abuse, health, education, training and social integration as well as immigration and asylum advice.
Bawso (Wales)
Bawso was founded in 1995 and provides practical and emotional support to black, minority, ethnic (BME) women and migrant victims of domestic abuse, sexual violence, human trafficking, Female Genital Mutilation and forced marriage in Wales. Services provided include outreach and risk assessment, accommodation provision, subsistence, advocacy, legal and immigration support, access to medical services, training opportunities.
Birmingham & Solihull Women’s Aid (Birmingham and Solihull)
Birmingham and Solihull Women’s Aid provide frontline domestic violence and abuse support services to women and children in the Birmingham and Solihull area. The services they provide include advice and support via drop-in centres, emergency refuge accommodation, housing support and advice, community outreach, legal support (such as, criminal proceedings), family support and training for professionals.
Foyle Women’s Aid (Northern Ireland)
Foyle is a charity based in Derry and Londonderry, Northern Ireland, which aims to eliminate domestic abuse and sexual violence by supporting all victims of abuse. They provide a range of services including supported accommodation, family support and a support worker to help victims of abuse with their housing, legal issues and income and budget.
Shakti Women’s Aid (Scotland)
Shakti Women’s Aid is a charity that helps BME women, children, and young people in Scotland who are experiencing, or who have experienced, domestic abuse from a partner, ex-partner, and/ or other members of the household. In addition to the support provided as part of the pilot, Shakti also provide temporary refuge, key workers who provide practical and emotional support, consultancy and expertise (to help local authorities and others support victims of domestic abuse), as well as referrals to other support services.
Executive summary
Introduction
In July 2020, the Home Office (HO) announced the launch of a UK-wide pilot programme to support victims/survivors of domestic abuse who otherwise had no recourse to public funds (NRPF): the Support for Migrant Victims (SMV) Pilot. The Pilot was to run for a year “to support migrant victims of domestic abuse who do not have access to public funds to access safe accommodation”[footnote 2]. In the same month, HO commissioned the Behavioural Insights Team (BIT) to undertake an independent evaluation of the Pilot, in order to understand the current support available to victims/survivors with NRPF, whom the Pilot was supporting, the costs of the support, its outcomes, and the specific challenges associated with delivering it.
The independent evaluation consisted of 5 key elements:
Logic mapping workshop
- outline: development of a logic map describing the activities, outcomes, and mechanisms of the Pilot
- aim: inform the development of the research questions being used throughout the evaluation
Survey of support providers
- outline: survey of 75 different organisations that provide refuge services to victims/survivors (with access to funding and with NRPF)
- aim: understand the support available to victims/survivors of domestic abuse outside of the Pilot
Analysis of monitoring data
- outline: key data collected on 302 victims/survivors supported through the Pilot, including their demographics, support needs, support received through the Pilot, and some post-support outcomes
- aim: build a whole-programme picture of who the Pilot is supporting, the support being delivered, and the costs of delivering the support
Practitioner focus groups
- outline: 4 focus groups conducted at 2 timepoints, with managers and caseworkers from each of the delivery partners
- aim: understand the Pilot delivery, challenges faced with implementing it, and difficulties encountered by victims/survivors
Beneficiary interviews
- outline: 18 interviews with victims/survivors and ten interviews with their caseworkers
- aim: capture the experience and perceptions of victims/survivors associated with the Pilot, and build more depth of insight into outcomes
This evaluation only covers the initial Pilot period, from April 2021 to March 2022. However, HO is funding the SMV programme for a further year while they take on board lessons from the pilot; and will continue monitoring its delivery activity, outputs and outcomes to inform future policy on support for migrant victims of domestic abuse.
Key findings
Overall, our evaluation presents a mixed picture. There were clear examples of where the Pilot was performing well, particularly in meeting the immediate and emergency needs of victims/survivors. However, we also identified several areas in which victims’/survivors’ needs were not being fully met, where provision and experiences were highly dependent on the victims’/survivors’ specific circumstances, or where the administration of the Pilot placed additional burden on delivery partners.
Successes: the Pilot provided a valuable service to the 302 victims/survivors supported during its first year and filled gaps in other provision.
- outside of the Pilot, support for migrant victims with NRPF does exist; of organisations we surveyed, equal numbers provided support to those with and without RPF
- the Pilot provided emergency relief to victims/survivors that were in need, via immediate accommodation and subsistence with few barriers to access
- it worked well for those eligible for other sources of support, including DDVC and Section 17, bridging the gap between victims/survivors leaving the abusive relationship and accessing other funding sources
- the dedicated support provided by caseworkers was particularly valued by victims/survivors that were supported through the Pilot
- the Pilot provided benefits to the mental wellbeing of victims/survivors through targeted support (such as counselling and therapy) and incidental benefits from other aspects of the Pilot, including new social networks
Limitations and challenges: Pilot funding constraints made it hard for delivery providers to meet the complex needs of victims/survivors.
Sufficiency of provision
- subsistence payments provided through the Pilot were often not sufficient to cover basic expenses, and all delivery partners relied on relationships with local charities to bridge the gaps
- providing suitable accommodation within the constraints of the Pilot was a challenge for delivery partners
Complexity of cases
- many victims/survivors had complex legal situations which required more than 12 weeks to resolve - 31% (n = 93) victims/survivors were provided services for 12 or more weeks
- delivery partners did not always have the resources nor expertise to fully support victims/survivors with highly complex needs
- the language and cultural diversity of victims/survivors created additional challenges to provision
Local and regional constraints
- regional variation of available support services meant there were regional differences in terms of the quantity and quality of support provided
- the Pilot was sometimes bridging gaps in local authority provision where local authorities did not recognise their duties
Awareness of the Pilot
- awareness of the Pilot, among both potential recipients and other agencies and local services, was a barrier to effective provision
- victims/survivors were often unaware of their entitlements, and where the funding they received came from
Each of these key findings is covered more fully in Section 6: Discussion.
Conclusion
The aim of the Pilot was to provide a support net for victims/survivors of domestic abuse with no recourse to public funds, and it is meeting this aim in critical ways. In particular, the provision of accommodation and basic subsistence to victims/survivors removes a key potential barrier to them leaving the perpetrator. However, we also identified several areas in which the Pilot could better support victims/survivors and reduce the burden on providers delivering the Pilot.
Whilst it is outside our role as evaluators to provide policy recommendations, we hope that the insights contained within this report will help to provide the support needed to victims/survivors with NRPF.
1. Introduction
1.1 Background to this report
In 2017, the Queen’s Speech promised that the Government would bring forward a Domestic Violence and Abuse Bill, which was released in January 2019[footnote 3]. The Joint Committee, appointed in March 2019, published its report outlining their recommendations in June 2019[footnote 4]. The report outlined the Joint Committee’s assessment that the Bill had missed “the opportunity to address the needs of migrant women who have no recourse to public funds”. Furthermore, the report made the recommendation to explore ways to extend existing support for victims/survivors of domestic abuse with no recourse to public funds, such that vulnerable victims/survivors might access protection and support at a critical moment in their lives.
In July 2019, the Home Office published a response to the Joint Committee, in which the Home Office committed to review the overall response for victims/survivors of domestic abuse[footnote 5]. The findings were published in July 2020 and included in the conclusions was a commitment to allocate £1.5m towards a ‘Support for Migrant Victims’ pilot scheme (‘the Pilot’), which would be launched later in the year. The report outlined that the Pilot would offer emergency support to address gaps in existing provisions and gather information to help future funding decisions.
The Pilot was launched in April 2021. The Pilot has been delivered through 6 delivery partners: Southall Black Sisters (SBS) (the primary delivery partner who manages the Pilot funding), Ashiana Sheffield, Bawso, Foyle Women’s Aid, Birmingham & Solihull Women’s Aid, and Shakti Women’s Aid[footnote 6]. The services provided included accommodation services, legal support (partially funded by the Pilot), subsistence payments, counselling and support groups.
The purpose of this report is to present findings from an independent process evaluation of the Pilot conducted by the Behavioural Insights Team. The aim of the evaluation is to assess the following aspects of the Pilot:
- How the Pilot has been implemented. The process evaluation[footnote 7] aims to cast light on how the Pilot has been delivered, the profile of the victims/survivors who accessed it, and factors that affected how the Pilot was delivered.
- The journeys that victims/survivors took through the Pilot, including their outcomes. The second focus involves looking at how the journey and outcomes of victims/survivors aligned with the Pilot’s aims and how perceptions of the support provided contributed to those outcomes.
- Where the Pilot sits alongside existing support provided to victims/survivors. This helps us to understand the need for the Pilot and the gaps in provision it can potentially address.
1.2 Summary of research activities
To evaluate the Pilot, we conducted the following core research activities:
Focus groups with frontline Pilot delivery workers (practitioners)
These involved running focus groups with practitioners from across all delivery partners, which focused on understanding the implementation of the Pilot, gathering their perspectives on what has worked well, and what has worked less well.
Interviews with support recipients
We undertook in-depth interviews with recipients of the Pilot, focused on understanding the range of experiences of support and outcomes from it.
Analysis of monitoring data of recipients of the Pilot
We analysed data collected by the delivery partners throughout the Pilot to help understand who received support, including the type of support received.
We also conducted a logic mapping workshop at the start of the Pilot, to understand the core Pilot activities and how they would contribute to the intended outcomes of the Pilot from the perspective of the delivery partners.
In addition, we conducted a survey of support providers who offer assistance to victims/survivors of domestic abuse. The survey was used to understand the current support that victims/survivors are able to receive outside of the Pilot - including both those with recourse to public funds and those with NRPF. While it sits outside of the main focus of the evaluation (meaning, it did not directly contribute to the evaluation), it addresses the third aim of this evaluation: understanding where the Pilot sits amongst this support.
2. Methodology
This section provides a summary of the methodology for each component of the evaluation. More details on each can be found in the Annex – the relevant Annex is linked at the end of each subsection.
2.1 Logic mapping workshop
At the start of the evaluation, we conducted a logic mapping workshop with each of the core delivery partners, to better understand the support provided through the Pilot and its intended outcomes. The workshop was attended by at least one individual from each of the delivery partners, as well as individuals from the Home Office Analysis & Insight team overseeing the research, and was facilitated by BIT.
Through the workshop, we populated an online board with 4 features of the Pilot:
- target group
- activities
- intended outcomes
- intermediary outcomes
While the board was primarily populated by BIT facilitators based on the workshop discussions, the board was visible to all participants who were also able to add their own content. At the end of the workshop, the notes were formed into a structured logic map diagram, which was shared with workshop participants for comments. The finalised logic map formed the basis for the subsequent research questions and research design and may be found in Annex 8.1.
2.2 Research questions
Based on the activities and outcomes identified in the logic map and the prespecified aims of the Pilot evaluation, we developed specific research questions to help guide our evaluation of the Pilot. The questions focus on implementation (reach, fidelity, quality, responsiveness, and mechanisms), but also cover potential outcomes and the quality of the intervention. The questions are, however, restricted to the Pilot and its impacts – we are not evaluating the range of other programmes and measures that affect outcomes of migrant victims/survivors of domestic abuse. The overarching research questions are displayed in Table 1 below:
Table 1: Research questions
| RQ | Pilot delivery |
| 1 | How many victims/survivors are helped by the Pilot? |
| 2 | What is the profile of victims/survivors who seek support? |
| 3 | What support do victims/survivors receive through the Pilot? |
| 4 | Which parts of the Pilot were the most beneficial for victims/survivors? |
| 5 | What are the limitations of support provided through the Pilot? |
| 6 | What are the costs of providing this support? |
| 7 | Are delivery partners able to successfully deliver the Pilot? |
| Pilot outcomes | |
| 8 | What are the potential effects of the Pilot on victims’/survivors’ wellbeing? |
| 9 | What are the potential effects of the Pilot on victims’/survivors’ independence? |
| 10 | What are the potential effects of the Pilot on immigration outcomes? |
Specific sub-questions are presented in sections on each research approach. A full list of research questions, sub-questions and methods can be found in Annex 8.2.
2.3 Survey of support providers
We conducted an online survey of 75 UK organisations that provide support to migrant victims/survivors of domestic abuse. The main focus of the survey was on understanding which organisations provide support, the scale and costs of provision, and the profile of victims/survivors that come forward.
The survey was sent to organisations identified through 3 channels:
- organisations listed in the Women’s Aid Gold Book
- existing mailing lists, including the Women’s Resource Centre and NRPF Network
- organisations suggested by other survey respondents
We received a total of 93 responses and removed 10 seemingly duplicate responses[footnote 8]. This resulted in a final sample of 83 responses from a total of 75 different organisations (we received more than one response for 6 organisations).
2.4 Pilot monitoring data
Monitoring data was routinely collected by delivery partners throughout the Pilot. It was only collected when a victim/survivor left the Pilot, and therefore does not include victims/survivors who were still being supported at the Pilot end. Data were provided to BIT on a quarterly basis and comprised 302 individuals that had exited the Pilot by the end of quarter 4, January to March 2022 (a further 123 victims/survivors were still being supported at the end of the Pilot period).
Some delivery providers entered all victims/survivors for a quarter under the first month of that quarter (for instance, victims/survivors leaving the Pilot between October to December 2021 were all recorded under October 2021). Where this might affect our interpretation of the figures, we have noted this in the text.
2.5 Interviews
Interviews were conducted with 18 victims/survivors between February and May 2022.
Interviewees were identified through a mixture of purposive sampling and convenience sampling by delivery partners (more details are available in Annex 8.5). We generally achieved high diversity across our sample with respect to nationality, ethnicity, age, marital status and whether the victim/survivor had children. However, all our interviewees were heterosexual women, and we did not interview any victims/survivors support by Bawso (who did not share details of victims/survivors who were willing to be interviewed as part of the evaluation).
Interviews were semi-structured and followed a pre-agreed topic guide (see Annex 8.6.3). They were a mixture of in-person and remote, depending on the recommendations of the recruiting delivery partner. Interpreters were arranged when needed, and a safeguarding and distress protocol was in place to protect research participants (see Annex 8.3 for a full discussion of research ethics). All interviews were recorded and transcribed, before being analysed using the Framework Approach[footnote 9]. Co-coding was used to highlight any discrepancies in the interpretation of the data. In some cases, with the permission of victims/survivors, additional conversations were held with their caseworkers after the interview to better understand their case. Researchers made notes through these conversations (rather than recording them) which were considered alongside the main interview analysis.
Throughout this report, case studies and quotations have been anonymised to protect the identities of research participants.
2.6 Focus groups
Four online focus groups were conducted for this evaluation: 2 in January and 2 in March. One from each pair was conducted with programme managers, and one with caseworkers. We aimed to have one representative from each of the 6 delivery partners, but this was not always possible due to the limited availability of the caseworkers and Pilot managers. Conversely, some delivery partners sent 2 attendees for the manager focus groups. The spread of delivery partners and total attendees is presented in Table 2.
Table 2: Focus group attendees, by delivery partner
| Focus group | Delivery partner | Total attendees | |||||
|---|---|---|---|---|---|---|---|
| SBS | B&S | Ashiana | Shakti | Foyle | Bawso | ||
| Manager 1 | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | 6 |
| Manager 2 | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | 7 |
| Caseworker 1 | ✔ | ✔ | ✔ | 3 | |||
| Caseworker 2 | ✔ | ✔ | ✔ | 3 |
As with the interviews, focus groups were recorded and transcribed and analysed using the Framework Approach.
3. Existing support for victims/survivors
In this section, we summarise the context in which the Pilot was introduced, based on the findings of our survey, in which we collected data for 83 respondents from 75 UK organisations[footnote 10] that provide refuge services to victims/survivors with access to funding and with NRPF.
3.1 Summary of survey findings
The majority of organisations provide services to both victims/survivors with access to public funds and those with NRPF
Of the organisations we surveyed, the clear majority (76%, n = 63) provided services to both victims/survivors with access to public funds and those with NRPF. Of the remaining 24% (n = 20), equal numbers provided services to either victims/survivors with access to public funds (n = 15) or with NRPF (n = 15). Within our sample, therefore, a victim/survivor with NRPF would have access to support at the same number of organisations as a victim/survivor with access to funding.
Table 3: To whom services were provided by survey respondents, in order of descending frequency (n = 83)
| Provided services to victims/survivors with access to public funds | Provided services to victims/survivors with NRPF | Provided services to non-migrant victims/survivors | Proportion of respondents |
|---|---|---|---|
| ✔ | ✔ | ✔ | 70% (n = 58) |
| ✔ | 11% (n = 9) | ||
| ✔ | 7% (n = 6) | ||
| ✔ | ✔ | 6% (n = 5) | |
| ✔ | ✔ | 5% (n = 4) | |
| ✔ | ✔ | 1% (n = 1) |
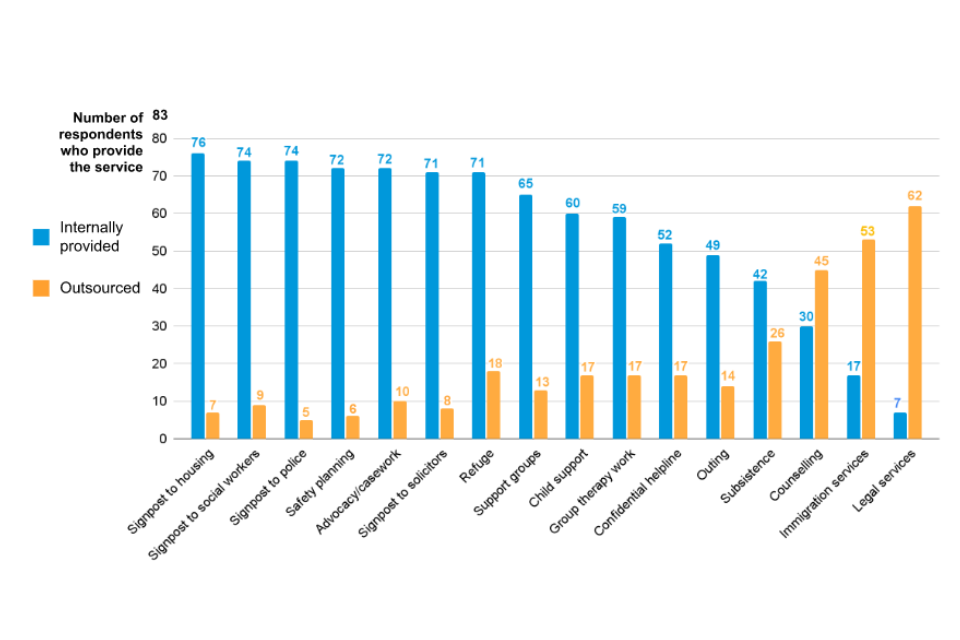
The most common services provided were refuge, signposting, advocacy, safety planning, and child support; less-common services often were outsourced
Respondents tended to provide the whole spectrum of services that victims/survivors require, including refuge, signposting, advocacy, safety planning, and child support[footnote 11]. More specialist services that may require specific training, such as counselling, immigration services, and legal services, tended to be outsourced.
Figure 1: Services provided (internally vs. outsourced) by respondents (n = 83)
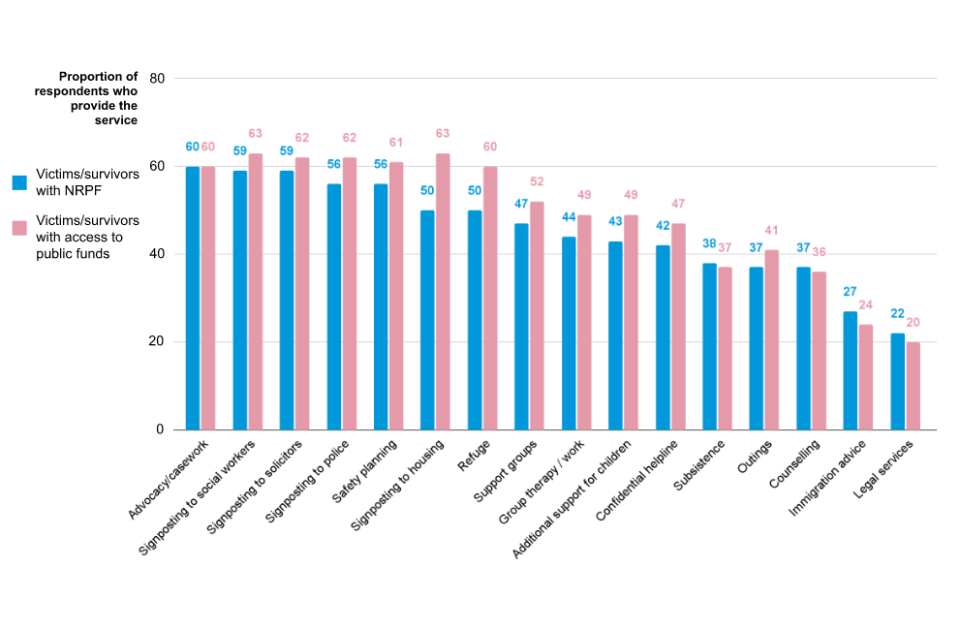
Signposting to housing and refuge were provided less to victims/survivors with NRPF than those with access to public funds
The biggest difference in service offerings between victims/survivors with public funding and those with NRPF was signposting to housing and refuge. As shown by Figure 2, these services were provided less often to victims/survivors with NRPF than those with access to public funds (63 respondents provided signposting to housing to victims/survivors with access to public funds versus 50 respondents to victims/survivors with NRPF; 60 respondents provided refuge to victims/survivors with access to public funds versus 50 respondents to victims/survivors with NRPF).
Figure 2: Services provided by respondent (victims/survivors with access to public funds vs. NRPF) (n = 83)
Lack of capacity and lack of funds were cited as the main reasons for service providers being unable to support more victims/survivors with NRPF
When asked why victims/survivors with NRPF were turned away, the most common reason provided (8 respondents) was that there was no capacity in the refuges for victims/survivors. Some respondents said that lack of funds meant they could not provide refuge (4 respondents), and required either housing benefits, a DDV concession or signed agreement from social services that they would provide funding. Respondents were clear that in cases where support couldn’t be provided, they would support victims with finding other services, or by referring them to other agencies or helplines.
Lack of funds was highlighted as being a barrier to multiple other services, including immigration support and legal advice
Respondents said that there often was not funding to support victims/survivors with NRPF, which limited how many victims/survivors they could support. DDVC is often relied upon in absence of other funding to provide access to refuge services; without it, many respondents could not provide housing. Others said that providing funding or housing was very challenging for victims/survivors with children where social care services are unable to provide funding.
Overall, the findings from the survey indicated that the lack of funding for victims/survivors with NRPF was a barrier for victims/survivors starting a life without the perpetrator, and that there was a strong need for funding to provide these individuals with refuge. These findings corroborated the rationale for the introduction of the Pilot, particularly the need for safe accommodation for victims/survivors who had just escaped abusive relationships.
3.2 Limitations of the survey findings
We took several steps to ensure our sample was representative, including:
- using snowball sampling and mailing lists to reach organisations that were not captured in the Gold Book to mitigate selection effects
- sending multiple reminders to potential respondents and keeping the survey open for several weeks, which increased the likelihood that individuals working in busy organisations had time to respond
However, our sample may not be representative of services that provide refuge in the UK for 2 key reasons:
- Services excluded from survey invites. Due to our sampling approach, we had to exclude any service providers that did not have an email address when identifying organisations to provide the survey link to. This may have excluded small service providers who do not have an email address. Moreover, as we only had one email address per organisation, it may have excluded organisations that have separate email addresses for different geographical regions[footnote 12].
- Services did not respond to the survey. We received a 30% completion rate for the original list of 355 organisations, which may have introduced selection bias into our sample. The organisations that did not respond may be different to those that did, meaning that our sample is not representative: for example, short-staffed organisations may not have responded due to their workload, and thus would not be represented in our survey.
A further limitation is data quality. In particular, the data quality for the questions relating to the number of victims/survivors supported was mixed – 36 respondents didn’t provide any data at all, with around half saying they didn’t know the answer. This adds an additional layer of selection bias in responses, if not knowing the answer also relates to the size of the organisation or the demographics of those they serve.
The organisations most likely to be excluded based on the limitations above are smaller organisations, who may be less likely to have a contact email and less likely to have accurate data. However, given that a quarter of our sample provided support to 10 or fewer victims/survivors, we feel we have captured at least some of these smaller organisations.
4. Pilot delivery
In this section, we discuss how the Pilot was delivered, including the number and profile of victims/survivors, and the support they received.
4.1 How many victims/survivors were helped by the Pilot? [RQ1]
302 victims/survivors were supported over the course of the Pilot – fewer than originally anticipated
Our analysis of the monitoring data indicated that 302 victims/survivors left the Pilot during the first 12 months of the Pilot (April 2021 to March 2022). We note that the monitoring data only captures victims/survivors who left the Pilot (meaning, the end of services funded by the Pilot) and therefore does not include victims/survivors still being supported at the end of the evaluation period (we have been told that a further 123 victims/survivors were still being supported). Importantly, we do not have data on the number of victims/survivors that sought help but were not able to receive it.
We understand that the Pilot had originally aimed to support between 500 and 1,000 victims/survivors between April 2021 and March 2022. We heard from the focus groups with practitioners that the COVID-19 pandemic may have made it harder for victims/survivors to find out about and seek support, which may have been why the final numbers were lower than anticipated. Table 4 presents the number of victims/survivors leaving the Pilot by service provider.
Table 4: Number of victims/survivors leaving the Pilot by service provider (n = 302)
| Service provider | Region of focus | Frequency of victims/survivors | Proportion of victims/survivors |
|---|---|---|---|
| Ashiana Sheffield | North East, Yorkshire and Humberside, and East Midlands | 23 | 8% |
| Bawso | Wales | 49 | 16% |
| Birmingham & Solihull Women’s Aid | Birmingham and Solihull | 71 | 24% |
| Foyle Women’s Aid | Northern Ireland | 17 | 6% |
| Shakti Women’s Aid | Scotland | 22 | 7% |
| Southall Black Sisters[footnote 13] | London & South-East | 120 | 40% |
The number of victims/survivors being supported by the Pilot increased over the course of the year
From the monitoring data we see that the number of victims/survivors leaving the Pilot generally increased across the course of the 12 months (see Figure 3). The distinct peaks at the start of each quarter (April 2021, July 2021, October 2021 and January 2022) are caused by some delivery partners recording all departures for the quarter within the first month, so overall figures by quarter are more reliable (see Table 5).
The largest increases were between:
- the first and second quarter (April to June 2021, compared with July to September 2021)
- the third and fourth quarter (October to December 2021, compared with January to March 2022)
The first and second quarter movement will be explained, in part, by the fact that these figures are departures from the Pilot. Many entries to the Pilot between April to June 2021 will be recorded in July to September 2021, and, unlike other quarters, no entries from a previous quarter will be recorded in April to June. The increase between the third and fourth quarters (October to December 2021 and January to March 2022) does not have a similarly mechanical explanation, but may have been caused by the increase in accommodation stipend between January to March 2022.
Figure 3: Number of victims/survivors leaving the Pilot by month (n = 302)
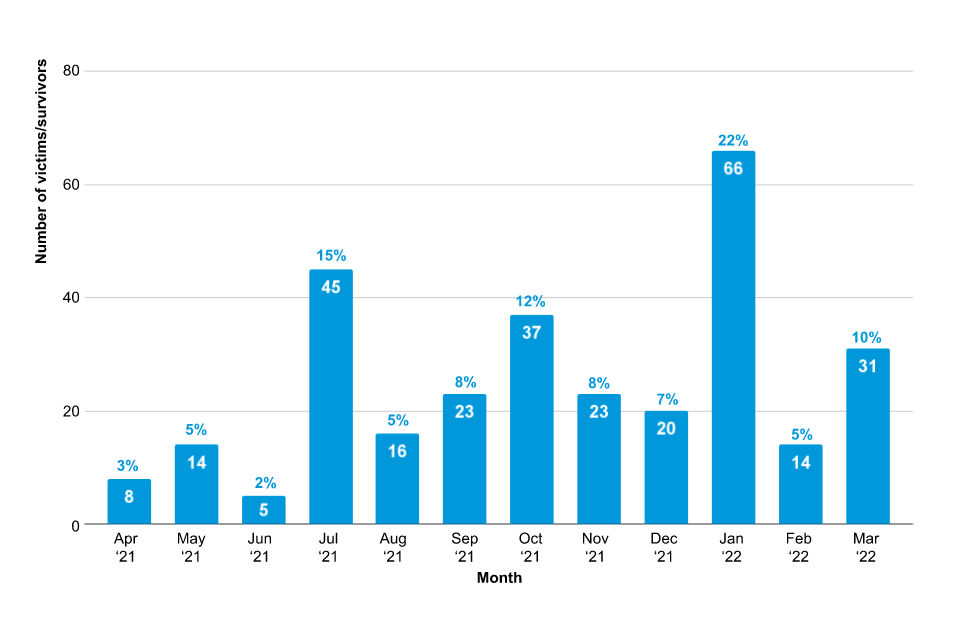
Table 5: Number of victims/survivors leaving the Pilot by quarter (n = 302)
| Quarter | Frequency of victims/survivors | Proportion of victims/survivors |
|---|---|---|
| Q1 (Apr - Jun ‘21) | 27 | 9% |
| Q2 (Jul - Sep ‘21) | 84 | 28% |
| Q3 (Oct - Dec ‘21) | 80 | 26% |
| Q4 (Jan - Mar ‘22) | 111 | 37% |
Victims/survivors found out about the Pilot through a range of channels
The focus groups and interviews we conducted highlighted that many victims/survivors assumed there would be no support for those with NRPF. Instead, some victims/survivors came to find out about the delivery partners - and subsequently the Pilot - in a moment of extreme need: for instance, by recommendation from the police after a severe incident of domestic abuse. It is important to note that victims/survivors found out about specific delivery partners, and how they could support them - but they did not necessarily understand how this support was funded and about the Pilot. We also found that there were other channels by which victims/survivors found out about the Pilot including:
- proactive contacting: victims/survivors looked online for organisations that supported women who faced domestic abuse, and directly reached out to the helpline
- suggestion by family members: victims’/survivors’ family members recommended they get in touch with a specific organisation
- police referral: when police are called to a severe domestic abuse incident, they usually provide victims/survivors with one or more organisations that they can contact for support
- GP referral: a number of victims/survivors said that they first heard of organisations that could support them while discussing their mental/physical health with their GP
- social services referral: some victims/survivors are in contact with social services, who gave them details of the delivery partners
- voluntary organisation referral: some victims/survivors were already in contact with other voluntary organisations; these bodies identified that victims/survivors and their children were experiencing domestic abuse and referred them to the delivery partners
- word of mouth: victims/survivors found out about organisations that may help them by hearing it from others: for example, hearing about it in a supported accommodation
Awareness of the Pilot may have been a barrier to uptake
Delivery partner staff reported that wider awareness of the Pilot was a key challenge in delivery, and that raising awareness of the Pilot was essential in ensuring that victims/survivors were referred to the Pilot. Before the Pilot, this type of support would not have been available for victims/survivors with NRPF, so services that typically refer them for support (as well as victims/survivors themselves) were often unaware that such support was now available. For example, some victims/survivors became homeless and were supported by a range of voluntary organisations who were unaware they could refer them to one of the delivery partners. Delivery partners reported doing extensive advocacy and awareness raising work with other community organisations, social services, and GPs to ensure all victims/survivors with NRPF would receive the support they needed. This included advocacy at the individual level (such as supporting victims/survivors with their specific case, and making sure other professionals were aware of the victim/survivor’s specific entitlements); and at the system level (for example, liaising accommodation providers, health services and other voluntary organisations to ensure they were aware that Pilot funding was available and encourage them to provide support or refer victims/survivors who would benefit from it).
“We have one of our caseworkers that has been doing some outreach work to make sure that other agencies and bodies know about this pilot, you know we need others to know this support is available to ensure that these women get the support they need.”
[Caseworker]
The lack of awareness of the Pilot and understanding of the funding available to victims/survivors with NRPF also created barriers for delivery partners who wanted to partner with other agencies to provide key services. Delivery partners reported having difficulty accessing support services, such as accommodation, due to agencies’ preconceptions that there was no funding available to support victims/survivors with NRPF. Delivery partners reported that because of these preconceptions, other agencies were concerned that providing services to victims/survivors with NRPF would be costly to them.
Delivery partners felt that awareness-raising and advocacy were key in addressing these issues. Delivery partners reported doing a lot of advocacy work with other agencies to publicise the Pilot:
“We’ve already mentioned all the awareness-raising that we’re having to do outside externally… because in [this city] we have got no accommodation providers.. so I had to do some advocacy and some awareness-raising with some of the supported accommodation providers, which is way out of my remit.”
[Caseworker]
It was also suggested that it would take at least a year to generate publicity for the Pilot which could help raise agencies’ awareness of the Pilot:
“We all know that for any project to start and to get its name, and the publicity, it takes a year. To raise publicity of this programme itself to take time to say there is money now, to the agencies as well, there is funds now, you can take women, that, in itself, is a big hurdle.”
[Pilot Manager]
The awareness raising activities conducted by delivery partners may also help explain the increase in the number of victims/survivors supported by the Pilot over the course of the year.
4.2 What is the profile of victims/survivors who seek support? [RQ2]
We analysed the monitoring data to assess the profiles of victims that were provided services by the Pilot. We note that we were unable to directly assess the profiles of victims that sought support (which includes both those who received support and those who were not able to receive it after seeking it). This was due to no data on the profiles of victims/survivors who sought help being directly available.
The profile of the victims/survivors leaving the Pilot is generally in alignment with the target group identified as part of the logic model. The exception to this is the inclusion of victims/survivors with children, as the expectation was that victims/survivors with children would receive support via social services under Article 17 of the Children Act 1989 - and thus not require support from the Pilot.
Victims/survivors tended to be female and heterosexual
The majority of victims/survivors tended to be female (97%; n = 294), and they also tended to be heterosexual (see Table 6).
Table 6: Gender and sexual orientation of victims/survivors that left the Pilot (n = 302)
| Sexual orientation | Female victims/survivors | Male victims/survivors |
|---|---|---|
| Bisexual | 2 | 0 |
| Gay or lesbian | 6 | 0 |
| Heterosexual | 270 | 5 |
| Prefer not to say | 7 | 0 |
| Unknown | 9 | 3 |
| Total | 294 (97% of total) | 8 (3% of total) |
Victims/survivors were predominantly Asian or Asian British, and Muslim
A narrow majority of victims/survivors were Asian or Asian British (51%, n = 154), and Muslim (51%, n = 154). While the most prevalent nationality was Pakistani (28%, n = 84), there was a spread of nationalities from across the world, as shown in Figure 4.
Figure 4: Nationality of victims/survivors (n = 302)
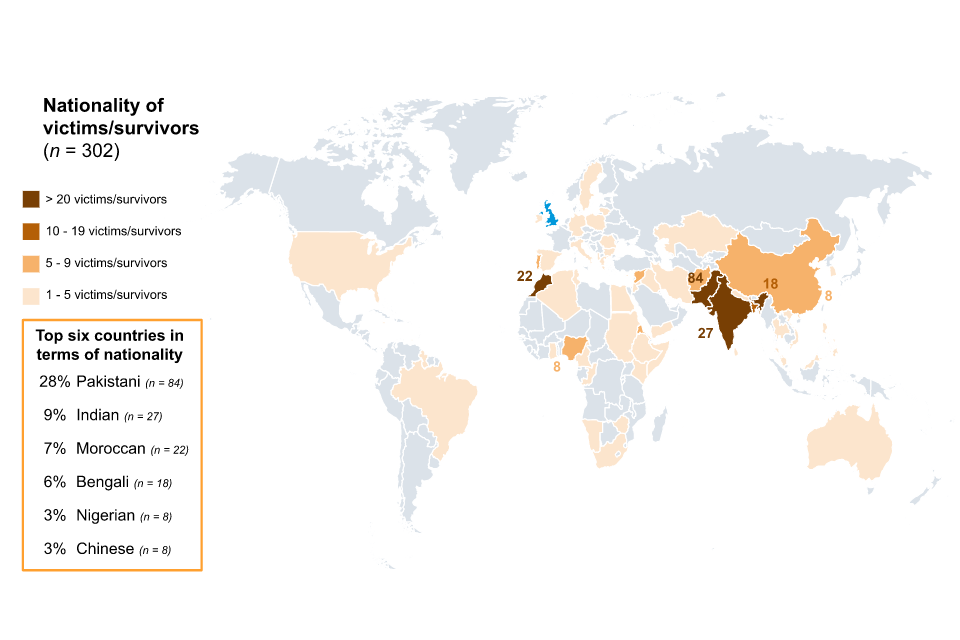
Table 7: Ethnicity of victims/survivors leaving the Pilot
| Ethnicity | Frequency of victims/survivors | Proportion of victims/survivors |
|---|---|---|
| Asian/Asian British | 154 | 51% |
| Black/African/Caribbean/Black British | 53 | 18% |
| Other | 40 | 13% |
| White | 29 | 10% |
| Arab | 14 | 5% |
| Prefer not to say | 7 | 2% |
| Mixed/Multiple ethnic group | 3 | 1% |
| Unknown | 2 | 1% |
| *Due to rounding, totals will not always sum to 100% |
Table 8: Religion of victims/survivors leaving the Pilot
| Religion | Frequency of victims/survivors | Proportion of victims/survivors |
|---|---|---|
| Muslim | 154 | 51% |
| Christian | 54 | 18% |
| Prefer not to say | 34 | 11% |
| None | 17 | 6% |
| Sikh | 13 | 4% |
| Catholic | 7 | 2% |
| Buddhist | 6 | 2% |
| Hindu | 5 | 1% |
| Other | 5 | 1% |
| Agnostic | 1 | <1% |
| Jewish | 1 | <1% |
| Zoroastrian | 1 | <1% |
| *Due to rounding, totals will not always sum to 100% |
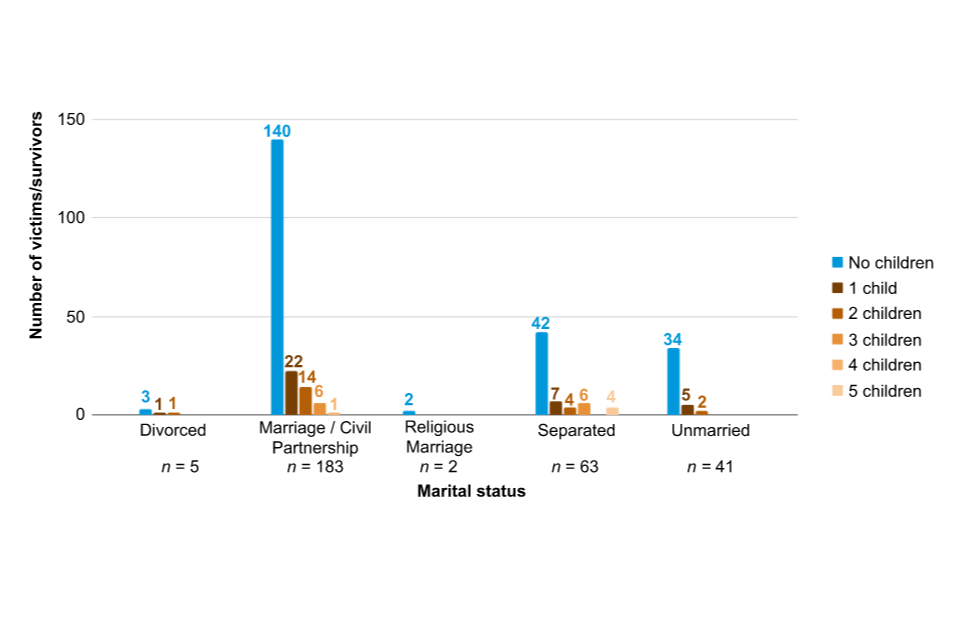
Most victims/survivors did not have children and were in a marriage or a Civil Partnership
The majority of victims/survivors did not have any children (75%, n = 221), and were either married or in a Civil Partnership (62%, n = 183).
Figure 5: Marital status and children of victims/survivors that left the Pilot (n = 294)
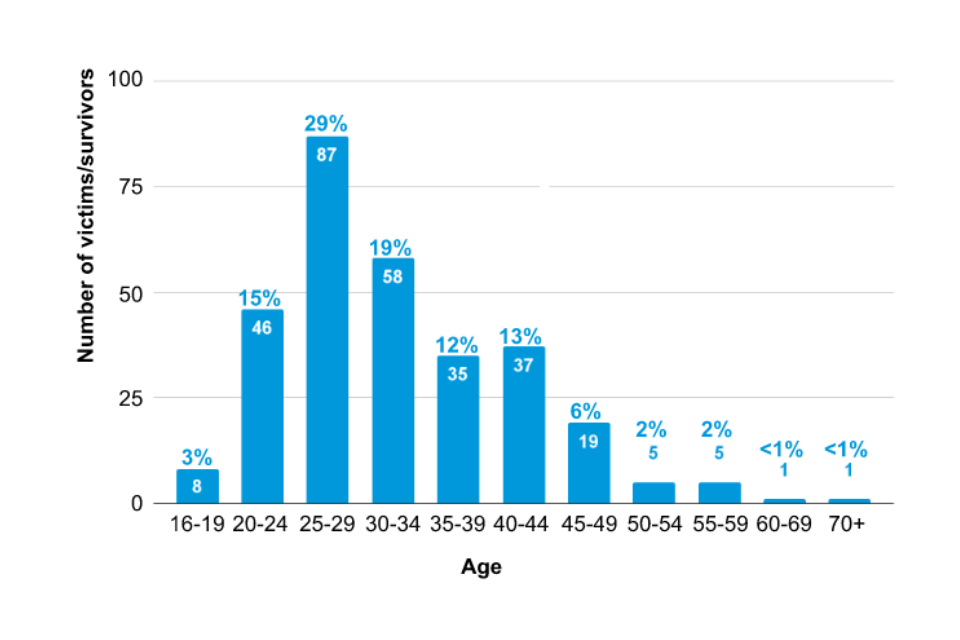
While there was a range of ages of victims/survivors, most were aged from 20 to 34
Figure 6 presents the range of ages of victims/survivors. The most common age bracket was 20 to 24 (29%, n = 87), but we saw a range of ages.
Figure 6: Age of victims/survivors that left the Pilot (n = 294)
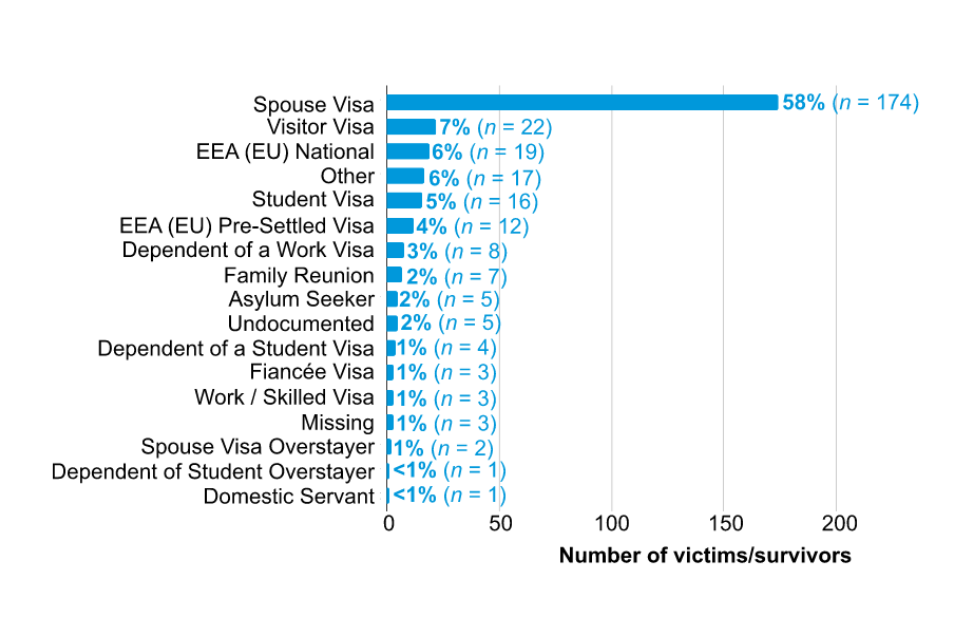
Most victims/survivors had Valid Entry Clearance as their immigration status on entry to the UK, and came into the UK on a Spouse Visa
The majority of victims/survivors entered into the UK on a Spouse Visa (58%, n = 174). An even greater majority had an immigration status of Valid Entry Clearance on entry into the UK (91%, n = 275).
Table 9: Immigration status on entry to the UK of victims/survivors leaving the Pilot (n = 302)
| Immigration status on entry | Frequency of victims/survivors | Proportion of victims/survivors |
|---|---|---|
| Valid Entry Clearance | 275 | 91% |
| No Valid Entry Clearance / Permission | 10 | 3% |
| Unknown* | 8 | 3% |
| Permission Granted at Border | 4 | 1% |
| Other* | 3 | 1% |
| Missing* | 2 | 1% |
* The monitoring data does not provide additional detail on the specific cases underpinning these variables. From the interviews, it appears that some victims/survivors had low knowledge of their immigration status and rights on entry, which may explain some unknown and missing data.
Figure 7: Route of entry into the UK of victims/survivors that left the Pilot (n = 302)
4.3 What support do victims/survivors receive through the Pilot? [RQ3]
In this section, we discuss the support that victims/survivors receive through the Pilot as a whole before discussing each service in detail, providing an overall description of the service that was provided, what worked well, and what could be improved for each service.
4.3.1 Overview of support
There were 6 broad stages of the Pilot for victims/survivors
Victim/survivor journeys through the Pilot were very diverse and depended on their needs, immigration status, and entitlements. However, the broad stages of the journey were similar across the majority of cases we discussed with caseworkers, managers, and victims/survivors themselves:
- Entry into the Pilot. Victims/survivors got in touch with the organisation either proactively by calling the helpline or when being supported by someone who is referring them.
- Needs assessment. Victims/survivors met with staff from delivery partners (usually their caseworkers) to discuss their story and their needs.
- Accommodation. In most cases victims/survivors were immediately placed in emergency accommodation to remove them from further danger or harm.
- Understanding eligibility. Victims/survivors discussed their eligibility for entitlements and visas with their caseworkers. Some discussed these with a solicitor.
- Receiving support. Victims/survivors received support such as accommodation, subsistence and counselling through the Pilot. Caseworkers provided them with ongoing guidance on next steps.
- Exit from the Pilot. Victims/survivors exited the Pilot usually by transitioning into another form of support, for example, receiving public funds through the DDVC, support from social services under Article 17, or asylum accommodation.
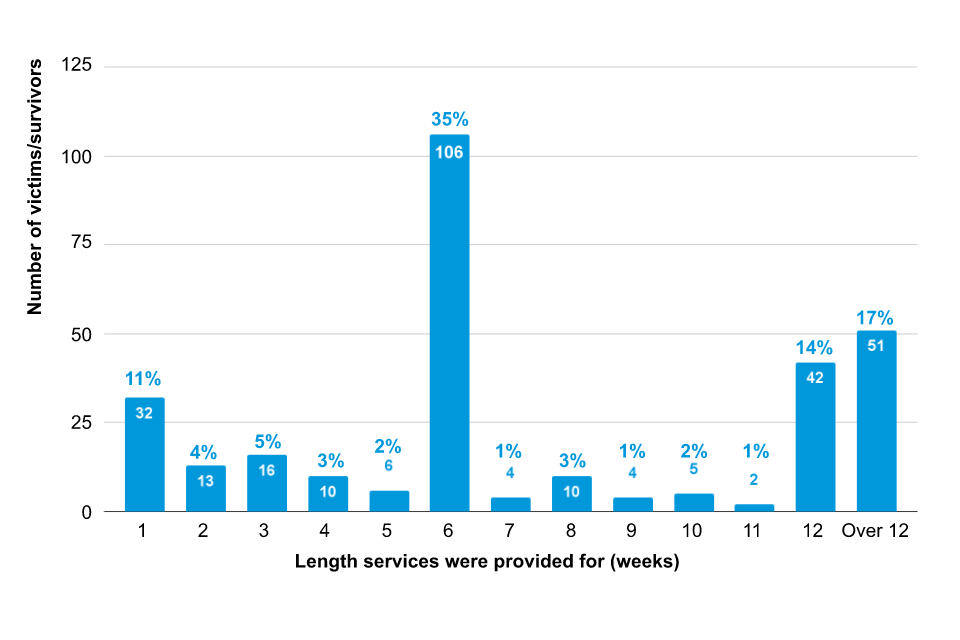
Most victims/survivors left the Pilot after either 6 weeks, or 12 or more weeks
The Pilot support was originally intended to last for up to 12 weeks per victim/survivor, or 6 weeks for victims/survivors eligible for DDVC. From January 2022 however, delivery partners were given more discretion to extend funding if needed.
Figure 8 presents the length of services provided to victims/survivors from the monitoring data (these figures are for any support as the monitoring data did not distinguish between lengths of support for different services). We see spikes in the number of victims/survivors supported for exactly 6 weeks (35%, n = 106) and 12 weeks (14%, n = 42), suggesting that in many cases victims/survivors were supported for as long as the Pilot would allow. In Section 5.1 we discuss these figures in relation to whether victims/survivors were granted DDVC, but the headline finding is that the majority (75%, n = 79 out of 106) of victims/survivors leaving the Pilot after 6 weeks had been granted DDVC, whereas those leaving after 12 weeks were very rarely leaving with DDVC (16%, n = 8 out of 51).
There was, however, a substantial proportion of victims/survivors supported for over 12 weeks (17%, n = 51), and this proportion was broadly consistent across quarter 1 to quarter 3 of delivery (April 2021 to December 2021) and quarter 4 of delivery (January to March 2022).
Figure 8: Length of services provided to victims/survivors leaving the Pilot (n = 301)
There was a diverse range of support provided, which broadly aligned with the provisions identified in the logic model
In the logic model developed with delivery partners, the core support provisions were identified as:
- safe accommodation
- subsistence payments
- legal support
In addition, the Pilot would “provide wrap-around support, included but not limited to: counselling services, support groups, translation and interpretation services.” (see Annex 8.1 for the full logic model).
Our interviews and focus groups provided more insight into this additional wrap-around support. In line with the logic model, a large part of this was wellbeing support including counselling and support groups. In-kind support, such as clothes, vouchers and access to phones and computers, was also an important part of this support. Caseworkers were not explicitly noted within the logic model, but it was clear from the qualitative research that they were a key aspect of the support provided. As well as helping victims/survivors access the other forms of support, they provided advocacy for the victims/survivors and were a source of emotional support and guidance.
The main types of support provided through the Pilot are summarised in Table 10 below. We elaborate more on each of these types of support subsequently in this section. However, it is worth noting from Table 10 that the funding for the Pilot was designed to cover some of these support types, but some were additional to the core Pilot support.
Needs assessments were used to identify the support each victim/survivor needed, but there was a lot of variation in their implementation across partners
In the logic model for the Pilot, developed with delivery partners, needs assessments would be regularly conducted with victims/survivors in order to identify the wrap-around support they needed. In practice, we found there was significant variation in how these were conducted.
We reviewed needs assessments from 2 delivery partners. Both contained information on the victims’/survivors’ history of abuse, their housing and financial situation, any health needs, whether they had children, and whether other agencies were involved in providing support. However, the structure and level of detail varied substantially. One was a reasonably succinct form, with 10 categories and corresponding actions required. A completed form was roughly 3 pages long. The other was very extensive, and included information on, for example, any ongoing court orders and victims’/survivors’ immigration status. It also included a DASH risk checklist, designed for assessing risk amongst victims of domestic abuse. A completed form was roughly 15 pages long.
Not all the providers conducted written needs assessments, instead conducting them verbally and more informally. We spoke to one of the delivery partners about this process and they were able to provide a detailed account of a victim/survivor’s identified needs but did not have a formal document for it. Similarly, one of the delivery partners working with SBS provided an email summarising the questions they asked of victims/survivors at the start of support, and the needs of the specific victim/survivor we had sampled for the needs assessment but noted they did not have a written document containing the assessment.
There was significant variation in the support received, reflecting the differing needs of victims/survivors
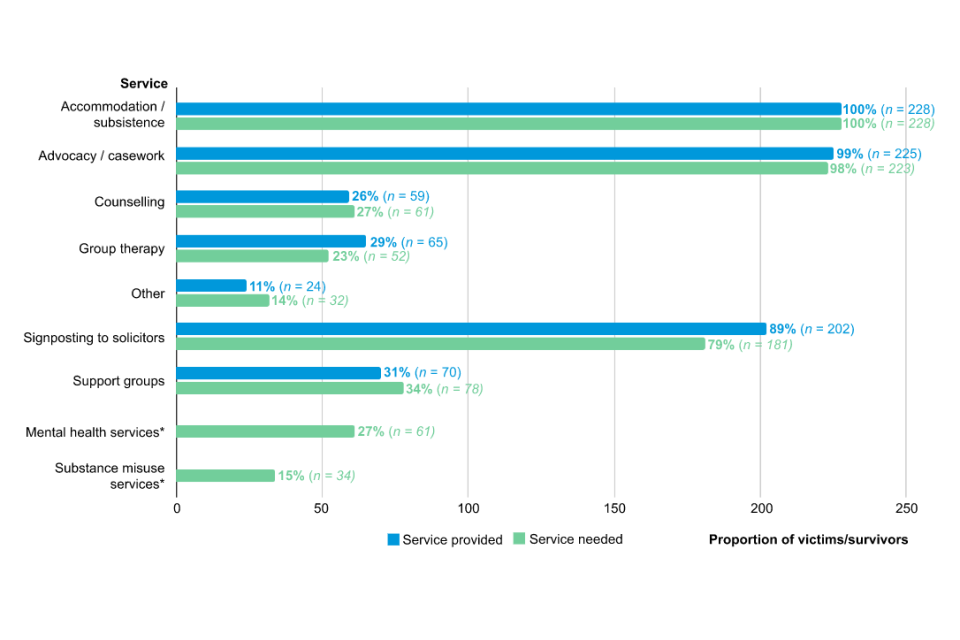
Figure 9 shows the percentage of victims/survivors receiving each type of support. While all victims/survivors received accommodation, and nearly all received advocacy/casework and signposting to solicitors, there is much more variation with counselling, group therapy, and support groups.
This appears to be driven, in large part, by the different needs of victims/survivors. Whilst there was variation in how needs assessments were conducted, the monitoring data included variables on the identified needs of victims/survivors. Figure 9 shows a generally close relationship between the proportion of victims/survivors that were identified as needing a service and the proportion who received it. There was also generally a strong correlation at the individual level between whether a victim/survivor was identified as needing a service and whether they received it. However, in some cases, a higher proportion of victims/survivors were identified as being provided with a service than were identified as needing it. This is particularly true for signposting to solicitors and group therapy. Figure 9 suggests that not all victims/survivors needed these services, indicating the difference with respect to the needs of victims/survivors who left the Pilot. We do not have clear evidence of why this was the case. However, some delivery partners said they provided group therapy as standard which may explain its overprovision. Similarly, signposting in itself is broadly costless, so may have been done as standard in many instances (which is consistent with the very high proportion [89%] of victims/survivors who were signposted to solicitors).
Figure 9: Proportion of victims/survivors receiving each service during the Pilot, relative to their identified needs (n = 228)[footnote 14]
The support provided also varied by delivery partner, which appears to be driven by differences in their offer
While some services were almost universally provided by all delivery partners, for other services there were substantial differences between delivery partners in how often they were provided. This was particularly evident for counselling, group therapy and support groups, as shown in Figure 10. Some providers offer some of these services but not others (Foyle, for example, offers group therapy and support groups to all victims/survivors, but does not offer individual counselling). We note that Birmingham & Solihull Women’s Aid did not offer any of these services, hence the figure displays 0% for all services.
It is important to understand that the support provided to victims/survivors was funded through a blended model, combining the Pilot’s and the delivery partners’ funds. This meant that the quality and offer of services often relied on how much additional funding delivery partners could provide.
Figure 10. Proportion of victims/survivors services were provided by delivery partner (n = 302)
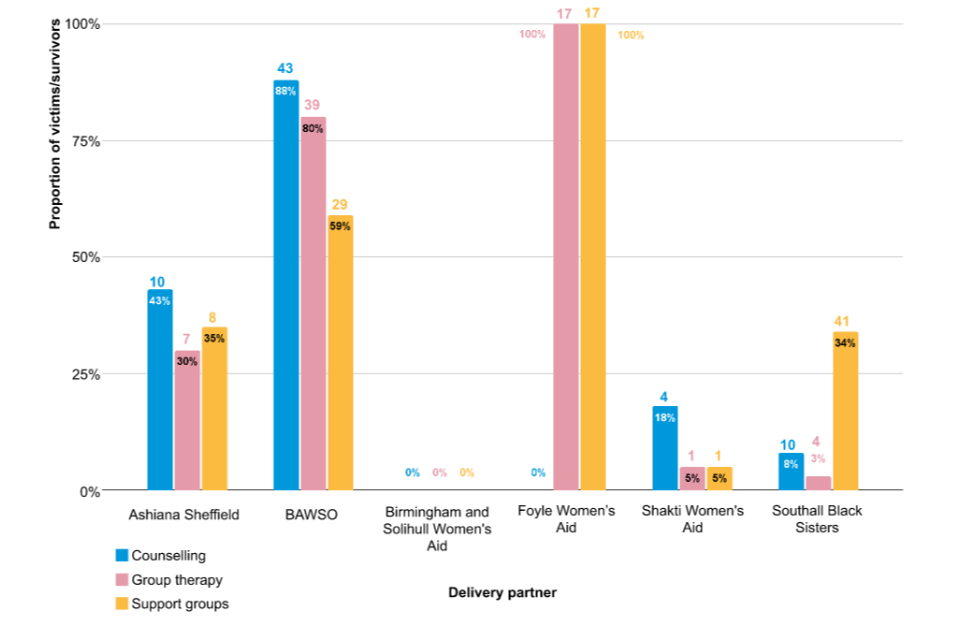
Table 10: Summary of support provided through the Pilot
| Type of support | Description |
| Accommodation (provided through Pilot funding) | Emergency accommodation was quickly provided to victims in need by organisations. Victims/survivors were mainly hosted in shared housing or other accommodation facilities such as vetted B&Bs with other victims/survivors with NPRF. Victims/survivors generally had an independent bedroom in the accommodation with shared communal spaces such as kitchens. Some had independent bathrooms. |
| Subsistence payments (provided through Pilot funding) | Subsistence payments ranged between £40 to £60 a week. Payments were initially £40 a week and then they increased to £50 a week, some delivery partners paid victims/survivors £60 a week. Some received it as a lump sum payment while others received it as a weekly instalment. Victims/survivors stopped receiving the subsistence payments when they had access to public funds. However, in some cases, delays and system errors meant that victims/survivors faced time gaps with no access to financial support. |
| In-kind support (not provided through Pilot funding) | Delivery partners supported victims/survivors to source other forms of in-kind support including things such as: Food from foodbanks. Smartphones. Essential travel. Internet access or mobile data. Toiletries including menstrual products. Vouchers for travel. Clothes. In-kind support was not funded through the Pilot but was sourced by delivery partners through other voluntary organisations. Access to these types of in-kind support was very heterogeneous as it depended on delivery partners’ networks. |
| Caseworkers (provided through Pilot funding) | Victims/survivors were assigned to a caseworker when they entered the Pilot - most had the same caseworker follow their case while some experienced changes in their caseworker throughout the Pilot. Caseworkers and victims/survivors had frequent debriefs. Caseworkers followed their case, providing emotional support, legal and bureaucratic support, signposting victims/survivors to other services. |
| Legal and bureaucratic support (partially provided through Pilot funding) | Delivery partners supported victims/survivors with their bureaucratic and legal needs in 3 ways: Through caseworkers or delivery partner staff. By signposting them to pro-bono legal advice. By applying for funded legal aid when eligible to apply for DDVC/DVILR, or by making an application for Exceptional Case Funding. Legal and bureaucratic support provided to the victims/survivors included: Support filling forms. Signposting to pro-bono solicitors. Support completing administrative tasks to settle immigration status (for example, providing their biometrics). Support putting the case to social services that they should be supported under Article 17. Providing interpreters. Support liaising with the police (for example, for document retrieval). Support setting up bank accounts to receive entitlements. Legal support to file for divorce. Legal support to understand immigration choices, and to complete application to settle status if eligible. Legal support to settle family legal disputes, for example, child custody. The Pilot did not directly fund legal aid for victims/survivors. The fund covered some of the delivery partners’ costs in finding pro-bono legal help or applying for legal aid, but not in its entirety. |
| Support for mental health and wellbeing (partially provided through Pilot funding) | Like other forms of support, wellbeing support varied greatly across providers. All victims/survivors received emotional support from their caseworker, others also received more tailored forms of support. Delivery partners provided wellbeing support in a number of ways to victims/survivors including: Regular catch-ups and debriefs with caseworkers. Support groups with other victims/survivors, offered in person or virtually. These sessions featured group activities such as dancing or creative writing. Therapy and counselling. Support accessing mental health care through the NHS, for victims/survivors with diagnosed mental health conditions. Occasional trips in the local area to places of natural beauty. Support finding volunteer work (for example, support finding them a volunteer role at a local charity shop). The Pilot covered the costs of the caseworkers’ work as well as therapy and counselling for many victims/survivors, but did not cover the costs of group support sessions or trips in the local area. |
4.3.2 Accommodation
Accommodation costs were capped at different levels for each delivery partner and accommodation type (for example, individual room versus ensuite). Some providers reported a cap of £80 per week, whereas for others it was as high as £250 (for ensuite rooms in high rent areas). The allowance increased in October to December 2021.
Emergency accommodation enabled victims/survivors to leave the perpetrator
Accommodation was one of the most valued parts of the Pilot by victims/survivors, who reported that access to the accommodation saved them from further physical or psychological harm and in many cases prevented them from becoming homeless. Many victims/survivors we interviewed entered the Pilot in a moment of crisis (for example, after an incident of severe physical abuse) or when they were homeless. Victims/survivors reported that once they had left the perpetrator, they had nowhere else to go because their families were not in the country, and many had been forced to socially isolate by the perpetrators. Because of these circumstances, emergency accommodation was an essential lifeline that helped victims/survivors in a moment of extreme vulnerability. Delivery partners were able to swiftly provide victims/survivors with accommodation in a moment of need. In some cases, victims/survivors were given access to emergency accommodation (for example, a hotel) and then relocated in shared accommodation with others in the longer term. The accommodation was provided entirely through the Pilot.
Victims/survivors were hosted in a range of accommodation types as delivery partners could not always accommodate victims/survivors in dedicated refuges
Delivery partners felt refuges would be the ideal place to host beneficiaries as they are situated in safe locations and offer a range of wrap-around services for guests such as childcare. However, this was not possible within the Pilot accommodation budget.
“We couldn’t afford our own refuges if you see what I mean, because the money was so under. We tried to find accommodation for £80 a week, it didn’t happen.”
[Caseworker]
“We couldn’t refer a woman to any refuges in [this city], which I think is the biggest issue that we’ve had. Although this may have also been because we had limited time [Pilot duration]. The wrap-around support that they could get in refuge would be ideal, let alone the main thing is, they would be safe. The accommodation we’re currently providing for women isn’t safe emergency accommodation. It’s just supported accommodation, which is just supported accommodation for homeless people.”
[Pilot Manager]
Instead, delivery partners met the accommodation needs of victims/survivors through a diverse range of accommodation arrangements, which included:
- vetted hotels and B&B: some victims/survivors were placed in vetted B&Bs or hotels; these were identified to be in secure locations, and many were already in use by social services; other victims/survivors were brought to an emergency hotel the first few nights and then relocated to another long-term facility
- shared housing with other victims/survivors: many victims/survivors lived in shared housing with other survivors (between 4 and 10 individuals) who also had NRPF; they typically had independent bedrooms and shared living spaces
- independent rentals: some victims/survivors lived in their independent accommodation which was paid directly by the Pilot
- supported accommodation: some victims/survivors were hosted in supported accommodation; these accommodations are designed to support people in need facing homelessness or substance abuse, rather than those experiencing domestic abuse
Delivery partners faced barriers in providing adequate accommodation because of issues in the amount, timeliness, and duration of funding
Delivery partners identified the primary reason for not placing victims/survivors in refuges as cost, as refuges could cost more than the accommodation stipend within the Pilot. However, they also reported that the structure of accommodation payments created barriers to obtaining adequate accommodation. Specifically:
- some accommodation providers were unwilling to take-on victims/survivors because they were unclear on how funding would be met after 12 weeks
- there were delays receiving the funding to cover accommodation costs from the Home Office, meaning that delivery partners had to self-fund in the interim
Even when accommodation costs could be met, some accommodation providers were reluctant to take victims/survivors in because the funding was only guaranteed for 12 weeks. Accommodation providers worried that they would be responsible for the victims/survivors after this point, but without any access to the funding to meet that responsibility:
“When we’re asking refuges or emergency accommodation, temporary accommodation, to take these women in, but saying, ‘For 12 weeks, we can pay you X amount of money,’ so the very first question they’re all saying is, ‘What happens after the 12 weeks?’”
[Programme Manager]
In addition, delivery partner staff flagged delays in receiving the funding from the Home Office to cover accommodation costs. For instance, towards the end of quarter 4 (January to March 2022), the delivery partners still had not received the funding to cover quarter 3 (October to December 2021). In the focus groups, delivery partners reported that delays in funding made it challenging to build a trusted relationship with accommodation providers:
“The other thing as well, is the time that you have to wait to actually receive the funding. Here we are, and we’re almost due to put in quarter 4, but we haven’t had quarter 3’s money yet. So, when we’re going back to refuges each quarter, or the other temporary accommodation providers. And they will say: ‘Well, you still haven’t paid me for…’ I don’t know if you are still waiting for your money from quarter 3, but it’s taking a lot of time to come through.”
[Caseworker]
The quality of the accommodation provided varied from good to very poor
While all victims/survivors were grateful for the accommodation and felt it enabled them to leave the perpetrator, there were high levels of variation in the quality of provision: some victims/survivors had overwhelmingly positive experiences, whereas others reported a number of issues.
Positive experiences
Many victims/survivors had very positive reviews of accommodation. Some living in shared housing or in vetted hotels and B&Bs felt that the accommodation was clean and spacious and had all the needed amenities. Many emphasised they valued having their own independent bedroom with their own privacy, and how they felt safe and supported in a women-only environment. In addition, victims/survivors generally felt that they were relocated to areas far from the perpetrators where they felt safe, this contributed to their wellbeing outcomes:
“I had my own room with a little bathroom and my own privacy where you can take back your mind and meditate again.”
[Victim/survivor]
“Everything was very comfortable. We had a very big kitchen which we share but in my room I have my bathroom.”
[Victim/survivor]
Negative experiences
Others that lived in shared housing, vetted hotels or B&Bs sometimes reported negative experiences. Key issues identified by interviewees included:
- lack of functioning amenities: some accommodation did not have basic amenities such as a working fridge, a stove or hot water; as put by one victim/survivor: “It’s okay but the fridge doesn’t work, it gets - it doesn’t get the power; the food gets rotten or food gets bad. The microwave doesn’t work. The cooker is also a bit broken”
- unhygienic living conditions: both victims/survivors and caseworkers reported that some accommodation was “filthy and full of rats”
- lack of understanding of victims/survivors situations: for some of those staying in commercial properties, such as B&Bs, issues arose when the accommodation providers did not understand the vulnerability of the victims/survivors they hosted; for example, one caseworker reported that a victim/survivor was asked to leave the accommodation because it was a particularly busy weekend, and the accommodation thought it could profit more from tourists
- experiences of discrimination from the local community: caseworkers reported that some accommodation facilities were situated in monocultural white British communities where victims/survivors faced discrimination and overt racism
- neighbours that may make victims/survivors feel unsafe: victims/survivors and caseworkers felt supported accommodation, in particular, was not suitable as it was designed to host homeless guests who are often male and suffered from alcohol or substance abuse issues
“The police took her to the hostel in [the location], and she wasn’t feeling comfortable there because there’s other, you know, alcoholic or drug difficulty there. We supported to move her from that hostel to the refuge place, which just has women there and just for other people including her.”
[Interpreter translating for victim/survivor]
4.3.3 Subsistence payments
Victims/survivors received a subsistence payment of £40 per week through the Pilot. In January 2022, this was increased to £50 per week.
Subsistence payments provided an important lifeline for victims/survivors
Victims/survivors highlighted that subsistence payments were crucial to their wellbeing and independence, and helped them cover basic needs such as:
- food: cash payments enabled recipients to buy food and cook their own meals; as well as being a basic need, this gave victims/survivors a sense of agency and independence, and positively impacted their wellbeing; some victims/survivors were able to cook recipes from their home country, which was a comfort to them
- toiletries: cash payments enabled recipients to purchase toiletries; those living with other peers would often pool their funds together to be able to afford necessities to meet their needs, such as buying menstrual products
- clothing: victims/survivors and their children had limited clothing and lacked basic items such as jackets or school uniforms for children as, in many instances, these items had to be left at the perpetrators’ homes, leaving victims/survivors without possessions
- transport: victims/survivors used transport to get to and from appointments, access shops and wellbeing support, and to stay connected with peers and networks
Having access to these basic needs enabled victims/survivors to leave the perpetrators and develop a sense of independence. Because of this, some highlighted subsistence payments as an aspect of the Pilot which was most beneficial to them:
“Yes, because I have the money now. Everything’s okay.”
[Victim/survivor]
“It’s a godsend because I was sitting there, about to be destitute, and you guys come in with a very nice lifeline, and I’m very grateful as well. It really helped with living expenses.”
[Victim/survivor]
There was some variation in both the amount of subsistence which victims/survivors received and the regularity of payments
In general, subsistence payments began soon after victims/survivors entered the Pilot. Victims/survivors mostly received payments in weekly instalments which were paid into their bank accounts. However, there was some variation in victims’/survivors’ receipt of subsistence payments: for example, one victim/survivor reported she had to wait 20 days from the point of leaving the perpetrator to her first payment. She then received £150 and another £450, 4 weeks later. Though the implications of the payment delays were not explicitly discussed, she said that she had needed to be very careful with money and relied on in-kind support and shop vouchers provided by the delivery partner for basic necessities such as food and toiletries:
“Since she left her marital house, and when she was about to live in the refugee house, not when she was in hostel, because…she was about 2 weeks in a hostel in [the location], then she moved to that refugee place. About 20 days after all in total, when she left her marital house, she received £150.”
[Interpreter translating for victim/survivor]
While the amount provided by the Pilot was consistent for all victims/survivors (£40 per week at first, and then £50 per week from January 2022), participants reported receiving subsistence payments which ranged between £40 per week to £60 per week, suggesting some discretion or subsidy by delivery partners. Subsistence payments also varied in delivery, with some being paid into bank accounts and others being paid via credit cards. In some cases, payments were also supplemented by shop vouchers, though this also appeared to be at the discretion of delivery partners. Victims/survivors expressed a preference for direct payments rather than vouchers, as this gave them agency over their expenditures:
“She found that because she is [short of] money, the voucher doesn’t give her the option to choose where she wants to use this money. She said she would prefer to have actual money rather than a voucher, then she can decide where she can use it. When she left her husband, she didn’t take much clothes and her personal things with herself. Now she’s quite, you know, it’s narrow for her where she’s able to use that money for.”
[Interpreter translating for victim/survivor]
Although subsistence payments provided an important lifeline, they were insufficient to cover basic needs victims/survivors
Despite being considered a vital lifeline, victims/survivors reported that subsistence payments did not comprehensively cover their basic needs, even after payments had increased to £50. The payments only partially covered food and toiletries, and other basic necessities such as clothing and essential transport were unaffordable to them. This problem affected those with children in particular, and was further aggravated by rising prices during 2022:
“I cannot do the travelling in this as well if I want to afford the tickets, I cannot, for bus tickets I cannot pay them.”
[Victim/survivor]
Victims/survivors who started receiving Universal Credit claimed that they were less concerned about their finances. They felt the Universal Credit was enough to cover all their basic needs without having to supplement it with in-kind support. Some also reported that since receiving Universal Credit, they valued gaining more autonomy over their expenditures by managing their own bills or paying their TV licence. As put by one of the victims/survivors who transitioned from Universal Credit from the subsistence payments:
“Money is better than before [now she is receiving Universal Credit], for sure.”
[Victim/survivor]
Some victims/survivors experienced periods during which they received no financial support because of delays in transitioning to other forms of support
While some victims/survivors received subsistence payments up to the point they started receiving other entitlements such as Universal Credit, others reported a time gap before receiving support. These gaps were due to delays and system errors in receiving entitlements. During this time, victims/survivors received no formal financial support and were dependent on the goodwill of delivery partners, peers in their accommodation, and charitable donations.
Case study - Delays in transitioning to Universal Credit leave victims/survivors without financial support
Shiza* came to the UK on a Spouse Visa. Though she has no children, she still struggled to manage on the £40-a-week subsistence payments provided and often had to visit the foodbank. Soon after entering the Pilot, she made an application for DDVC which should have been approved within 6 weeks. However, because of a system error and missing documents, her DDVC application and access to benefits was delayed. After 12 weeks, the subsistence payments stopped even though she was not yet receiving Universal Credit. For almost 2 months she had no financial support and she survived because other women in her accommodation shared their food with her - “even if it was just plain rice”. After waiting for 2 months, she finally started receiving Universal Credit and can now afford to pay for most of her basic needs.
*Case studies have been anonymised to protect the identities of victims/survivors.
In some cases, victims/survivors or caseworkers expected to transition to other forms of support within a given timeframe (for example, 6 weeks for those with DDVC), but unexpected delays in receiving these entitlements meant that the victims/survivors were left without income. Caseworkers felt that it was difficult to prepare for these unexpected errors and delays, and because of this, victims/survivors felt there had to be more flexibility in the duration of the financial support to ensure there was a smooth transition into receiving entitlements:
“I think the fund thing, we get it for 6 weeks, but some of the ladies, they don’t get their Universal Credit paid for nearly 8 weeks. Mine started off I think after 7 weeks, so obviously for one week I didn’t have anything. She did speak to the manager as well, and they said they can’t really do anything. I think they could do £40 at least until the start of Universal Credit.”
[Victim/survivor]
4.3.4 In-kind support
Delivery partners used in-kind support to provide for victims’/survivors’ basic needs which could not always be met by subsistence payments
Due to insufficient subsistence payments, delivery partners addressed a range of the victims’/survivors’ needs by sourcing in-kind support through their internal resources or through other voluntary organisations. Some victims/survivors relied on in-kind support such as food banks, vouchers, and charitable donations to access these items. In the focus groups, Pilot managers universally said that they had partnerships with food banks, as well as a range of other local charities. While these services were for victims/survivors both on the Pilot and otherwise supported by the delivery partner, Pilot participants sometimes received priority because their need was greater than those with recourse to public funds. Caseworkers and their clients stressed that supplementing needs with in-kind support was key to addressing victims’/survivors’ basic needs because of the insufficient amount received:
“Women’s Aid help us to link the food bank, yes, and give me food bank support. Also during every holiday, Christmas, they give me some voucher for food and a lot of children’s gifts, and a lot of whatever we need, just the daily clothes and that.”
[Victim/survivor]
Victims/survivors needed access to transport and digital devices to access their entitlements
The findings suggest that subsistence payments were insufficient to cover the costs of essential travel and access to digital devices. Victims/survivors needed to travel to progress their immigration applications (for example, provide biometrics) or family legal disputes. Many victims/survivors were living outside urban centres and could not afford trains to reach their destinations.
The findings also revealed how smartphones were often a necessity that enabled victims/survivors to receive entitlements and become independent of the Pilot. For example, victims/survivors required a bank account in order to receive the subsistence payments and Universal Credit. However, high street banks do not take clients without a settled immigration status. Instead, delivery partners used e-banking providers such as Monzo, which require users to download a dedicated app on a personal device. Victims/survivors mentioned in the interviews how they valued having access to their personal bank account:
“Benefits, yes, yes, yes, yes. They gave me [Delivery partner helped victim/survivor to open] bank [account]. Yes, yes, bank. We have open bank. That is my first time, then I have the bank account.”
[Victim/survivor]
4.3.5 Caseworkers
Victims/survivors attributed a range of positive outcomes to the guidance provided by their caseworker
Victims/survivors were supported through their journey by a dedicated caseworker, who provided them with a range of support. This included emotional support, bureaucratic and legal support, and sign-posting victims/survivors to other sources of support. Across the board caseworkers were deemed invaluable by victims/survivors - and one of the most highly valued aspects of the Pilot. According to victims/survivors, caseworkers played an important role in improving their wellbeing outcomes, independence outcomes and helping them to understand their immigration choices.
Emotional support through trusted relationships
During their journey through the Pilot, many victims/survivors developed a trusted relationship with their caseworker. Soon after entering the Pilot, victims/survivors were assigned a designated caseworker who conducted a needs assessment so they could offer tailored support to their client. From then on, caseworkers had frequent debriefs (weekly or more frequently) with their client to support them emotionally and to arrange the support they needed. Where possible, delivery partners also purposely matched victims/survivors with caseworkers who spoke the same language as their client. For instance, one caseworker mentioned she usually supports children, but because she was a Farsi-speaker the delivery partner asked her whether she wanted to support a Farsi-speaking SMV client. The caseworker felt that sharing the same language helped her develop a trusted relationship with her client and enabled her to provide her with the best support.
Victims/survivors emphasised how frequent debriefs with caseworkers were a central source of emotional support, which helped them regain their confidence and independence after they experienced domestic abuse:
“The best thing that [Caseworker] did was obviously calming me down and giving me hope that everything’s going to be fine. You’re going to be fine.”
[Victim/survivor]
“I think the most important thing for help is they gave me long-term company and mental support to encourage me leave my husband.”
[Victim/survivor]
Where we did encounter a negative experience of the caseworker relationship, it was due to the victim/survivor being assigned multiple caseworkers through the Pilot due to staff changes. The victim/survivor reported how this was highly distressing for her and delaying her access to entitlements, further underscoring the importance of the caseworker relationship:
“They had to change her support worker 3 times. This was quite traumatic because she had to re-tell her story several times, it also led to mistakes in filing her DDVC application which led to delays. She was receiving calls from unknown numbers which made her uncomfortable. She thought it was her husband and that scared her.”
[Interpreter translating for victim/survivor]
Support with legal and administrative processes
Caseworkers were essential to victims/survivors in navigating the legislative immigration process understanding which entitlements they could apply for. This also meant that caseworkers played a central role in guiding victims/survivors as they considered their immigration choices. For example, caseworkers supported clients to submit their DDVC application and were essential to victims/survivors with children, who in some instances had to argue for their right to be supported by social services. Caseworkers played a central role in advocating for their clients’ rights with Local Authorities (LAs) (for example where LAs did not recognise their duty to provide services, or there were disputes as to which LA was responsible). They were key in supporting victims/survivors to complete all the complex administrative tasks (for example, forms, paperwork, appointments) related to settling their legal family disputes and immigration.
Sourcing other forms of support to address victims’/survivors’ basic needs
Caseworkers played an important role in sourcing a wide range of support to address their clients’ basic needs. They tapped into their networks of voluntary organisations to signpost clients to additional support. For example, caseworkers found specific schemes for clothes donation, negotiated frequent access to food banks, and reached out to children’s charities to seek additional support for clients’ dependents. Caseworkers reported that because of the insufficient subsistence payments, they had to find alternative ways to address their clients’ essential needs. For example, one caseworker mentioned that she and colleagues would drive clients’ legal appointments in their own car:
“…because £40 point a week, especially if you have children, is not a lot of money to be living on. So, anything at all that can help, and if they’re travelling to different solicitor’s appointments, that all costs money too. So, we would take them. We would take them in our own cars and stuff.”
[Caseworker]
4.3.6 Legal and bureaucratic support
Delivery partners provided victims/survivors with essential legal and bureaucratic support
Victims/survivors entered the Pilot with a range of complex bureaucratic and legal needs, including having to understand their immigration choices, settle family disputes, and apply for support from local authorities. All victims/survivors received some level of assistance with these complex tasks from caseworkers, delivery partner staff (for example, advocacy managers), or legal professionals. Many also required translation, which the delivery partners facilitated. Interviewees emphasised how the uncertainty of their immigration status and entitlements created a lot of stress and anxiety, and receiving dedicated support contributed to improving their levels of wellbeing.
Victims/survivors were generally very pleased with the support received, especially when they were signposted to legal professionals:
“They [delivery partner] connect with the immigration lawyer and family lawyer, and my family lawyer helped me to attend the court and deal with everything between me and my husband.”
[Victim/survivor]
This was illustrated by one victim/survivor who said that the immigration solicitor she was referred to was able to help her settle her visa and entitlements more quickly than other women staying in her accommodation. She mentioned that other women who did not have access to this support had to visit the immigration office in person and retell their stories several times (which sometimes led to distress). Instead, she was able to submit everything swiftly and remotely with the support of her lawyer:
“All the ladies said to me as well that your visa was actually really quick, and the best thing was you didn’t have to go in, it was just over the phone.”
[Victim/survivor]
Delivery partners had disputes with local authorities over their duty to support children under Article 17 of the Children Act 1989
Both caseworkers and victims/survivors with children emphasised how obtaining support from social services under Article 17 was not straightforward. Because of pressure on funding (something that was exacerbated during the pandemic), social services pushed back on supporting victims/survivors by refusing to offer financial support and accommodation. Delivery partners mentioned local authorities were even less likely to provide support if the children were not UK nationals. Caseworkers and delivery partner staff had to navigate complex bureaucratic and legislative systems to advocate for the rights of victims/survivors. This included frequently liaising with local authority staff, nurturing relationships where possible, and raising disputes where necessary. Caseworkers mentioned that in cases where the local authorities refuse to support the victims/survivors, they were forced to take legal action against them:
“We will just legally challenge the local authority and we will go to court. We have absolutely no qualms about that. If they have children, there is a statutory duty. It’s not our responsibility and we won’t be made to feel that it is by anybody.”
[Caseworker]
However, because not all delivery partners had access to pro-bono or in-house legal support, some were unable to challenge local authorities’ decisions. This meant that some victims/survivors with children still did not receive the support they were entitled to. For example, some local authorities claimed that their duty was solely to support the children of victims/survivors, not the victim/survivor themselves. In these cases, local authorities would sometimes offer to support the children through foster care but not support the mother - an outcome that would have severe negative consequences for all. Whilst delivery partners provided support to victims/survivors in challenging these decisions, these cases emphasise how victims’/survivors’ ability to access their entitlements depended on the delivery partner’s capacity to influence local authorities and access professional legal support.
Case study - Local authority refusing to support mother of 2
Ju* is a mother of 2 who entered the UK from China on a fiancé visa. Her children are aged 7 and 9 and, despite having spent most of their life in the UK, are not British. She suffered a long period of psychological abuse from her partner or ex-partner. Her situation is complex, so she does not qualify for the DDVC, and social services are unwilling to support her. Ju’s caseworker has tried to convince the local authority that they should support Ju and her children. However, the local authority has pushed back offering to support her children by placing them in foster care and leaving Ju without any financial support – an outcome that Ju is very concerned about. Ju and her children are unable to return to China because of incredibly strict COVID-19 travel restrictions, which prohibit all entry. Ju is currently in the process of applying for a start-up visa, so that she can start working as a graphic designer. She is unsure she will be able to regularise her immigration status before her funding ends at 12 weeks. Both Ju and her caseworker are unsure of what will happen next.
*Case studies have been anonymised to protect the identities of victims/survivors.
The lack of funded legal aid was a barrier for delivery partners, who had to rely on conditional or pro-bono legal support
Funded legal aid was not covered by the Pilot and could only be accessed by applying through specific routes such as the DDVC or Exceptional Cases Funding (ECF). There are 2 issues with the lack of immediate funding for legal aid. First, delivery partners need to cover the initial legal costs to access conditional legal aid. Second, the lengthy processes to access funding means that victims/survivors cannot advance their cases and may depend on the delivery partners for longer than needed.
To access means-tested legal aid funding, partner staff needed to complete days of unfunded skilled work. According to one caseworker, submitting an ECF application can take up to 3 days of focused work. The costs of this work and any associated cost of training other staff to provide these services are not covered by the Pilot, or any other funded scheme.
Furthermore, the time lag to file the application and receive the funding meant victims’/survivors’ cases are delayed because of a lack of legal advice. Victims/survivors who qualify for DDVC need to wait for weeks until they receive legal aid, while those who do not qualify to face even higher barriers to accessing legal aid funding. As put by one of the caseworkers herself:
“If it’s a woman who’s escaping domestic violence, we can get the DDVC and then they can get legal aid, but before we get to that point or if the DDVC is refused, then you’re stuck at no way to move forward. The woman can’t get an outcome without a solicitor fighting her case, but we also can’t get a solicitor because there isn’t any money.”
[Caseworker]
Delivery partners relied on pro-bono consultancies or internal staff for legal advice
The quality and amount of the legal aid provided varied greatly across delivery partners because they had to rely on local networks of pro-bono legal consultants and internal resources. Delivery partners did much of the work themselves (especially for DDVC applications), sourced pro-bono consultants, or in some instances asked solicitors to take on the case on the basis that they will be paid when the client had funding - however, many solicitors were unwilling to do this.
This meant that delivery partners were in a precarious situation when it came to accessing legal aid. This was evidenced in the case of one delivery partner, who, after losing their only pro-bono lawyer, was unable to signpost victims/survivors to legal support:
“We don’t have the appropriate immigration lawyers to signpost to, there are a few across [the country], but they don’t do any pro bono work… so for us, that’s what has been one of the biggest barriers, is accessing that immigration advice… We lost our one and only immigration lawyer that would provide some pro bono work… So that has caused a really massive barrier in terms of signposting women for the immigration advice.”
[Pilot Manager]
One delivery partner highlighted that because they had lost the lawyer doing pro-bono work for them, they were now doing it all themselves, with the support of other internal staff who may have an understanding of the legal landscape. They felt that this was the only way forward to advance some cases. Another delivery partner said that they had received training to enable them to support victims/survivors with legal application forms, though they still relied on professional legal support for complex cases:
“We’ve had some training to help women to complete the application. So that’s why I’m able to help them directly to complete all the applications and follow the case, call out the resolution centre to find out the progress… but on more complex cases… we signpost them also to an immigration adviser or immigration solicitor.”
[Caseworker]
However, not all delivery partners felt qualified or able to support victims/survivors with legal applications or provide advice:
“We don’t do any of that side [providing legal support and advice] ourselves, because we’re not qualified immigration advisers, we don’t feel it’s appropriate - and potentially illegal for us to be giving out that advice anyway.”
[Caseworker]
Lack of legal support affected victims’/survivors’ outcomes within the Pilot and beyond
The varied provision of professional legal support had implications for victims’/survivors’ immigration choices and independence outcomes. Delivery partners reported that those without access to legal aid may decide to return to the abusive relationship or return to their home country, where it may be unsafe for them:
“Having a solicitor try and fight for your right of leave to remain in the UK when you’re on no recourse, it costs a lot of money. Thousands and thousands of pounds. The length of time that it takes for some women can be years, so you can just imagine the costs are just spiralling year-on-year, which when they’re no recourse, this is why a lot of them either go back to their abusive partners or they go back to their home countries.”
[Caseworker]
The lack of professional support from the start can lead to delays and errors, which meant further delays in victims/survivors receiving entitlements or being able to understand their immigration outcomes. Souma’s case study shows how the lack of professional legal assistance can have implications for how long women are supported by the Pilot:
Case study - Errors in submitting the DDVC application due to the lack of legal support
Souma* came from Pakistan and entered the UK on a Spouse Visa. She was meant to be supported through the Pilot for 6 weeks because her case was relatively straightforward. The delivery partner supporting her applied for DDVC so she could receive Universal Credit. However, the organisation was not able to seek help from a solicitor to review her application. The delivery partner submitted the application on her behalf, but with a few clerical errors. It took weeks to correct the error on the DDVC which implied long delays. Souma inevitably had to be supported through the Pilot much longer than needed.
*Case studies have been anonymised to protect the identities of victims/survivors.
4.3.7 Support for mental health and wellbeing
Victims/survivors received a range of mental health support, which was highly valued
Victims/survivors received a range of formal and informal wellbeing support throughout their journey, which was one of the most valued elements of the Pilot. The support varied across providers, but common practices included:
Emotional support provided by caseworkers. Victims’/survivors’ experiences of emotional support provided by caseworkers were very positive. Emotional support through frequent catchups was an integral part of everyday caseworker-client interactions:
“Every time I feel down, and I have something going on, it’s I have any medical issue, or I have mental issues I discuss with my support worker, and she guide me, and she support me.”
[Victim/survivor]
Referral to mental health treatment. Some victims/survivors were signposted and supported to access mental health treatment through the NHS, therapists, and counsellors. In some cases, therapy was directly funded by the Pilot. These services helped victims/survivors, who were in dire need of support because of their experience of abuse, as well as intersections with other conditions such as depression or anxiety:
“They [delivery partners] give us a counsellor, a therapist for free, who’s taking care of us. Try to help us mentally because when we arrive here, our mental health is not good. We are scared, we are panicky.”
[Victim/survivor]
Access to funded psychological support was not universal but depended on the delivery partners. Those who could not access this professional support felt they did not receive the level of support they needed:
“They don’t have expert counselling. They have staff, they support [us] but they’re [don’t have] expert understanding [of] psychological issues and give you [the] right advice for specific things. If there is any counsellor in one refuge who can give us advice and to do something for us regarding specifically for our mental health that will be brilliant.”
[Victim/survivor]
Group support sessions. Some delivery partners organised regular group support sessions for victims/survivors. These sessions were not covered by the Pilot but were funded by the delivery partners internally. Support sessions happened weekly and were an opportunity for people supported by delivery partners to come together to share their experiences and take part in activities to promote their wellbeing. Those who attended felt these sessions were incredibly valuable for their wellbeing and for forming peer networks with others with similar experiences:
“Well, that’s the beauty of this in [delivery partner] to have a support group where everybody comes together… on Wednesday, everybody comes to support groups so we can hear and see and feel again and understand one another. That it’s not you going through this and you are going through that. The support group is very important I would say.”
[Victim/survivor]
Case study - The impact of the weekly support group for victims/survivors
Patience* experienced violent physical and psychological abuse by her husband for many years. Since joining the Pilot, she now feels safer, but she still struggles with trauma. As put by Patience herself: “Sometimes, the memories come and you just feel sad for nothing or you just feel like you are down, somehow weak.” She says one of the things that has helped her most is coming to the weekly support group hosted by her delivery partner. In the support group, women like her come together to talk, exercise, and paint. They even started a writing club, working on a book collectively, in which they recount their stories. She has found the writing incredibly healing, and she is proud that the book was launched at her city’s library. She hopes that their stories will empower others to leave perpetrators.
*Case studies have been anonymised to protect the identities of victims/survivors.
To encourage and facilitate attendance, some delivery partners covered the cost of transport to sessions. Support groups were often hosted in urban areas where there were a number of clients, which meant that those living more remotely could not necessarily access this support.
“The support group is in [the city], so yes, we don’t have an office in [the other city]. We’re based in [the city], so there isn’t a support group in [the other city] for [victims/survivors].”
[Interpreter translating for victim/survivor]
Having too much free time negatively affected some victims’/survivors’ wellbeing, but volunteering and organised activities were a help
Victims/survivors were keen to learn new skills so that they could improve their wellbeing and better integrate into society once they had left the Pilot. Some started volunteering at local charity shops or supporting delivery partners by providing translation and ad hoc support. Others, on their own account, started courses and took English classes. Some delivery partners even organised day trips to local areas of natural beauty. All of these activities and courses were not funded by the Pilot but were arranged on a case-by-case basis.
However, the more general experience was that victims/survivors had a lot of free time, which led them to dwell on traumatic memories. Many stressed how they were keen to improve their English and literacy, which would allow them to be more independent in many areas of their life:
“Could be English courses or any other skills. It could be painting, art, anything, music or any physical activities like swimming. Something like that which we can keep ourselves busy… Yes, it’s important for me because if I’m busy somewhere else and I will think less about an activity and about things happened and I can help myself to busy somewhere, to focus for a specific time with things which I don’t want to remember.”
[Victim/survivor]
In some cases, victims’/survivors’ financial situation or immigration status meant they were unable to participate in activities to support their wellbeing. This was especially the case for victims/survivors whose immigration status was unresolved, as these victims/survivors were discouraged by solicitors and others from taking part in activities such as volunteering:
“That was my personal suggestion, to try to join some of this charity to just do voluntary, but some solicitor and the other people said unless you didn’t get the final result from the Home Office, you’re better to not go anywhere, don’t join.”
[Interpreter translating for victim/survivor] SHA-02-SU17
There was significant variation in the level and types of wellbeing support offered to victims/survivors
As highlighted in Figure 10, the likelihood of a victim/survivor accessing counselling, group therapy or support groups varied substantially by delivery partner. In general, there was a correlation between the level of each type of support within a given partner – delivery partners that frequently provided counselling were also more likely to regularly provide access to group therapy or support groups. A notable exception is Foyle’s, where group therapy and support groups were universally provided, but individual counselling was not offered.
Whilst other forms of wellbeing support were not captured within the monitoring data, we found some evidence of similar variation in their provision through our interviews with victims/survivors. For example, the number and types of trips varied by delivery partner, as did other forms of support (such as the provision of childcare) which could contribute to victims’/survivors’ wellbeing.
4.4 What part of the Pilot is most beneficial to victims/survivors? [RQ4]
All forms of support offered to victims/survivors were needed and valued - as evidenced in detail within the sections on different types of support. To summarise, the most successful elements of the Pilot were:
The Pilot provided emergency relief, which enabled victims/survivors to escape the perpetrators
Victims/survivors received support quickly after getting in contact with the delivery partners. This was key in order to remove them from the risk of further physical and psychological harm. Victims/survivors swiftly accessed accommodation and subsistence payments which were vital lifelines and allowed them to leave the perpetrator without becoming homeless and destitute. They were also quickly linked to a dedicated caseworker, who assessed their needs, and guided them on next steps in terms of their immigration status and access to entitlements.
The Pilot worked particularly well for those who were transitioning to other sources of support – particularly for those eligible for DDVC and for many with children who could access support from local authorities. The Pilot provided emergency relief to enable victims/survivors to access these forms of support, which were not immediate, known of, nor easily accessible without a high level of understanding of British institutions.
The dedicated support provided by caseworkers for victims/survivors was particularly appreciated by Pilot beneficiaries
Victims/survivors felt the emotional and logistical guidance provided by their caseworkers was one of the key elements of the Pilot that enabled them to gain their independence. Support workers played a key role in providing ongoing emotional support, which enabled victims/survivors to regain their confidence, process trauma, and leave their abusive relationship. Caseworkers also helped victims/survivors understand their immigration choices and entitlements and carried out the bulk of the work when it came to administrative tasks and advocating for their client’s rights. Finally, caseworkers signposted victims/survivors to a range of services including therapy, legal counsel, and in-kind support to address their needs.
The wellbeing support provided through the Pilot was highly valued by victims/survivors
Pilot beneficiaries reiterated time and time again how much they valued the formal and informal wellbeing support offered throughout the Pilot. They emphasised the role of caseworkers, peer networks, and therapy as key in enabling them to overcome psychological trauma. They also emphasised how the ongoing guidance which enabled them to understand their immigration choices and access entitlements was key in supporting their wellbeing and reducing their anxiety.
The Pilot had unintended positive consequences
While the Pilot was primarily focused on providing a safe environment for victims/survivors and enabling them to leave circumstances of abuse, there were positive effects of the Pilot support that went beyond this immediate need. These included:
- peer networks: victims/survivors formed peer networks with others who had similar experiences and/or cultures, which provided them with invaluable emotional support; victims/survivors reported how these peer networks helped them to gain independence following the programme, for instance by making it affordable to move into a shared council housing
- personal development: some victims/survivors were able to pursue courses, improve their English, and improve their employability by volunteering; some delivery partners were able to facilitate these opportunities for specific victims/survivors; for example, victims/survivors reported that delivery partners helped them get a volunteer role working in a charity shop
- digital and financial inclusion: through the Pilot, victims/survivors received digital devices, access to the internet, and were supported to open bank accounts; these were key resources and systems that reduced their marginalisation and enabled them to access their entitlements
4.5 What are the limitations of the Pilot? [RQ5]
The support was too short for victims/survivors with complex circumstances
While the Pilot worked for those who were eligible for other forms of support (for example, DDVC or local authority provision), it worked less well for those with more complex immigration circumstances. The delivery partners (and in some cases the victims/survivors we spoke to) generally felt the 12-week duration was too brief for those who had uncertain immigration statuses. For example, for those who were forced overstayers, had had their documents destroyed, or experienced delays in accessing entitlements due to bureaucratic errors, the fixed duration of the funding was problematic. In some cases, victims/survivors experienced periods where they received no financial support from the Pilot. This often put a lot of pressure on delivery partners who stepped in to breach the gap for victims/survivors they had started supporting. Delivery partners felt that, in the last quarter of the Pilot, there was greater flexibility and extensions became an option for complex cases, but this had not been clearly communicated to all caseworkers and managers. There was no clarity on how long support should last exactly, both delivery partners and survivors/victims were convinced that duration of support should be dealt with on a case-by-case basis.
Subsistence payments were often insufficient to meet the basic needs of victims/survivors
Subsistence payments – even when increased to £50 per week – were insufficient to cover the basic needs of victims/survivors, especially when they had children. This was shown by the fact that victims/survivors had to rely on foodbanks and other voluntary organisations to cover basic needs food and clothing. Subsistence payments were also insufficient to cover the costs of essential travel to legal appointments and internet devices, which were essential tools for victims/survivors to access their entitlements. The qualitative research suggests that having subsistence payments would be sufficient if they matched Universal Credit.
There was a high variation in the quality of accommodation, legal support, in-kind support, and wellbeing support
There was substantial variation in the type and quality of support across regions and delivery partners. The quality of accommodation, legal advice, and in-kind support depended on the local networks of the delivery partners and their ability to source these services with extremely limited resources - or on a completely unfunded basis. Accommodation quality varied because delivery partners had to identify low-cost providers in the area. Legal and in-kind support was almost entirely pro-bono and depended on local availability and networks. Finally, many providers internally funded a range of activities for victims/survivors. These included support groups, day trips and English courses, and were incredibly valued by those who had access. However, the specific activities depended heavily on the provider.
Victims/survivors may benefit from more activities to promote their independence and wellbeing
Some victims/survivors felt that the Pilot could offer activities to help them gain key skills for life in the UK and improve their physical and psychological wellbeing. Many, who did not speak English or had low literacy, stressed how having English courses would have helped them to gain their independence in many areas of their life. Others mentioned how learning new skills that make them more employable would also be beneficial. Suggested activities were not always about developing new skills however, and many mentioned that more group activities and physical exercise would improve their wellbeing substantially.
4.6 What are the costs of providing this support? [RQ6]
From our analysis of the monitoring data, we calculated the total cost of services provided to the 302 victims/survivors who left the Pilot as £729,000 (3 s.f.) - an average of £2,455 per victim/survivor.
Accommodation / subsistence services were the highest cost with respect to total cost and cost per victim/survivor
Table 11 below presents the total costs by service, the proportion of victims/survivors who received the service, and the average cost per victim/survivor who received it. The most costly service in terms of average cost per recipient and total cost, was accommodation / subsistence. Notably, the monitoring data did not differentiate between accommodation and subsistence, so we were not able to distinguish between the costs for these services. We also find that advocacy / casework was both a high total cost and a high average cost per recipient.
We note that the proportion of victims/survivors who received each service in Table 11 are different than those presented in Figure 9. This is because of some data entries saying that victims/survivors received a service, but no cost was provided due to data collection issues.
Table 11: Cost of services provided to victims/survivors who left the Pilot
| Service | Total cost | Proportion of victims/survivors who received the service | Average cost per recipient* |
|---|---|---|---|
| Accommodation / subsistence | £452,759 | 97% (n = 293) | £1,545 |
| Advocacy / casework | £187,887 | 76% (n = 230) | £817 |
| Counselling | £24,820 | 17% (n = 51) | £487 |
| Support groups | £28,140 | 19% (n = 57) | £494 |
| Signposting to solicitors | £23,984 | 48% (n = 144) | £167 |
| Group therapy | £11,410 | 10% (n = 31) | £368 |
| * [footnote 15] |
Accommodation/subsistence and advocacy/casework services had the most variation in costs across delivery partners
Figure 11 shows the average cost per victim/survivor by service by delivery partner. We note that accommodation/subsistence and advocacy/casework services had the most variation in costs, whereas the other services were typically more aligned. This may be due to regional differences in costs of accommodation and salaries for caseworkers.
Figure 11: Costs of services by delivery partner by service (n = 302)
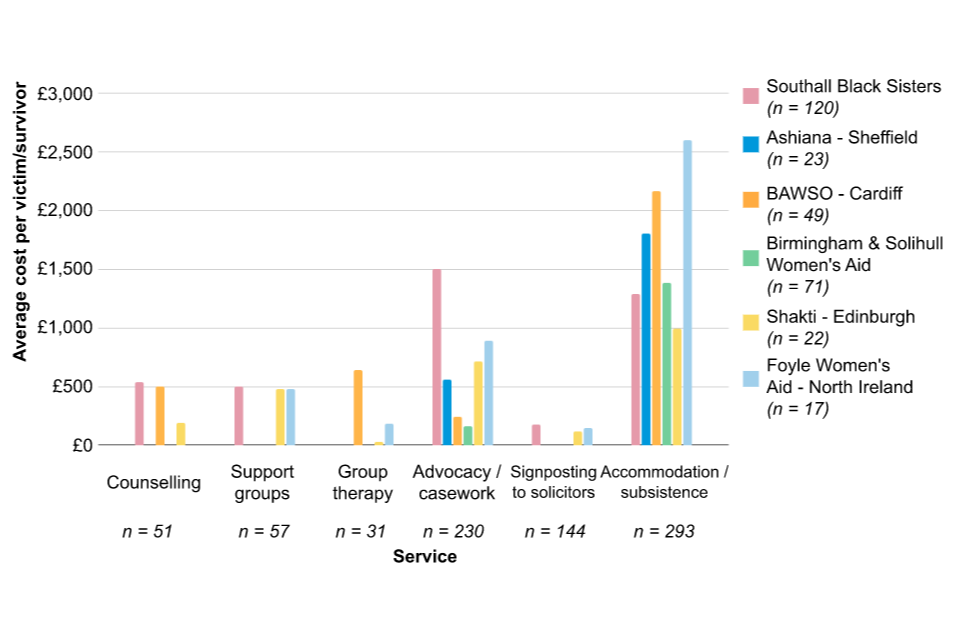
4.7 Are the delivery partners able to successfully deliver the Pilot? [RQ7]
Delivery partners faced a number of challenges in delivering the Pilot successfully. Each of the sections on specific support types touches on some of them. However, to summarise the key barriers:
Providing accommodation in the constraints of the Pilot was a challenge for providers
Finding suitable accommodation was a key barrier for delivery partners because of the amount, duration, and timeliness of the funding. Due to the amount of funding for accommodation, delivery partners were unable to afford Women’s refuges. Delivery partners had to identify and create relationships with affordable accommodation providers. This was particularly challenging in areas with high property prices or poor supply. This led to some victims/survivors experiencing inadequate accommodation with poor or unsafe living conditions. The length of funding also created complications in finding accommodation providers who worried about next steps after the funding elapsed. Finally, delivery partners flagged there were delays receiving the funding from the Home Office, which further complicated their ability to pay for and create relationships with accommodation providers.
The lack of funded legal aid was a barrier preventing delivery partners from supporting victims/survivors to access their entitlements
Delivery partners could not access funded legal aid through the Pilot, so had to apply for conditional legal aid, use internal resources, or seek pro-bono support in the absence of legal aid. However, legal advice was essential to support victims/survivors to settle their family disputes and understand their immigration choices. Legal aid was only available to some on a conditional basis (either through DDVC or ECF), but obtaining this funding required time and work on behalf of the delivery partners. Some partners felt able to support victims/survivors with the bureaucracy themselves, while others felt unprepared. In some cases, the lack of professional legal support led to errors and further delays in progressing clients’ cases. This often left delivery partners to rely on the goodwill and availability of pro-bono solicitors.
Delivery partners had to dispute local authorities over their duty to support children under Article 17
There were many instances where local authorities were unwilling to support victims/survivors and their children because of strained budgets and resources. Delivery partners had to advocate for victims/survivors and their children’s rights by navigating complex legislative systems and internal local authority politics. There were instances where delivery partners were forced to take legal actions against local authorities on the basis that the local authorities were neglecting their statutory duties. In some cases, local authorities pushed back on supporting a victim/survivor by offering to take the children in foster care - separating the family unit.
There was a lack of external and internal awareness, and understanding of the Pilot
Because the Pilot was newly launched, there were some small barriers when it came to external and internal understanding of what the Pilot was and how it worked. Externally, delivery partners emphasised how both victims/survivors and other agencies (including local authorities, the police, and other charities) were not aware that the support was available. Internally, caseworkers and Pilot managers felt that there could have been more clarity on how the funding worked and specifically on changes during the course of the year. For instance, caseworkers found out they could apply for an extension for complex cases “only by asking”. They would have appreciated more clarity on the options available from the start.
5. Pilot outcomes
In this section, we discuss the outcomes of the Pilot. We recognise that the core aim of the Pilot was to help support victims/survivors of domestic abuse escape from their abusive relationships, and to start a life beyond the perpetrator. To this end, we first focus on the effects of the Pilot on victim/survivor independence, and then their wellbeing. We finally summarise the potential effects of the Pilot on immigration outcomes, which delivery partners identified as particularly important during the logic model workshop.
5.1 What are the potential effects of the Pilot on victim/survivor independence? [RQ8]
We conceptualised independence in 2 ways to reflect the different ways in which ‘independence’ was referred to in the interviews and focus groups:
- independence from the perpetrator: when victims/survivors entered the Pilot, ‘independence’ typically was used by them in reference to escaping an abusive relationship - thus gaining independence from their partners or ex-partners
- financial independence: as the support from the Pilot progressed, some victims/survivors started to think of ‘independence’ more in terms of financial autonomy and their ability to partake in society
While the Pilot was generally successful in emancipating victims/survivors from perpetrators, enabling financial independence proved more complex. Some victims/survivors were able to achieve financial independence on exit of the Pilot through finding a job. However, the more typical experience was that victims/survivors needed to be supported by other entitlements because they faced high barriers to entering the labour market. Having support via benefits entitlements provided time for these barriers to the labour market to be overcome but did not constitute financial independence on their own. We provide more clarity on these points below.
The Pilot supported victims/survivors to gain independence from the perpetrator
Victims/survivors became independent from abusive relationships as a result of the Pilot. Many described the support received through the Pilot as a lifeline that enabled them to finally leave the perpetrators. In the interviews, many victims/survivors stressed how liberated they felt from the perpetrator, and how they never wanted to have contact with them again. However, this seemed to be more complicated with those who had children with their partners or ex-partners, as the parenthood of their children forms a link with the perpetrator even after they have stopped contact with them.
Victims/survivors were determined to rebuild their life independently of the perpetrator. Many participants mentioned how the Pilot helped victims/survivors improve their understanding of domestic abuse. Caseworkers felt - and victims/survivors said - they had to learn how to process their experiences, stop blaming themselves for their circumstances, and learn how they could reduce their risk of future abuse, for example, by learning how to spot abusive patterns. As put by one of the victims/survivors herself:
“I’m not going to be a victim again for anything. I can go through this, and I deserve better. Yes, I can go through these things. They’re not going to be for whole life. I feel yes, I can do something. This is not going to be forever. I can move on. I still have so many things to do and I can do.”
[Victim/survivor]
We asked caseworkers whether they had experienced victims/survivors returning to abusive partners or ex-partners after the Pilot. Caseworkers felt it was very rare for those in the Pilot to return because beneficiaries of the Pilot were often in such “desperate circumstances” and were unlikely to look back after having been given a route out of abusive relationships. Our analysis of the monitoring data corroborated this sentiment: 5% (n = 14) of victims/survivors either returned to their family home or reconciled with the perpetrator. However, caseworkers did emphasise that those with children were more likely to still have contact with their partner or ex-partners which could lead to relapses in the relationship. As put by one of the caseworkers:
“Only a few women return to their partners, when the support really fails them. But in general no, they do not return or leave the programme. They are so grateful for this chance of escaping their awful circumstances, they would not think about going back for one second. The only cases, yeah, are women with children. They sometimes still have a relationship with their husband or boyfriend if it’s the father. This can sometimes cause them to return.”
[Caseworker]
Around half of victims/survivors had access to public funding by the end of their Pilot support
From the monitoring data, we were able to determine the proportion of victims/survivors who were able to access funding - or had made progress towards it - on exit of the Pilot. Figure 12 presents the proportion of outcomes of victims/survivors on exit of the Pilot. We found that 49% (n = 148) had access to funding on exit of the Pilot, most commonly by being granted DDVC. It is also apparent that, for other victims/survivors, there was progress towards access to funding (22%, n = 67), typically in the form of applications for asylum. For some victims/survivors however, there was no progress towards financial independence (6%, n = 19) or the outcome was simply not known (15%, n = 44).
Figure 12: Outcomes of the Pilot by victim/survivor[footnote 16]
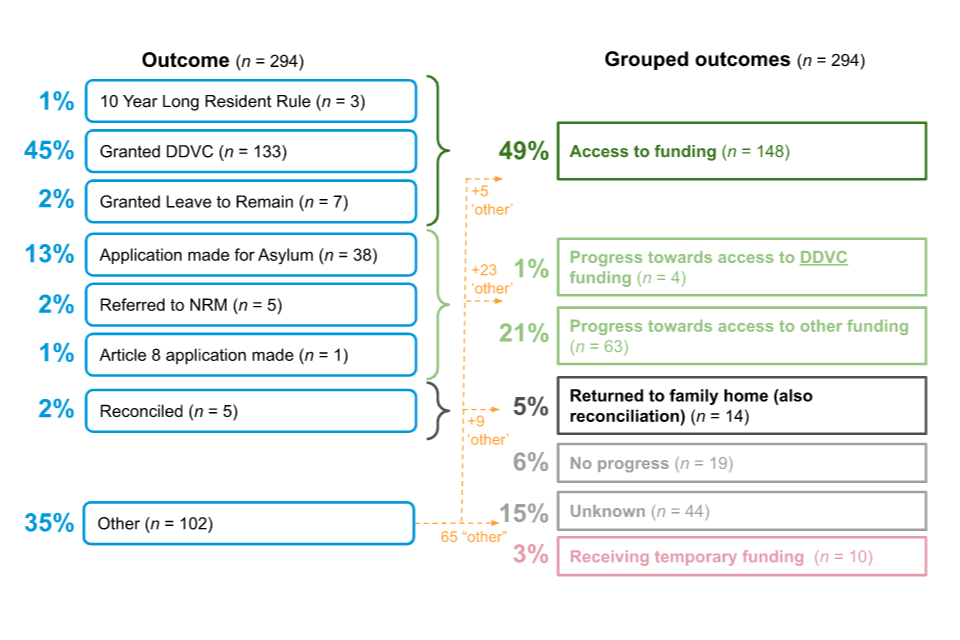
Victims/survivors were more likely to have access to funding by the end of their Pilot support if they were eligible for DDVC
We heard from victims/survivors who were eligible for DDVC that they generally received swift support from caseworkers to apply and received an outcome within the 12-week timeframe of the Pilot. Victims/survivors we spoke to felt that the process was straightforward given the support of their caseworker. In these cases, victims/survivors were granted temporary leave to remain and could subsequently apply for indefinite leave to remain. As a result of their indefinite leave to remain, victims/survivors received access to public funds, which meant being able to claim Universal Credit, apply for council housing, or to be hosted in dedicated women’s refuges, aiding access to wrap-around service. This also meant that some could start working, increasing their financial independence.
In contrast, victims/survivors ineligible for DDVC tended to face longer and more complex journeys to access funding and understand their options. For these victims/survivors there was a lack of clarity whether and how they could remain in the UK. While the delivery partners tried their best to support victims/survivors in evaluating their options, these challenges were exacerbated when perpetrators withheld documents, dedicated legal counsel was unavailable, or when local authorities where uncooperative. As discussed above, 13% (n = 38) of victims/survivors leaving the Pilot had applications made for asylum due to these challenges.
This complexity in accessing funding is reflected in the length of support needed and the likelihood of accessing funding at all, by funding outcome. Figure 13 presents the typical length of time services were provided for 2 cohorts: victims/survivors who were granted DDVC on exit of the Pilot, and those who were not. For those granted DDVC, the majority (80%, n = 106) were supported by the Pilot for 6 weeks or less. Very few (6%, n = 8) were supported for over 12 weeks but eventually had DDVC granted. This suggests that the DDVC process, when successful, was generally fast.
In contrast, for those not eligible for the DDVC, nearly half (47%, n = 80) were supported for the full 12 weeks or longer. Importantly, as discussed above, these tended to be cases where funding was not immediately available after the support from the Pilot ended.
Figure 13: Length of services by outcome (granted DDVC or not granted DDVC)
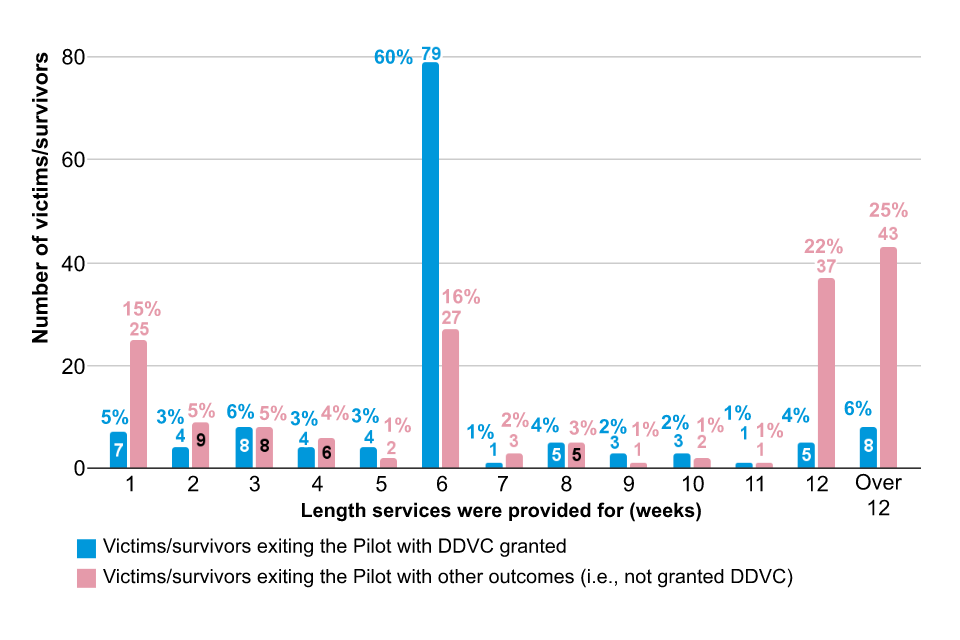
Although many victims/survivors had access to funding (or applications made) on exit of the Pilot, they were unlikely to be financially independent after exiting the Pilot
Access to funds after the Pilot provided security and certainty for victims/survivors, which is an important step towards financial independence. For others, a lack of funding after the Pilot meant that victims/survivors had to be supported through another route. In general, with some exceptions, victims/survivors were not in a position to support themselves financially at the end of the Pilot. There were 3 main outcomes for financial dependence:
- Victims/survivors were able to access benefit entitlements. These victims/survivors were eligible for and, able to transition promptly to, some public funds (such as DDVC or Universal Credit) after the Pilot. For victims/survivors, this outcome was the most preferable and was a step towards financial independence. Some victims/survivors in this position were exempt from seeking work due to poor mental health resulting from abuse. Others, however, were volunteering to support other victims/survivors, looking for education and training opportunities, or paid work to support themselves financially.
- Victims/survivors were supported by the asylum system. These victims/survivors were in the process of seeking asylum and, accordingly, were living in asylum accommodation. Victims/survivors seeking asylum were provided with accommodation and 3 meals a day. Because of their unresolved asylum status, they were unable to seek work to support themselves financially and received £8 per week. 13% (n = 38) of victims/survivors leaving the Pilot had applications made for asylum.
- Victims/survivors remained dependent on their delivery partner organisation. These victims/survivors no longer received support through the Pilot but were still dependent on financial or in-kind support (such as, foodbanks) provided by their delivery partner organisation. This was sometimes due to delays in receiving Universal Credit or DDVC or because their immigration status prevented them from working in the UK.
Despite the support received through the Pilot, victims/survivors faced high barriers in achieving financial independence
Financial independence was difficult to achieve for many because of high barriers that victims/survivors faced in entering the labour market. Barriers expressed in the interviews can be grouped in 2 categories: legal and personal capability barriers.
Legal barriers to financial independence
Legal barriers to financial independence included victims/survivors having uncertain immigration status, not having the right to work in the UK, or missing documents or qualifications which prevented them from progressing their career. Many victims/survivors were keen to gain further independence by working and managing their own rent and finances; however, they faced high legal barriers to doing so.
Case study - Unsettled immigration status prevents victim/survivor from achieving financial independence
Ju* entered the UK from China on a fiancé visa. She is a graphic designer and has completed several digital design courses in the UK. After leaving the perpetrator, Ju entered the Pilot and slowly started to rebuild her life and her independence. However, despite wanting to work and support herself financially, her uncertain visa status prevents her from working in the UK. In order to find work and become financially independent, Ju needs to find a company willing to sponsor her. Although she found a company willing to employ her, they were not willing to go through the process of applying for a sponsorship licence. Because of this, Ju is still financially dependent on accommodation provision and subsistence payments. “They just told me - asking, do I have financial issues? I explained, yes, because I’m not working. I’m not allowed to work because of the visa. If I work, I could switch to a certain type of visa… but this type of visa requires you sometimes to actually find a job first, switch, also not any job but it has to be a sponsored job… I tried to find a solution; there is a company… that was always interested in me. I had contacted them, and I think they were interested in hiring me, but they are not interested in getting a sponsorship licence… which is fair enough because it’s a lot of things to deal with, a lot of money to pay for companies to get a sponsorship licence.”
*Case studies have been anonymised to protect the identities of victims/survivors.
Other victims/survivors faced barriers because the perpetrators had destroyed or withheld documentation. These victims/survivors reported that the perpetrator had destroyed their educational qualifications, which had made them less employable.
Case study - Destroyed documents create barriers for victim/survivor who wants to become a nurse
Jaqueline* is originally from Rwanda and entered the UK on a Spouse Visa. Her husband started violently abusing her. Eventually she had to call the police, who helped her find emergency accommodation through the Pilot. But, as a form of retaliation and control, the perpetrator kept her documents. He was eventually forced by the police to handover proof of the Spouse Visa and her passport, but he had burnt other crucial documents like Jaqueline’s high school diploma, bachelor’s degree, and MBA. Jaqueline feels the Pilot has done wonders for her independence, and she now has indefinite leave to remain. She feels ready to move out of the accommodation provided into council housing and she feels she is ready to take control of her “adult duties” like “paying bills and managing her finances”. Jaqueline hopes she can qualify as a nurse and work for the NHS, but this has been difficult since she has no proof of completing university. Fortunately, the nursing college has decided to admit her on the condition that she passes an English and numeracy test, which she is currently studying for. This case study shows how despite big efforts by victims/survivors to regain their independence, perpetrators can still exert control.
*Case studies have been anonymised to protect the identities of victims/survivors.
Capability barriers to financial independence
Other victims/survivors faced barriers to financial independence which related to their own personal capability. Several victims/survivors had been abused from a very early age, and or had suffered extreme trauma from their experiences. For these reasons they felt completely unable to work due to mental health conditions which made social interactions very difficult. In other circumstances, victims/survivors and their caseworkers emphasised how they had been kept isolated from British society by the perpetrator and thus had severe linguistic and literacy barriers which made it extremely difficult for them to secure employment and navigate the bureaucratic complexities of life alone.
5.2 What are the potential effects of the Pilot on victims’/survivors’ wellbeing? [RQ9]
Victims/survivors felt that the Pilot had very positive effects on their wellbeing specifically by making them feel “safe” and supporting them to regain their “confidence”. This was not just due to one specific element of the Pilot but was an outcome that resulted from a combination of their lived environment, social networks, and access to rights and entitlements. Nonetheless, those with unresolved immigration circumstances tended to feel anxious about their prospects beyond the end of the Pilot.
Victims/survivors felt their mental health and wellbeing had improved throughout the Pilot
Across the interviews, victims/survivors described feeling safer and more confident as a result of the support provided through the Pilot. When asked about role of the Pilot in improving their wellbeing, victims/survivors gave positive responses:
“I think I’m smiling a bit more and crying less.”
[Victim/survivor]
“I generally found myself and found my confidence. At the beginning, I think I was very feared for everything, for my kid, for myself… for the future, and now, I know I need to be more brave, yes, and just more independent.”
[Victim/survivor]
The support received through the Pilot was generally valued by victims/survivors and contributed to their wellbeing. For example, participants were supportive of being housed in a safe women-only environment, where they could form networks with peers. Others mentioned how they valued the agency that had arisen from the receipt of cash payments, which enabled them to cook for themselves, and others spoke positively of the ongoing emotional support offered by caseworkers.
Some victims/survivors developed the confidence to take on volunteer work, supporting other victims/survivors of domestic abuse, which they felt positively impacted their mental health and wellbeing:
“I was scared going outside or everything, because of everything that happened to me, but now I feel a little bit safer to do that. I start doing some voluntary work, which is helpful.”
[Victim/survivor]
“I’m also works as, got my part-time job and works as a volunteer to help the other females in dangers.”
[Victim/survivor]
Victims/survivors developed peer networks through the Pilot
The peer networks which victims/survivors developed during the Pilot provided informal support which played a key role in improving victims’/survivors’ wellbeing. Victims/survivors described forming tight friendships or groups with others they had met in their accommodation, through activities such as cooking together. Through these friendships, they could provide guidance and support to each other. Other victims/survivors, who spoke the same language and/or shared the same religious beliefs, were able to build a sense of normalcy and community together. Many of these relationships were long-lasting and some victims/survivors moved in with their peers when they had access to council housing. This seemed particularly common for victims/survivors in shared accommodation:
“Actually, when you arrive in the refuge, we become like a family, a very nice, and we support each other. Everyone have their ups and down. Everyone have our story so we just try to feel, as in when a new girl come, we just try to welcome her, to see her at home so that she can try to forget what happened for her.”
[Victim/survivor]
Some victims/survivors still experienced stress and anxiety over about their future because of a lack of certainty over their immigration status and entitlements
A number of victims/survivors experienced anxiety caused by a lack of certainty about what would happen to them after the support provided by the Pilot finished. This was particularly the case for victims/survivors whose immigration status was unresolved when the support provided by Pilot:
“Although she has all these things and all this lots of support, … she is still under pressure for her circumstances because it is a kind of unknown situation what’s going to happen to her. That still makes her have an effect on her anxiety, so still got anxiety and worrying about what’s going [to] happen.”
[Victim/survivor]
Victims/survivors who were waiting for their immigration status to be resolved, or to be able to access benefit entitlements, experienced long periods of uncertainty. During these periods, they felt stressed or anxious, and unable to do activities that supported their mental health and wellbeing. For example, one victim/survivor described being advised against volunteering or doing other activities while waiting for a decision on her immigration status from the Home Office:
“Some solicitor and the other people said unless you didn’t get the final result from the Home Office, you’re better to not go anywhere, don’t join [a volunteering organisation]. She finds that trying to stay home all the time and do nothing, and she would appreciate it if she’s able to join, make herself busy and have to learn something, and use this time which is kind of wasting time at the moment until she gets the final answer for her remaining, you know, the UK.”
[Victim/survivor]
5.3 What are the potential effects of the Pilot on immigration outcomes? [RQ10]
The primary aim of the Pilot was to provide a support net for victims/survivors of domestic abuse who do not have access to public funds, and are unable to escape abusive relationships due to a lack of access to safe accommodation.
However, in the logic model workshop, delivery partners also emphasised immigration outcomes as an important component of the Pilot. Specifically, that victims/survivors “understand their rights and entitlements” and “regularise their status as appropriate”. This section accordingly explores the range of immigration outcomes that victims/survivors entered and exited the Pilot with.
A greater proportion of victims/survivors had applications in progress on exit of the Pilot than those entering the Pilot
Figure 14 illustrates that victims/survivors both entered and exited the Pilot with a wide range of immigration statuses. We found that, while fewer victims/survivors exited the Pilot with an immigration status of ‘Valid Leave’ than entered with it (57% [n = 173] on entry versus 42% [n = 128] on exit), more victims/survivors had applications in progress on exit of the Pilot (9% [n = 27] on entry versus 39% [n = 117] on exit).
Figure 14: Immigration status on entry and exit of the Pilot (n = 302)
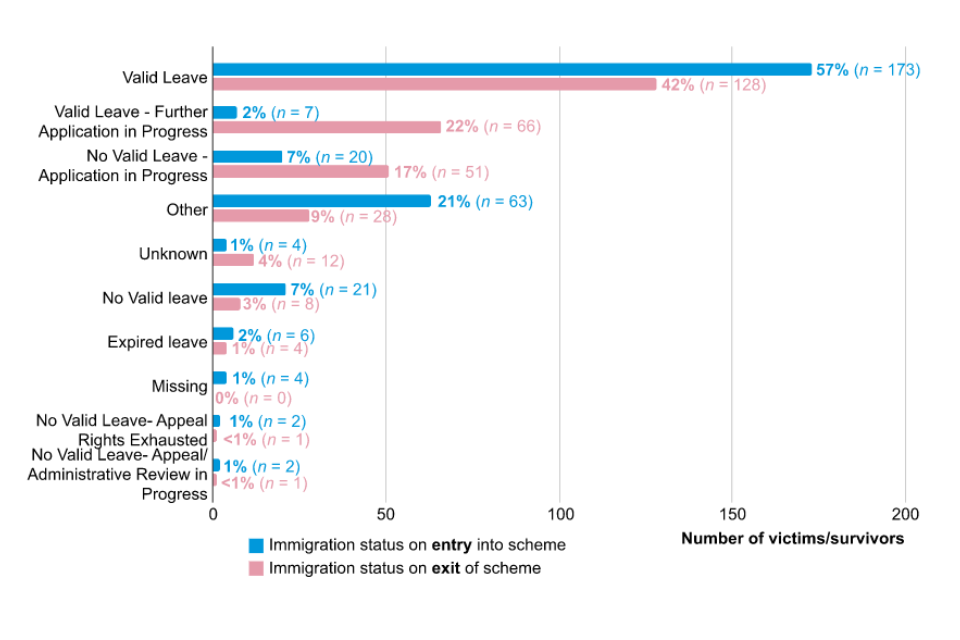
Immigration outcomes at the end of support
- indefinite leave to remain through DDVC: victims/survivors obtained a temporary visa for a 3-month period while they secured indefinite leave to remain with the support of an immigration solicitor; they would obtain this status on the basis that they are on a qualifying Spouse Visa and victim/survivor of domestic abuse
- supported by social services: victims/survivors with children started receiving support from local authorities under Section 17 of the Children’s Act and were granted the right to remain with the support of a community care solicitor; the Pilot does not usually see how these immigration cases are resolved as they tend to support these clients only for a brief period of time
- asylum application: victims/survivors started receiving support from the Home Office under Section 98 of the Immigration Asylum Act of 1991; their refugee status will be reassessed after 5 years to see whether they still face potential harm of returning to their home country. This outcome is pursued for those who can prove they are at risk of harm in their home country, for example, LGBT+ people, or those at risk of honour crime from their family or in-laws
- right to remain through 20 years rule: some victims/survivors can obtain a 10-year permit to remain in the UK if they can prove they lived in the UK for more than 20 years
- right to remain through Right to Family Private Life Application: in some rare cases victims/survivors are granted Article 8 of the European Convention of Human Rights which can grant migrants the right to stay if they prove they have family and private life in the UK; victims/survivors are usually supported for a limited period through SMV and then settle into accommodation with family or friends
- work-based temporary visa: some victims/survivors apply for a temporary work-based visa; for example, they may apply for a Start-up visa or an Innovator Visa, by demonstrating to the Home Office that they have a viable and innovative plan to set-up a business; however, the vulnerabilities and specific circumstances faced by many of the victims/survivors (for example, low income, poor mental health and language barriers) can make this a particularly challenging route to pursue
- not granted leave to remain: some victims/survivors are not granted leave to remain in the UK and return to their home country
Victims/survivors entered the Pilot with limited knowledge of their immigration choices, sometimes as a direct result of the abuse they faced
The Pilot played a key role in improving victims’/survivors’ understanding of the immigration system, which was generally very low when they entered the Pilot. Several victims/survivors were brought to or entered the UK without an understanding of how the immigration system works, and many entered the Pilot still with limited knowledge of the immigration system or their immigration choices. Poor literacy and English skills were one of the reasons for this, as they posed a significant barrier to victims/survivors engaging with the information available.
However, there were also multiple examples in which victims’/survivors’ poor understanding of the immigration system was directly related to abuse. Firstly, some victims/survivors came or were brought to the UK under false pretences or imperfect information. For example, some victims/survivors came to the UK as fiancées thinking they will become brides and are then abused and exploited while their visa expires. Others were brought into the UK under the false promise of stable work but are then abused and exploited. In other cases, victims/survivors were brought in on a work visa without any deception. However, they are never supported to settle their immigration status and their poor understanding of the system means that they may not be aware that they have no further right to remain.
Secondly, perpetuating a lack of information about visa and immigration status was used by some perpetrators as a way of exerting control. For example, perpetrators exploited the fact that victims/survivors were in the UK illegally to threaten and control them. Victims/survivors reported that the perpetrators threatened them by saying that they would call the police or the Home Office to have them jailed or deported. Caseworkers said that this created trauma through fear of government institutions, which further hindered their understanding of their immigration options.
“Because the perpetrators have threatened them saying ‘I will call the Home Office on you!’ when they come into the programme and we say to them that we need to file an application with the Home Office so many are terrified and they beg me not to. Some start crying. They have no idea about their rights or options because of the perpetrators - this is also on top of the fact many have low literacy or don’t speak English.”
[Caseworker]
Case study - Victims/survivors is brought to the UK by a firm but was not supported to settle her immigration status
Tianna* is originally from Jamaica. When she was a teenager, she was scouted by a prominent British football club looking for promising female talent. The club’s talent scouts arranged for her to come into the UK on a work visa promising her a bright future. During her career as a football player, Tianna experienced a lot of racism and neglect from those who promised to support her. The club never paid her as much as her white team-mates, and never took her immigration status seriously. When her career started drawing to an end, Tianna found herself without a permit to remain in the UK, despite having lived in the country for over 2 decades. She was left to rely on her boyfriend for support, who was abusing her physically and psychologically. When Tianna felt she could not take it anymore and left she became homeless, without any access to public funds or a support network. She slept rough for some time until she found support through a homelessness charity, who put her in contact with one of the delivery partners. The delivery partners are now trying to apply for her Right to Remain under the 20-year rule, but it has been proven difficult to trace all her documents since the club who brought her to the UK failed to keep accurate records of her permits throughout the years.
*Case studies have been anonymised to protect the identities of victims/survivors.
6. Discussion
In this section, we summarise the findings of our evaluation of the Pilot and synthesise these into 2 broad groups: what has worked well, and what has worked less well.
To assess what worked ‘well’, we considered whether different elements of the Pilot contributed to its overall aim: to provide a support net for victims/survivors of domestic abuse with NRPF, specifically by providing safe accommodation so that they can leave the abusive relationship. We also considered where the experience and outcomes of support seem to vary based on the characteristics of the victim/survivor.
6.1 What has worked well?
Our findings suggest that there were 4 clear areas in which the Pilot worked well:
The Pilot provided emergency relief to victims/survivors that were in need
The Pilot provided accommodation to at least 302 victims/survivors with NRPF (more were receiving support at the end of the evaluation). Without the Pilot, these victims/survivors may not have found a safe place to stay. Accommodation was one of the most valued parts of the Pilot by victims/survivors, who said that it allowed them to leave the abusive relationship at a moment of crisis, preventing further physical or psychological harm. In cases of utmost urgency, we heard that caseworkers were able to provide emergency accommodation (such as a hotel) to victims/survivors on the day they sought help, which was also funded by the Pilot. Overall, the Pilot was a lifeline at a time of extreme vulnerability for victims/survivors.
The Pilot bridged the gap between victims/survivors leaving the abusive relationship and accessing other funding sources
Regardless of the source of funding - from Universal Credit to DDVC - it takes time to apply and receive the funds, and often requires the assistance of a caseworker. The Pilot helped victims/survivors by providing funding for services while other funding was secured. For example, nearly half (45%, n = 132) of victims/survivors were granted DDVC by the time they left the Pilot. The majority of these had support for 6 weeks (60%, n = 79), although roughly equal numbers were supported for a shorter (20%, n = 27) or longer period (20%, n = 26). We also found more victims/survivors had applications in progress on exit of the Pilot (9% [n = 27] on entry versus 39% [n = 117] on exit). This suggests that the Pilot helped provide support for victims/survivors at a time when other funding was not there, bridging this gap. The Pilot helped by providing services with a total cost of £729k, an average of £2,455 per victim/survivor, which otherwise may not have been funded.
The dedicated support provided by caseworkers was particularly valued by victims/survivors that were supported through the Pilot
One of the most valued aspects of the Pilot was having a dedicated caseworker who accompanied beneficiaries on their journey. Having a specific, dedicated caseworker meant that victims/survivors had a frequent contact, who we heard was able to provide ongoing emotional support - which was particularly important given that victims/survivors had left an abusive relationship. Caseworkers were also able to help provide legal and bureaucratic support, helping beneficiaries understand their immigration options and accessing their entitlement. For example, caseworkers helped victims/survivors apply for DDVC or asylum, as well as a range of other administrative tasks, such as submitting biometrics or opening a bank account. Dedicated support facilitated ongoing support for a system that is not always easy to understand - especially if English is not your first language - to victims/survivors who were at a time of great need.
The Pilot provided substantial benefits to the mental wellbeing of victims/survivors
In addition to providing victims/survivors with a safe place after escaping an abusive relationship, the Pilot also helped improve the mental wellbeing of victims/survivors. At the start of the journey of victims/survivors, the Pilot helped with the basic needs of victims/survivors, such as providing a safe place to stay, as well as ending potentially physical or psychological harm from the perpetrator. Dedicated caseworkers were also able to provide emotional support to victims/survivors. As their journey continued, services such as group therapy helped victims/survivors build peer networks with others who had shared experiences, as did sharing accommodation with other victims/survivors. Access to mental health care was also available for those with conditions, which was facilitated through the Pilot. The Pilot also helped reduce stress and anxiety by helping victims/survivors understand their immigration options and entitlements.
6.2 What has worked less well?
Despite the Pilot performing well in some respects, we also identified 4 areas in which it did not fully meet the needs of victims/survivors:
Subsistence payments were often not sufficient to cover basic expenses, and delivery partners universally relied on relationships with local charities to fill the gap
We found that the funding for subsistence and accommodation was not always sufficient for the needs of victims/survivors. For example, subsistence payments were not always sufficient to cover basic expenses, such as food, toiletries, or other basic necessities like essential transport. This was the case even after payments had increased to £50 and meant that delivery partners had to rely on relationships with local charities to fill the gaps. This issue was exacerbated by rising living costs during October to December 2021.
Providing suitable accommodation within the constraints of the Pilot was a real challenge for providers
Finding suitable accommodation was a challenge for providers due to the amount, duration, and timeliness of the funding. The amount meant that delivery partners were unable to afford Women’s refuges, and thus had to find accommodation elsewhere, such as supported accommodation or B&Bs. These were not always appropriate for victims/survivors of domestic abuse as they included other guests who were men or struggling with substance abuse. Overall, the insufficient funding meant that some victims/survivors were provided with poor or unsafe living conditions.
Even where delivery partners were able to place victims/survivors in suitable accommodation, the structure of repayment often created challenges for the delivery partner themselves. Applications for reimbursement could only be made to the Home Office on a quarterly basis, and payments could take upwards of a month to come through. Delivery partners who took on victims/survivors at the start of a quarter would therefore need to meet the costs of the accommodation for 4 months or more before receiving payment.
Many victims/survivors have complex legal situations which require more than 12 weeks to resolve
We heard that some of the victims/survivors had complex circumstances which made it hard for them to resolve their status within the duration of the Pilot. In some cases, this was because victims/survivors were pursuing processes, such as asylum or residency applications, that regularly take more than 12 weeks. However, it also included cases where documents had been destroyed or withheld by perpetrators, delaying the ability to apply for any support, or where local social services were unwilling to provide the support that victims/survivors were entitled to.
In these cases, resolving the complex legal situation often took longer than 12 weeks. This is reflected in the monitoring data, where the most common service length was at or above 12 weeks for those who were not granted DDVC (47%, n = 80). Victims/survivors reported this causing anxiety, as they did not know how they would be supported once the Pilot period ended. In practice, delivery partners would sometimes find ways of supporting victims/survivors after this point, but not necessarily at the same level. Delivery partners did, however, report an improvement after January 2022 when they were granted more flexibility in how the funding could be used.
In some cases, victims/survivors would be transferred to the asylum system while their application was pending. However, we heard that this route had ended up with severe negative consequences for some victims/survivors as asylum accommodation (and the route more broadly) does not have the support required for a victim/survivor of domestic abuse.
The risk of support ending also impacted the provision of accommodation. Some accommodation providers were reluctant to take on victims/survivors being supported through the Pilot, because they worried that they would be responsible for them after the funding ended if the victim/survivor did not have access to any other form of support.
Delivery partners do not always have the resources or expertise to support highly complex cases
The complexity of some of the cases receiving support from the Pilot also placed additional burdens on delivery partners. They reported that the legal complexity of many of the cases meant that providing support for victims/survivors coming through the Pilot was often more challenging than for other victims/survivors they supported. These challenges could be combined with other vulnerabilities, including mental health conditions, that delivery partners also felt they needed more support to address. In some cases, delivery partners did not feel they had the expertise to support victims/survivors as effectively as possible.
The diversity in languages of victims/survivors added additional challenges to supporting them
We found that the range of languages found amongst victims/survivors created specific challenges when implementing the Pilot. Delivery partners were able to offer interpretation services in cases where there was no common language, but these were only available for their services. For services external to the delivery partners, such as accommodation services, interpretation services were less common, which left some victims/survivors feeling isolated. This was a particular issue for legal support, where complex concepts were challenging to communicate without interpretation services.
Regional variation of available support services meant there were regional differences in terms of the quantity and quality of support provided
We found that differences in the types and quality of support provided was driven partially by regional differences in the availability of local services. This was apparent for the following services:
Accommodation: The accommodation provided varied due to different local costs, as well as supply. For instance, due to the limited budget for accommodation, delivery partners used their networks to source alternative accommodation. For those in more rural areas, the lower density of accommodation meant that victims/survivors sometimes had to move further away from their local area to access accommodation. In some cases, victims/survivors were moved to a different city because they did not feel safe staying closer to home.
Legal support: All delivery partners signposted to lawyers, but access to pro-bono support varied between regions. Some delivery partners had strong relationships with pro-bono lawyers, which facilitated better signposting. For other delivery partners, pro-bono lawyers were much harder to come by: we heard from one delivery partner that their one pro-bono lawyer retired and there was no replacement, hampering support. As finding pro-bono aid was so difficult, delivery partners had to do a lot of unfunded work sourcing aid or applying for legal aid. We also heard that one delivery partner had trained caseworks to be better equipped to support with the legal paperwork due to issues finding pro-bono lawyers. In other cases, caseworkers did not have the necessary training to address the legal needs of victims/survivors, which led to delays and errors in legal paperwork.
Wellbeing support: 4 out of 6 delivery partners provided individual counselling and group therapy and support groups were offered by 5 out of 6 providers. The experiences of support differed by region, however, as more rural areas meant that victims/survivors had to travel longer distances, or had weak internet connectivity, making remote access challenging.
The Pilot bridged gaps in local authority provision in regions where local authorities were unable to fulfil their duties
Local authorities have a duty to support victims/survivors with children under Article 17 of the Children Act 1989. However, delivery partners commented that local authorities were under-resourced, resulting in them being unable to recognise their duties under Article 17. This manifested in different ways: in some cases, local authorities only offered support to children through foster care, and not to mothers. This resulted in delivery partners having to spend time arguing the case that victims/survivors should be supported under Article 17, and in some instances, taking legal action against the local authority. The Pilot was not intended to support victims/survivors with children due to the requirement of Article 17, but we found that 25% (n = 74) of victims/survivors had at least one child, indicating that the Pilot was covering gaps in local authority provision.
Awareness of the Pilot, amongst both potential recipients and other agencies and local services, was a barrier to effective provision
We heard from several delivery partners that the newness of the Pilot meant that awareness was a key challenge, which might have affected uptake of the Pilot and its ability to reach victims/survivors in need. Low awareness amongst victims/survivors is one potential barrier to uptake; they may not know that support was available given their funding status, and therefore not seek support. However, the bigger emphasis from delivery partners was on awareness amongst other organisations. For example, community organisations, social services, the police and GPs could all potentially refer victims/survivors to the Pilot (either directly, or by providing victims/survivors with information about the Pilot). However, they were not always aware of the Pilot and delivery partners reported doing extensive awareness raising work to address this.
Low awareness of the Pilot amongst other organisations could also affect delivery as well as uptake. Delivery partners reported having difficulty accessing support services, such as accommodation, due to agencies’ preconceptions that there was no funding available to support victims/survivors with NRPF. Delivery partners reported that because of these preconceptions, other agencies were concerned that providing services to victims/survivors with NRPF would be costly to them.
The awareness raising activities conducted by delivery partners is a possible explanation for the increase in the number of victims/survivors supported by the Pilot over the course of the 12 months.
Victims/survivors were typically unaware that the funding originated from the Pilot and were unaware of their entitlements
Victims/survivors typically entered the Pilot with little understanding of their entitlements, and their involvement with the Pilot did result in more victims/survivors understanding their entitlements. This was generally facilitated by the caseworkers, who were able to share their knowledge with victims/survivors. However, victims/survivors did not realise that the Pilot was the source of the funding for their accommodation and tended to think that the delivery partners were providing the funding themselves. Moreover, victims/survivors also did not realise that some services were funded by other sources, such as support groups. This overall suggests that the Pilot did help to increase understanding of what victims/survivors could receive, but often not to the extent that victims/survivors understood where their entitlements came from. This, in turn, meant that the cessation of funding from the Pilot caused confusion and upset to some victims/survivors.
7. Conclusion
The aims of the Pilot were to provide a support net for victims/survivors of domestic abuse who do not have access to public funds and are unable to escape abusive relationships due to a lack of access to safe accommodation.
In many and important ways, the Pilot met these aims. Accommodation and/or subsistence were provided to all the victims/survivors that received support from the Pilot, which helps to provide a safe place for victims/survivors to go to at a time of great need. We heard of many cases where this has helped to bridge the gap while victims/survivors get access to other entitlements, for example, through DDVC or where local authorities are slower to respond to their Section 17 obligations for victims/survivors with children. This support removes the barrier that could have prevented them from escaping an abusive relationship, and the data suggest that a very small minority return to the perpetrator.
The Pilot also went beyond these aims in some respects. Most notably, it provided victims/survivors with social and emotional support through a combination of caseworker support; counselling, individual and group therapy; activities organised by delivery partners; and the strong support networks that some victims/survivors build with other victims/survivors being supported at the same time. It also helped victims/survivors to understand their legal entitlements and helped connect them to legal support. This can help victims/survivors with legal challenges relating to abuse, custody of children, or specific cases such as a history of trafficking, as well as applications for residency and asylum.
However, there were clear limitations to the support. Firstly, the Pilot provision itself did not always meet the need for “safe accommodation”. Refuges could almost never be covered within the accommodation budget, meaning that some victims/survivors were housed in a patchwork of other provision which might be unclean, unsafe, or unreliable (with some cases of victims/survivors being asked to leave B&Bs at the weekend). Secondly, the subsistence payments provided to victims/survivors did not always cover their basic needs. As well as food, victims/survivors can need clothing, toiletries, and transport to appointments or to stay in touch with their communities and support networks. Subsistence payments could not always cover these costs, and delivery partners were reliant on in-kind donations from charities to help victims/survivors make ends meet. Thirdly, there is an unresolved question on the outcomes of victims/survivors who do not have a quick pathway to funding, for example through DDVC. Whilst the Pilot gave delivery partners some flexibility to extend support if needed from January 2022, it was often unclear what the long-term path is for victims/survivors, and this caused additional anxiety for victims/survivors during the Pilot as well as leading to a lack of support once the Pilot ended.
There were also challenges to implementing the Pilot. The services provided often depend on local partnerships, so delivery partners are often constrained by what is available, particularly in relation to accommodation and pro-bono legal support. The administration of the Pilot also placed both time and financial burdens on delivery partners. In particular, there were sometimes several months between when a delivery partner started supporting a victim/survivor and when they were reimbursed by the Pilot. This may be a barrier to smaller organisations providing support if the Pilot were to be extended.
Finally, this evaluation only covers the victims/survivors who received support from the Pilot. What we are not aware of is individuals that did not receive support, including the victims/survivors who have not yet escaped the perpetrator - or have not made the difficult decision to escape due to other barriers. Thus, while we can say (with the above limitations) that the Pilot achieved its aims for those who received support from it, our evaluation cannot make a conclusive remark over whether it helped more victims/survivors escape abusive relationships.
Overall, the Pilot appears to be providing a valuable support net for victims/survivors and reducing the barriers to them escaping an abusive relationship. However, there are aspects of the Pilot that could be improved to better support victims/survivors and reduce the challenges of delivery for providers. In our role as evaluators, policy recommendations sit outside of the scope of this report. However, we hope that the insights gained from this research can help to refine the Pilot if the support is to be expanded.
8. Annex
8.1 Logic model
See Annex 8.1 - SMV Programme Logic Model as captured by service providers.
8.2 Full list of research questions and sub-questions
| RQ | Overall question | Sub-question | Data source |
|---|---|---|---|
| Implementation | |||
| 1 | How many victims/survivors are helped by the Pilot? | ||
| How many victims/survivors sought help? | Monitoring data | ||
| How many victims/survivors were turned away? | Monitoring data | ||
| 2 | What is the profile of victims/survivors who seek support? | ||
| What is the breakdown of victims/survivors by each demographic? | Monitoring data | ||
| How do victim profiles align with the logic model, particularly in terms of gender and immigration status? | Monitoring data | ||
| Are certain characteristics over/under-represented relative to the UK migrant population? | Monitoring data + HO migrant statistics | ||
| 3 | What support do victims/survivors receive through the Pilot? | ||
| How do victims/survivors find out about the Pilot? | Recipient interviews + practitioner FGDs | ||
| What types of support are provided through the Pilot? | Recipient interviews + practitioner FGDs + Monitoring data | ||
| What do victim/survivor journeys through the Pilot look like? | Recipient interviews + practitioner FGDs | ||
| What are victim/survivor’s experiences of the Pilot like? | Recipient interviews | ||
| What proportion of victims/survivors signposted to solicitors have a meeting? | Provider data | ||
| What types of accommodation do victims/survivors receive through the Pilot? | Practitioner FGDs + Recipient interviews | ||
| How long are victims/survivors supported by the Pilot? | Monitoring data | ||
| How long do victims/survivors receive accommodation support from the Pilot? | Monitoring data | ||
| What proportion of victims/survivors access each of the services available? | Monitoring data | ||
| 4 | Which parts of the Pilot were the most beneficial for victims/survivors? | ||
| What proportion of victims/survivors need each of the services available? | Monitoring data | ||
| What aspects of the Pilot were most beneficial for victims/survivors? | Recipient interviews | ||
| Why did victims/survivors find these parts of the Pilot helpful? | Recipient interviews | ||
| What did victims/survivors see as the benefits of these parts of the Pilot? | Recipient interviews | ||
| 5 | What are the limitations of support through the Pilot? | ||
| Which aspects of the support were the most challenging to set up? | Practitioner FGDs | ||
| What aspects of the support provided did victims/survivors feel least benefit from? | Recipient interviews + practitioner FGDs | ||
| What factors limited the impact of this support? | Recipient interviews + practitioner FGDs | ||
| How could these aspects of support be improved? | Recipient interviews + practitioner FGDs | ||
| What is the gap between need and access for each of the services available? (number who need but did not access) | Monitoring data | ||
| What factors limit provision of services when there is a need? | Practitioner FGDs | ||
| What types of support are recipients unable to access through the Pilot? | Recipient interviews + practitioner FGDs | ||
| What support are recipients receiving from other sources? | Recipient interviews + practitioner FGDs | ||
| At which points (if at all) do victims/survivors disengage with the support? What causes victims/survivors to disengage? | Practitioner FGDs | ||
| 6 | What are the costs of providing this support? | ||
| What are the costs by support component? | Monitoring data (+ discussions with providers) | ||
| How do costs vary by provider? | Monitoring data (+ discussions with providers) | ||
| 7 | Are delivery partners able to successfully deliver the Pilot? | ||
| What are the challenges providers face in implementing the Pilot? | Practitioner FGDs | ||
| What support do providers have, and need, to deliver the Pilot effectively? | Practitioner FGDs | ||
| Outcomes | |||
| 8 | What are the potential effects of the Pilot on victim/survivor independence? | ||
| What is the range of financial situations faced by victims/survivors at the end of the support? | Recipient interviews | ||
| What forms do relationships between victims/survivors and the perpetrators take by the end of the Pilot? | Practitioner FGDs + Recipient interviews | ||
| In what ways do victims/survivors perceive the support as affecting their independence? | Recipient interviews | ||
| 9 | What are the potential effects of the Pilot on victim/survivor wellbeing? | ||
| How do victims/survivors describe their wellbeing and mental health at the end of the Pilot? | Recipient interviews | ||
| How do victims/survivors understand the impact of the Pilot on their wellbeing? | Recipient interviews | ||
| 10 | What are the potential effects of the Pilot on immigration outcomes? | ||
| What proportion of victims/survivors have regularised their status by the end of support? | Monitoring data | ||
| What is the breakdown of immigration outcomes for victims/survivors at the start and end of support? | Monitoring data | ||
| What proportion of victims/survivors change immigration status between support starting and finishing? | Monitoring data | ||
| How many victims/survivors go from each immigration status at the start of support to each status at the end of support? | Monitoring data | ||
| Is there a relationship between being signposted to a solicitor, meeting with a solicitor (if possible to collect), and changing immigration status? Does this hold when controlling for factors such as children and initial immigration status, which might predict whether victims/survivors are offered a solicitor? | Monitoring data + Provider data on solicitor uptake | ||
| What types of immigration and residency outcomes do victims/survivors have at the end of the support? | Recipient interviews + practitioner FGDs | ||
| In what ways do victims/survivors perceive the support as affecting their immigration outcomes? | Recipient interviews | ||
| How do victims/survivors understand their immigration choices? | Recipient interviews | ||
| Mediators | |||
| 11 | How do outcomes and experience of the support depend on… | ||
| Ethnicity | |||
| English proficiency | |||
| Presence/age of children | |||
| Support provider | |||
| Outcomes of immigration appeals | |||
| Type of accommodation provided (if any) |
8.3 Research ethics
The qualitative research posed a number of ethical risks, due to the intersecting vulnerabilities of victims/survivors and the potential for the content of the interviews to touch on distressing topics.
At the inception of the research, we submitted the research plan to BIT’s internal ethics approval process. Due to the research involving a highly vulnerable group, we undertook an in-depth assessment of the potential ethical risks. We documented these risks in accordance with the ethical principles set out in the guidance issued by the Government Social Research Profession, as follows:
- principle 1: sound application and conduct of social research methods and appropriate dissemination and utilisation of the findings
- principle 2: participation based on valid informed consent
- principle 3: enabling participation
- principle 4: avoidance of personal and social harm
- principle 5: non-disclosure of identity and personal information
For each principle, we set out how the research complied with each principle, and actions to mitigate any areas in which there was incompliance. Adaptations and provisions made for this research included:
Preparation for the interview
Phone calls were held with each of the delivery partners prior to the interviews to discuss the protocol. This ensured that delivery partners had enough understanding of the interview content to address any questions that interviewees may have before agreeing to participate in the interview. We also discussed with each delivery partner any additional considerations for the interview set up, including whether to conduct interviews in person, by phone or by video call (interviews were conducted in person for victims/survivors supported by SBS, but remotely for other providers where delivery partners felt that transport to an interview site risked creating a barrier to participation).
The interviewer held a brief phone call with each interviewees’ caseworker before the interview. This allowed them to provide background information and highlight any particular vulnerabilities of the interviewee.
Interview content and processes
All interviewees were given the option of having an interpreter for the interview (arranged and funded by BIT). This helped to ensure that interviewees were not excluded based on their English proficiency or native language.
To ensure that participants understood the informed consent requirements, the interpreter would verbally translate them at the start of the interview. The consent requirements were shared with the interpreter ahead of the interview to give them time to familiarise themselves with the content. It was made clear to all interviewees that they could stop the interview at any time.
None of the questions in the interview asked about victims’/survivors’ experiences prior to accessing support. This was to mitigate the risk of distressing or even re-traumatising victims/survivors by asking them to recount the abuse they had faced.
Interviews were conducted by one of 2 specialist qualitative researchers, with experience conducting interviews with vulnerable groups. Researchers followed a protocol on how to enforce good safeguarding practices and minimise distress when conducting interviews, as well as a distress protocol in case instances occurred.
Interview environment
Interviewees were given the option of having another person present for the interview, such as a friend or someone from the delivery partner.
Interviews were conducted in an all-female environment. This included female interviewers and female interpreters.
8.4 Details of survey processes and methodology
8.4.1 Survey development
The aim of the survey was to provide data on UK organisations that provided refuge services to victims/survivors with recourse to public funds and with NRPF. To develop the survey, we first reviewed the initial questions of the Women’s Aid annual survey. We then selected questions that would specifically address the following research questions:
- Who currently provides domestic abuse support and what support is currently available to victims/survivors?
- How many victims/survivors are currently supported by existing service providers for domestic abuse?
- How many victims/survivors have been turned away and why?
- What is the profile of victims/survivors who come forward?
- What is the current cost of provision to support victims/survivors?
We subsequently iterated the survey several times based on feedback from the Home Office’s research and policy teams. We also refined the survey based upon our own assessment of ease in responding, duration, and to minimise confusion given the complexity of the policy area. Additionally, we conducted user-testing of the survey with Shakti Edinburgh in October 2021 and Birmingham & Solihull Women’s Aid in September 2021. The user-testing assessed the ease of completing the survey and highlighted areas to be streamlined.
8.4.2 Data collection
We used Smart Survey, an online survey platform, to collect data. To distribute the survey, we sent email invites to organisations, asking them to participate. We used the following process to identify a list of organisations we should send the invite to:
- We used the Women’s Aid Gold Book to identify 355 organisations who provided “services that provide refuge”. We then excluded all organisations that did not have an email address (or had duplicate email addresses), resulting in a sample of 186 organisations.
- The survey link was also shared with the Women’s Resource Centre and regional leads of the NRPF Network, for distribution within their mailing lists.
- Finally, we used a “snowball” recruitment approach, where we asked respondents to provide contact information of others. We sent the survey link to those contacts who had email addresses, or sent an online form where no email address was provided. Of the 32 contacts provided by respondents, 27 participated in the survey.
8.4.3 Final sample
After data collection ended, we had received a total of 93 responses. We excluded 10 responses as they appeared to be duplicate responses[footnote 17]. This resulted in a final sample of 83 responses from a total of 75 different organisations (we received more than one response for 6 organisations). 51 of these were from the original 355 organisations identified with the Gold Book.
We cannot be certain of how representative our sample is relative to all organisations that provide refuge services in the UK, due to selection bias (such as, only a proportion participated) and using an online survey (which might exclude those without email addresses, for example).
8.5 Details of interview processes and methodology
8.5.1 Interview sampling process
Interviewees were identified through a mixture of purposive sampling and identification by delivery partners. We initially selected a sample of interviewees from the monitoring data, to ensure diversity based on a wide range of factors including the services received by the victim/survivor; their gender, country of origin, and visa / type of leave on entering the scheme; as well as factors such as their religion, sexual orientation, known disabilities and age. A list of proposed interviewees was sent to each delivery partner, who could exclude specific victims/survivors if they felt an interview posed an increased risk of stress or trauma.
However, our sampling was based on the monitoring data, which only included victims/survivors who had left the Pilot in the previous quarter. This posed an additional challenge to recruitment, as delivery partners did not always have continued contact with victims/survivors. Furthermore, some delivery partners emphasised the importance of creating a clean break when support ended and felt that recontacting victims/survivors after an extended period risked muddying this. As a result, only 2 delivery partners provided interviewees from the sample we had selected. The remainder of the interviewees were identified by delivery partners in January to March 2022 of delivery.
Intended sample
Table 12 below sets out the characteristics of the 40 victims/survivors we initially proposed for interview, drawn from July to September and October to December 2021 of the monitoring data.
Table 12: Characteristics of proposed interview sample
| Intended final sample (n = 20) | |||
|---|---|---|---|
| Sampling criteria | minimum N | Sampling invites | |
| Delivery partner | |||
| SBS | 2 | 10 | |
| Ashiana | 2 | 6 | |
| Bawso | 2 | 8 | |
| Bir’ham Women’s aid | 2 | 8 | |
| Shakiti | 2 | 4 | |
| Foyle | 2 | 4 | |
| Services accessed | |||
| Counselling | 3 | 14 | |
| Support groups | 4 | 18 | |
| Group therapy / work | 3 | 12 | |
| Advocacy / casework | 10 | 34 | |
| Signpost to solicitors | 10 | 35 | |
| Accommodation / subsistence | 10 | 35 | |
| Other | no quota | 2 | |
| Gender | |||
| Women | no quota | 40 | |
| Men | Max 2 | none[footnote 18] | |
| Country of origin | |||
| Avoid repeats | Some repeats | ||
| Northern Africa | 1 | 3 | |
| Eastern Africa | 1 | 4 | |
| Middle / Southern / Western Africa | 1 | 5 | |
| Latin America | 1 | 3 | |
| Northern America | 1 | 2 | |
| Central Asia | 1 | 1[footnote 19] | |
| Eastern Asia | 1 | 2 | |
| South-Eastern Asia | 1 | 3 | |
| Southern Asia | 1 | 5 | |
| Western Asia | 1 | 6 | |
| Eastern Europe | 1 | 3 | |
| Southern Europe | 1 | 3 | |
| Children status | |||
| With | 5 | 12 | |
| Without | No quota | 28 | |
| Visa / type of leave on entering the scheme | |||
| Domestic abuse: DVILR, DDVC | At least 2 | 3[footnote 20] | |
| Modern slavery: Modern slavery | At least 2 | 1[footnote 21] | |
| Asylum: Asylum & humanitarian protection | At least 2 | 4 | |
| EU visa (non family) + work / study / visit: EU Free movement, EUSS PSS, EUSS SS, work, study, visit | At least 2 | 11 | |
| Family (DDVC eligible): EUSS family permit, family settlement, EEA family permit | At least 2 | 8 | |
| Family (non DDVC eligible): Work-dependent, Study-dependent, Family reunion | At least 2 | 4 | |
| Other: LOTR, other, blanks, unknown | No quota | 4 | |
| None: no permission / route | At least 2 | 5 | |
| Secondary criteria: | Disability | Aim for some with disability | Some diversity |
| Sexual orientation | Aim for range & diversity | Some diversity | |
| Religion | Aim for range & diversity | Some diversity | |
| Age | Aim for range & diversity | Some diversity | |
| Length of time in scheme | Aim for range & diversity | Some diversity |
Achieved sample
Our achieved interview sample was composed entirely of victims/survivors who identified as heterosexual women, and we did not speak to any victims/survivors who reported disabilities. However, our sample was highly diverse with respect to nationality, ethnicity, age, and marital status. We spoke to respondents from a range of regions, including South East Asia (n=8), the Middle East (n=4), Central Asia (n=2), Sub-Saharan Africa (n=2), Eastern Europe (n=1) and the Caribbean (n=1). This included women who self-described as white, Asian/Asian British, Arab, and Black/Caribbean/Black British. We were able to sample victims/survivors across all delivery partners who partook in the Pilot, except Bawso, who did not share details of victims/survivors who were willing to be interviewed as part of the evaluation. The age range was also wide, with our sample including participants between 20 to 24 years of age through to 45 to 49 years of age. The sample included victims/survivors who were unmarried, separated, divorced, and still married/in a civil partnership; and included victims/survivors with no children, young children (0 to 4) and older children (5 to 17), as well as one woman who was pregnant.
If we had permission from the victim/survivor and felt the need to further discuss the case, we followed up with a phone conversation with their caseworkers. This yielded 6 informal interviews with caseworkers. This included speaking to caseworkers from Southall Black Sisters, Ashiana, Shakti and Birmingham & Solihull Women’s Aid.
Table 13: Interview sample split across different delivery partners
| Organisation[footnote 22] | Number of interviewees | Number of caseworkers |
|---|---|---|
| Core delivery partners[footnote 23] | ||
| Southall Black Sisters | 4 | 1 |
| Birmingham & Solihull Women’s Aid | 4 | 2 |
| Ashiana Sheffield | 4 | 1 |
| Shakti Women’s Aid | 3 | 2 |
| Foyle Women’s Aid | 1 | 0 |
| Bawso | 0 | 0 |
| Additional delivery partners, funded through the funding pot[footnote 24] | ||
| Iranian and Kurdish Women’s Rights Organisation (IKWRO) | 1 | 0 |
| Safety for Sisters | 1 | 0 |
| Total | 18 | 6 |
8.5.2 Interview process
Interviews were conducted between February and May 2022 and featured semi-structured phone and in-person interviews following a pre-agreed topic guide (see Annex 8.3). Interviews were recorded (when permission was granted by the participant) and professionally transcribed. Caseworkers were present in some of the interviews, and we arranged interpreters when needed.
With victims/survivors’ permission, we conducted some follow-up conversations with caseworkers after the interviews. Discussions with caseworkers were more unstructured and were not recorded.
All of the data collection was conducted exclusively by independent researchers from BIT.
8.5.3 Interview analysis
The analysis was conducted using the Framework Approach, which is a qualitative method that enables researchers to systematically analyse qualitative data and spot patterns across different participants[footnote 25]. The framework operated as a detailed coding guide, supporting researchers to retrieve data from interviews on specific themes (for example, accommodation facilities and amenities) and enabling cross-checking of findings in the team. We analysed the qualitative data using a mixture of magnitude and thematic coding. Magnitude coding records whether participants were positive, neutral, or negative about a specific theme, for example, accommodation to explore the range of experiences. Thematic coding explores the data to synthesise recurring themes and experiences.
Two researchers worked on the analysis and to reduce researcher bias. We used co-coding, a method where more than one researcher reviews the transcript, which can highlight discrepancies in the interpretation of the data.
8.5.4 Limitations
There were 2 limitations to the interviews. First, the sample for interviews was largely determined by delivery partners (see Annex 8.2 for details). This meant that we were not able to ensure complete diversity across our sample (for example, we did not speak to any male victims/survivors). It also meant we were restricted to victims/survivors that delivery partners were still in contact with, which may have excluded those who have completely disengaged from the Pilot or who may have had particularly negative experiences. Despite these challenges, we obtained a range of positive and negative reports, which typically signals that bias is unlikely to be detrimental to the research’s rigour.
The second limitation was due to language and interpretation. We had to rely on interpreters for several interviews because of the linguistic diversity of the sample. The use of interpreters to mediate the interviews may have introduced a loss of colour and nuance from the responses of the participants.
8.6 Research materials
8.6.1 Survey of support providers
Introduction & information sheet
Thank you for participating in this survey which aims to build a comprehensive picture of support available to victims/survivors of domestic abuse across the UK, including those with ‘No Recourse to Public Funds’ (NRPF). We are conducting this survey as part of the evaluation of the Home Office funded ‘Support for Migrant Victims Pilot’.
We really appreciate your time.
The Behavioural Insights Team (BIT) are conducting this survey on behalf of the Home Office. Please click here if you would like information on this research, as well as contact details should you wish to speak to someone in our research team.
Only the researchers at BIT will have access to your individual responses. BIT will share aggregate information with Home Office Analysis & Insight, who will not be able to see responses for individual organisations. Please see BIT’s Privacy Policy for further information on how your data will be used and stored.
By clicking “Next Page”, you are consenting to participate in the research. If you wish to withdraw your consent, find out more about the research, or withdraw your information after you have completed the survey, please contact {name} ({name}@bi.team).
In this section, we will ask you about the services that your organisation provides.
- What is the name of the organisation you are answering on behalf of? *
-
How would you describe the organisation you are answering on behalf of? *
- domestic abuse / Violence Against Women and Girls (VAWG) service provider
- immigration support provider (excluding legal advice)
- other (please specify below)
- please specify below if you clicked “other”
-
Who do you provide services to? Please tick all that apply. *
- migrant victims with access to public funds
- migrant victims with `No Recourse to Public Funds’ (NRPF)
- non-migrant victims/survivors
-
Which services do you provide (whether directly or outsourced to another provider)? Please tick all that apply.
Answer options: My organisation provides this internally; My organisation outsources this;
- refuge and/or accommodation
- counselling
- legal services
- immigration advice
- confidential helpline
- additional support for children
- outings
- safety planning
- support groups
- group therapy/work
- advocacy/casework
- signpost to housing
- signpost to police
- signpost to social workers
- signpost to solicitors
- subsistence
- I don’t know what services are provided
-
To which of the below do you provide services? Please tick all that apply. *
- men
- women
- children
- I don’t know who services are provided to
- other (please specify)
-
Which countries are your domestic abuse service(s) based in? Please tick all that apply. *
- England
- Scotland
- Wales
- Northern Ireland
- I don’t know where our services are based
- countries outside of the UK (please specify)
-
We are trying to build the most complete picture possible of support services for victims/survivors, with a focus on refuge services. Please provide details of any providers that we may not be aware of who provide refuge services to migrants so that we can ask them to complete this survey. We are particularly interested in small or highly localised providers that may not be captured in large public datasets. Please could you provide us with:
- Name of contact.
- Organisation.
- Telephone number or email address (if known).
-
Which regions in England are your domestic abuse service(s) based in? Please tick all that apply. *
- North East
- North West
- South East
- South West
- East Midlands
- West Midlands
- London
- Yorkshire and the Humber
- East of England
- I don’t know where our services are based
-
Please enter the number of victims/survivors of domestic abuse your organisation provided support for in the past 2 financial years. Please provide an estimate if you are unable to provide exact figures. If you don’t know the answer, please type “don’t know” in the comment box. Answer options: Number of victims/survivors with recourse to public funds (estimate if unknown); Number of victims/survivors with NRPF (estimate if unknown)
- 2020 to 2021 financial year
- 2019 to 2020 financial year
Please provide a comment if there is anything else we should know, or enter “don’t know” if you don’t know the answer
-
Which services do you provide to victims/survivors? Please tick which apply. Answer options: Migrant victims with recourse to public funds; Migrant victims with NRPF
- refuge and/or accommodation
- counselling
- legal services
- immigration advice
- confidential helpline
- additional support for children
- outings
- safety planning
- support groups
- group therapy/work
- advocacy/casework
- signpost to housing
- signpost to police
- signpost to social workers
- signpost to solicitors
- subsistence
- other (please specify below)
- please specify below if you clicked “other”
- Please could you comment on whether there are any needs of victims/survivors of domestic abuse with `No Recourse to Public Funds’ that you feel are not being met by service providers.
-
In financial year 2020 to 2021, did you have to turn any victims/survivors with `No Recourse to Public Funds’ away from your services? *
- yes
- no
-
In financial year 2020 to 2021, how many victims/survivors with `No Recourse to Public Funds’ (NRPF) have you had to turn away? Please provide an estimate if you are unable to provide exact figures. If you don’t know the answer, please type “don’t know” in the comment box. Number of individuals (estimate if unknown)
- migrant victims with NRPF
Please provide a comment if there is anything else we should know, or enter “don’t know” if you don’t know the answer
- migrant victims with NRPF
- Are there any further comments or details that you would like to share?
8.6.2 Monitoring data variables
The monitoring data template was developed by the Home Office and SBS prior to the evaluation start. The following variables were included in the monitoring data collection file:
- partner code
- partner
- service user No.
- month
- victims with NRPF receiving support each month
- victim with NRPF turned away
- counselling provided
- support groups provided
- group therapy/work provided
- advocacy/casework provided
- sign post to solicitors provided
- accommodation/ `Subsistence provided
- other provided
- counselling costs
- support groups costs
- group therapy/work costs
- advocacy/casework costs
- sign post to solicitors costs
- accommodation/subsistence costs
- other costs
- cost of services provided (£)
- gender
- age
- sexual orientation
- disability
- nationality
- ethnicity
- marital status
- if have children, how many
- age of children
- religion
- immigration status on entry to the UK
- immigration status on entry to the UK (what the victim believes)
- type of visa on entry to the UK
- type of visa victim believes they entered the UK on
- immigration status on scheme entry
- immigration status on scheme entry (what the victim believes)
- visa / type of leave on scheme entry
- visa / type of leave on scheme entry (what the victim believes)
- immigration status on exiting of the scheme
- immigration status on exiting of the scheme (what the victim believes)
- visa / type of leave on exiting the scheme
- visa / type of leave on exiting the scheme (what the victim believes)
- documentation used to confirm immigration status
- country of origin
- route of entrance to the UK
- counselling needed
- support groups needed
- group therapy/work needed
- advocacy/casework needed
- sign post to solicitors needed
- accommodation/subsistence needed
- mental health services needed
- subsistence misuse services needed
- other needed
- length of time of service provided
- outcome
- overall duration of stay in the provision in weeks and days
- the number other services the victim has been to before reaching the current provider
- comments
8.6.3 Interview guide
Consent Statement - 3 min
[Important: Before you begin, read the Consent Statement to the participant. You should not conduct an interview if they do not want to participate.]
I am from the Behavioural Insights Team, an organisation that works to provide advice and guidance to government and other organisations on how to improve their public services and programmes. We are currently working with the Home Office to understand the impact of support for migrant victims of domestic abuse, like the support you’ve received from [insert organisation].
We would like to talk to you about your experience of the support, but we’ll only do that if you’re happy to talk with us. Our goal is to understand how the support is currently offered and what additional things you think could be done to address your needs and those of others in a similar situation. If you agree, we will interview you for roughly 45 minutes asking you about your experiences and thoughts on the support you received. Some of the questions may be difficult to talk about, but you can stop the interview at any time, or skip a question.
The purpose of this interview is purely to assess the quality of services the program is able to provide. This interview will not be used to determine anything in relation to your immigration status and we will not be collecting any personal information about who you are, such as your name, age or nationality.
We will take notes during the interview. We would also like to make an audio recording, if you are happy for us to. The notes and recording (should you agree to us making one) will only be shared with staff at the Behavioural Insights Team. All notes will be kept strictly confidential and only used for the purposes we’ve just mentioned. They will be stored on a password-protected computer, which only [BIT to insert final number] researchers on the direct project team will be able to access. All notes and recordings will be deleted at the end of the project.
At the end of our research, we’ll write a report for the Home Office, which may be published. This report may include direct quotes from our interview. However, we will not share your name or add any information that people could use to identify you.
Do you have any questions for me at this point? [answer any questions]
Now I will read out a few questions to you. Please answer yes or no to each. [pause for participant to say yes/ no after each question]
- Do you understand what the interview involves?
- Have you been able to ask any questions you might have?
- Do you understand that this is a voluntary interview, that you can choose to end at any time, without giving a reason?
- Are you happy for us to securely store the notes from this interview?
- Are you happy for us to share what we have learned from this interview in a note to the Home Office so that they can understand the support being provided? It will all be anonymous – we will never name you, and the Home Office will not be able to identify you.
- Are you happy to participate in the interview?
[Only continue if the participant has answered ‘yes’ to all questions]
- Are you happy for us to take an audio recording of the interview?
- [if yes to above] Are you happy for us to securely store the recording from this interview?
[If participant has given consent to record, turn on audio recorder; if no consent to record, take notes]
[If verbal consent and consent to record given: Turn on recorder to record consent]
Since I will need a record of your consent, can I check again that you understand what this interview is about and that you are happy to participate and have the notes securely stored?
Introduction - 2 min
[Before you begin, please make sure to ask the participant where they would feel most comfortable completing the interview, and whether they would like someone else to be present or a door to be left open (if using an office space).]
Thank you for agreeing to spend some time talking with me today. The purpose of this interview is to understand your experience of the support you’ve received from [insert organisation].
During the next 45 minutes, I’m going to ask you a series of questions about yourself, the kinds of support you received, and the impact of this support. Please note that the questions I am going to ask don’t have right or wrong answers, we are interested in hearing about your experience. Also, as we discussed just now, this conversation is completely confidential, which means that no one will know what we’ve discussed, and we will not share any unique details of your case with the Home Office. We can also skip any questions you prefer not to answer.
Before we get started, do you have any questions for me?
Topic 0: General Questions - 5 min
[The aim of this section is to settle the interviewee and build trust. You should have spoken to their caseworker already and draw on things you have learned from that conversation. However, if this is not possible, the question below can help lead into Topic 1.]
- To start, can you tell me how long you’ve been in contact with [insert name of organisation]?
Topic 1: Experience of the programme - 10 min
[Explain to the interviewee that this section will be questions surrounding the type of support they received and their experience of it. Reassure them there are no right and wrong answers]
-
How did you learn about [insert name of organisation] and the support you could receive from them?
- How did you come to be in contact with the organisation?
- When did you first get in touch with [insert name of organisation]?
- Were there any barriers to you coming forward? If so, what were they?
-
What was your first meeting with [insert name of organisation] like?
- Can you describe the sign-up or registration process?
- How long did it take for you to start receiving support after you registered?
-
What types of support have you received?
- Did you receive refuge accommodation?
- [If yes] what was this process like?
- In what other ways did the program support you?
- How long do you expect this type of support will last?
- Were you offered any other support that we haven’t already mentioned?
- Did you receive refuge accommodation?
Topic 2: Benefits of the programme - 5 min
[Introduce that this section includes questions to understand the benefits of the program]
-
What parts of the support did you find most helpful?
- Were there any services, resources or people that you remember in particular?
- How did that help you?
- Were there any services, resources or people that you remember in particular?
Topic 3: Limitations of the programme - 7 min
[Explain that this section will ask questions about how the programme could be designed to provide better support. Remind the participant that their responses are confidential and will not be shared with [insert organisation].]
-
When you think about your experience seeking support from [insert organisation] were there any parts of it that you would change?
- [If yes] what parts?
- Why?
-
Was there any support that you felt you needed but you didn’t get help with?
- [If yes] what kinds
- Why would this type of support have been helpful?
- Did you manage to receive this, or other support from any other sources?
- Have you experienced any other challenges or issues that you’d like to share?
Topic 4: Potential effects of the programme on independence - 5 min
[Explain that this section will ask questions about how they are feeling currently. Remind the participant that they can stop the interview or skip a question at any time if they would prefer not to answer.]
-
Can you describe a bit to us how your life looks now since you first received support? [prompt if necessary: living situation, daily life, level of stability, independence]
- How do you feel about your financial situation?
- Are there any specific financial challenges you’re facing?
Topic 5: Potential effects of the programme on wellbeing - 3 min
[Inform the interviewee that this is the final section of the interview, and it is about how they are feeling now overall.]
- Can you describe how the programme has impacted your wellbeing?
Wrap up - 5 min
[Let the interviewee know that this is the last question, and an opportunity for them to mention anything else they would like, or feel is important]
- Is there anything else you would like to tell me? [Inform the interviewee that we have now reached the end of the interview. Let them know what kind of support is available to them (from the list created with DPs in advance) if they feel they need to talk to someone after the discussion.]
- Do you have any questions about the interview?
- As part of this research, we would like to talk to a few case workers about their impressions of the programme. This would mean that we ask them about your case, but we will not tell them about anything that you have told us today. We will only do so if that is ok with you. Would you be comfortable with us speaking to your case worker? [If the participant seems unsure, give them a chance to think about it and get back to you later. Do not ask them to make a decision on the spot.]
[To conclude:
- bring the interviewee back to a neutral place, for example by circling back to some of the interests they mentioned in the first section
- thank the interviewee for their time and let them know that their answers will help us to share insights that can shape the future direction of the program
- provide contact details in case they would like to follow up]
8.6.4 Safeguarding and Distress Protocol
Safeguarding means protecting the health, wellbeing and human rights of adults at risk, enabling them to live safely, free from abuse, violence and neglect. It is about working to prevent and reduce both the risks and experience of abuse, violence or neglect.
Prior to any interviews taking place, interviewers should review the BIT’s Adult Safeguarding Policy.
This protocol is also designed to protect victims/survivors from distress during qualitative interviewing, as they have been identified as a vulnerable group. Where distress is minor, it doesn’t mean that the victim/survivor does not want to take part in the interview. It can often feel important to interviewees to share their story, even if it is upsetting, so using techniques, such as taking short breaks, can often be helpful. However, where distress is significant, the interviewer should be prepared to handle the issue, and be ready to report safeguarding concerns. This document outlines the different procedures to follow to minimise the risk of distress as a result of taking part in interviews and enable interviewers to identify and report any safeguarding concerns.
Timeline - safeguarding and distress protocol
1 week before
Book in a call with the victim/survivor’s case worker to understand a bit about their background, including their reason for reaching out, and their level of English (to make sure appropriate provision is in place) [TBC]
Contact the victim/survivor to:
- introduce yourself and start establishing a rapport
- finalise the date/time
- agree whether in person or online/phone [if in person, make sure they are comfortable with the location]
- offer them the opportunity to have someone else present
- if in person, they can bring a trusted person with them
- if online/phone, check if they would like someone from the DP to join the call, and/or if they need interpretation
In the case where victims/survivors do not have a phone or email and the meeting is entirely arranged by the DP, send a message to the DP to pass on to the victim/survivor to start building trust.
1 day before
Send a message to the victim/survivor with a reminder of the interview, and checking they are still happy with the setup.
During the interview
The interviewer has a responsibility to be alert to evidence of abuse, violence and neglect; and to be ready and willing to act on suspicions. It is also our ethical responsibility to ensure that any signs of distress are identified and addressed. Follow the appropriate procedures (outlined below) for signs of distress and safeguarding concerns.
At the end of the interview, share with the victim/survivor a list of sources of support / resources they can access should they feel the need to.
After interview
Send victim/survivor a message thanking them for their time, sharing the list of resources again, and reminding them they can reach out any time if they have follow-up questions about the interview.
Procedures to follow - during the interview
Prior to any interviews taking place, interviewers should review the Adult Safeguarding Policy and the Risk table which outlines some of the safeguarding risks to look out for.
At the start of the interview
- inform the participant that they may end the interview at any time, and without the need for an explanation – and that they will receive any participation payments regardless
- identify any topics that will be discussed that may cause distress and confirm that the participant is willing and able to proceed; if they are not, either end the interview, or with participant agreement, proceed but without canvassing the topics identified as distressing
Signs of distress: what to do
- look out for verbal and non-verbal signs of distress; for example, this may include:
- reluctance to answer (extended pauses, evasive responses, declining to answer numerous questions)
- uncomfortable body language (shifting in seat, looking away from the interviewer)
- visible upset
- asking to end the interview
- if a participant is becoming distressed:
- remain calm, empathetic and non-judgemental
- check with them to understand if they are feeling anxious or distressed (for example, by asking “What are you feeling at the moment?”)
- offer to turn off the audio recording and to pause the interview or to end the interview
- if they choose not to continue, the interview is ended immediately; otherwise, the researcher may pause as long as necessary and resume the interview
- offer to call a person whom the interviewee trusts (for example, their case worker)
- encourage the participant to seek formal help and offer to do so on their behalf, if they wish
- after the interview:
- make a note of the incident
- debrief internally to discuss concerns. Inform HO if serious
- ensure that the organisation supporting the victim/survivor is informed of the incident, most likely through the caseworker
- ensure that the caseworker or organisation makes a courtesy call the next day or defer to their procedures
Safeguarding concerns: what to do
- note: on top of the safeguarding plan below, the interviewer should also simultaneously address the interviewee’s distress, if present (see above guidance)
- if you have concerns that the interviewee is disclosing evidence of abuse, violence or neglect, you should follow these steps:
-
step 1: is there an immediate risk of harm to the interviewee or others?
- if yes: call the police or other emergency services as soon as possible; follow up with an emergency report to Ruth Persian (Designated Senior Person - DSP)
- if no: proceed to step 2
-
step 2: establish an understanding of what has happened
- keep questions to the minimum necessary to ensure a clear and accurate understanding of what has been disclosed; remember to only ask questions to help establish whether they are at risk of harm; do not make allegations or lead them to make allegations
- if you notice something concerning, which hasn’t been disclosed: ask open questions to establish if there is an explanation for example, “that looks like a big bruise; can you tell me what happened?”
-
step 3: make a written record
- note down what has been said, any physical evidence that is available including injuries or the personal state of the interviewee
-
step 4: inform the interviewee
- if you consider that there is a risk, inform them that you need to tell an appropriate authority about what has been discussed
-
step 5: report the concerns
- to the appropriate person at the client / partner and to the DSP as soon as reasonably possible
- be available to the safeguarding leads and DSP to assist with further assessments, including whether cases need to be escalated to other parties such as the policy and / or child protection services
- if in doubt: always discuss concerns with DSP
8.6.5 Focus Group Discussion Guide - Case Workers
| Topic | Aims | Timing |
|---|---|---|
| Set-up | Providing background information and getting verbal consent | 5 mins |
| Background | To understand participant roles and experiences with service provision. | 10 mins |
| Core elements of Pilot | Core research question: What support do victims/survivors receive through the Pilot?To understand what services are provided, which are most utilised, how the users approach the service etc. | 25 mins |
| Limitations of the Pilot | Core research question: What are the limitations of support received through the Pilot? To understand the main factors preventing provision of support, barriers to help seeking through the Pilot and reasons for disengagement where relevant. | 25 mins |
| Ending support and impact | Core research question: What are the potential effects of the Pilot on victims/survivors?To understand disengagement with the Pilot and impact on victims/survivors. | 15 mins |
| Wrap up | To get a reflective assessment of Pilot support, and provide a space for any aspects not captured. | 5 mins |
NOTE TO FACILITATOR: READ THIS: Important things to keep in mind when doing the interviews
- the main question is in bold; you do NOT need to ask all the sub-questions and use all the probes; follow what the participant is saying and probe into those topics, while trying to make sure to get a wide-angle view, as well as diving deep into specific topics
- always follow-up and probe to understand ‘why’ and ‘how’; the aim is to get to the why things are done the way they are done and what’s helping and getting in the way of service provision for victim/survivor’s
- use open-ended questions - ‘what’, ‘how’, ‘in what ways’, ‘can you tell me more about’; avoid close-ended questions which result in yes/ no answers, for example, ‘is this’, ‘did you’
Set-up - 5 mins
Introductions - to yourself and BIT
Provide background info
- the Pilot is a pilot that aims to provide a support net for victim/survivor s of domestic abuse who do not have access to public funds and, as a result of these restrictions, are unable to access safe accommodation in order to escape abusive relationships
- the BIT are conducting an evaluation which seeks to establish how the SMV pilot scheme is implemented, the challenges it faces and how it could be improved
- we know that each of you are specialists in this field and have a lot of experience in supporting victim/survivors; whilst this is really important, we ask that for the next 90 minutes you refrain from discussing wider experiences of victims and focus on the SMV pilot scheme and the victims which you have assisted through the scheme
Provide focus group details - Should take up to 90 mins
- aim of this focus group is to understand your experiences and views about the SMV pilot scheme; we really want to hear about what the Pilot looks like in practice, specifically what works well about it, what doesn’t, and why
- we would like to know your thoughts and point of view - there are no right or wrong answers to any of the questions and anything that you have to say will be valuable to us
- we may prompt you or call on you by name, but you are under no obligation to answer any of the questions. If anything makes you uncomfortable or you simply do not know the answer, please just say
- thank all participants for taking the time to speak with us
Reiterate key points
- but, anything you say in this discussion will be anonymised before sharing it with others; in any reports, information will be presented in aggregate, quotes de-identified and no names will be used
- if you feel uncomfortable answering a question, we can just skip it or we can stop the interview
- we will be taking notes throughout (so there are 2 of us) but no names will be formally recorded
Check if they have any questions before starting
Gain consent - Are you happy to start the focus group?
Background - 10 mins
[To understand participant roles and experiences with service provision.] To get to know you, I’d like to hear a bit about what you do.
Can you tell me:
- what is your role?
- how many victims have you supported through the SMV pilot scheme?
- what do you like most about your role?
NOTE TO FACILITATOR: Ask the above questions collectively. Move around the room and allow each participant to respond to all three questions. Try to keep this to 90 seconds per participant. No need to probe here, this is just an introduction to ease people into the FG.
9:15 Core elements of the Pilot - 25 minutes
[To understand what services are provided, which are most utilised, how the users approach the service etc.]
For this focus group, I have structured the conversation into sections. We will focus first on the core elements of the Pilot, then discuss limitations and end by discussing wider implications of the Pilot on victim experiences.
[If participants bring up limitations in this section, remind them that you will discuss limitations next and first want to understand the core Pilot offer]
First of all we are going to discuss the core elements of the Pilot as well as your perceptions of how the Pilot works in practice. What types of support are provided to victims/survivors through the Pilot?
- probe: accomodation, financial, mental health, medical, legal, safety plans?
Are there any additional support services the Pilot connects them to?
- probe: counselling, therapy, immigration lawyers, medical, immediate safe spaces, family and children, sexual health, community forums, education, language/translation
can you tell me more about what that support involves?
- potential rephrase: what does that look like in practice?
- is support offered to any other people beyond the victim/survivor themselves? Probe - children, family members, friends?
Which aspects of support are most often used by victims/survivors?
- why is that support accessed more?
- which are the easiest to access for victims/survivors? Why?
- which aspects of support do victims/survivors benefit most from? Why?
- which are the easiest for you to arrange for victims/survivors? Why?
- do responses to support vary between victims/survivors? If so, how?
Which aspects of support are least often used by victims/survivors?
- why is that support accessed less?
- which are the most challenging aspects to arrange? Why?
- which are the most challenging to encourage victims/survivors to take up? Why?
- which aspects have the least impact on victims/survivors? Why?
- how could these aspects of the Pilot be improved?
[Optional: skip if 30 mins into FGD already] I’d like to understand what the journey of support looks like for a victim/survivor. Which services are offered to victims/survivors first?
- does this vary from case to case? How are victims prioritised in terms of which support services they can access?
- how does a case worker decide which support services to offer to which victims? What is the process for deciding this?
- how long will it take them to access that support?
- does timing vary dependent upon which services are being offered? If so, which services take longer to provide? Which services can be provided immediately? How often is this done?
Considering your role as a case worker, what do you perceive to be the most crucial part of the Pilot and why?
9:40 Limitations of the Pilot - 25 minutes
[To understand the main factors preventing provision of support, barriers to help seeking through the Pilot and reasons for disengagement where relevant.]
Next, I’d like to focus on challenges you and victims/survivors face with the Pilot. What do you understand to be the main challenges associated with the Pilot?
- probe: languages, finances, access to immigration lawyers, lack of trust, lack of understanding, lack of consistency, fear of repercussions, Children’s Act?
- at what stage in the process of support provision are those challenges most clear?
- are the challenges to service provision attributed to the Pilot not having access to the service requested or barriers from a victim perspective?
[Option, time dependent] Have you encountered victims/survivors disengaging from the Pilot? What are the main reasons that happens?
- if they disengage, at which points do they tend to disengage with the support?
- what portion of your victims/survivors disengage?
- how consistently do victims/survivors disengage?
- are there any processes in place for when a victim/survivor begins to disengage?
Are there any types of support that you feel victims/survivors need but are unable to access through the Pilot?
- what are the most commonly requested services which the Pilot are unable to arrange? Why?
- how often are services requested which the Pilot do not provide?
[Option, time dependent] If you were given unlimited resources, what 3 aspects of the Pilot would you change and why?
10:05 Ending support and impact - 15 mins
[To understand disengagement with the Pilot and impact on victims/survivors.]
Next, I’d like to spend a bit of time understanding the end of support and your perceptions of the impact on victims/survivors. [Can be cut if overrunning] When does a victim stop receiving support from the Pilot? In what circumstances?
- is there a process in place for when support finishes? Does this vary from case to case?
- do you have any ongoing contact with victims/survivors after that? What does that look like?
[Can be cut if overrunning] Describe the process victims/survivors have to follow when they end support.
What impact do you see the support having on victims/survivors?
- how can that impact be improved?
- if you had to identify one key cause for that impact not being maximised, what would that be?
The next 2 questions are more sensitive. However, it is important for us to understand the full range of victim/survivor experiences, and we will not ask victims/survivors these questions to avoid distressing them.
Thinking about the victims that you have supported through the Pilot, what have victims/survivors relationships with the perpetrator been like at the end of the support?
- how many are still in contact?
- what affects that?
How would you describe victims/survivors immigration outcomes at the end of the support?
- considering the cases you have worked on, how many victims/survivors do you believe want to stay in the UK?
- what barriers do they face in being able to do that?
- how many do (or will) remain in the UK to your knowledge?
- what barriers do you think they face?
10:20 Wrap up - 5 mins
[]
To end with, I would like to know your opinion of how effective you think the Pilot is in offering comprehensive, wrap-around support for victims/survivors.
If I presented you with a scale of 1 to 10 with 1 representing a victim receiving absolutely zero support and 10 representing a victim becoming completely independent from the perpetrator and empowered in all other aspects of their lives, where on this scale would you put the support currently provided by the Pilot?
Lastly, is there anything I did not ask that you wish I had? Anything you would like to add or clarify?
We have come to the end of the focus group. I would like to thank each of you for taking the time to speak with me today and for providing me with your raw and honest reflections of the Pilot. I remind you that everything discussed today will be de-identified as we take this forward within the project.
Should you have any further questions regarding this research, please contact Bridie Murphy, who was arranging this Focus Group with you.
8.6.6 Focus Group Discussion Guide - Case Managers
| Topic | Aims | Timing |
|---|---|---|
| Set-up | Providing background information and getting verbal consent | 5 mins |
| Background | To understand participant roles and experiences with service provision. | 10 mins |
| Understanding the core elements of the Pilot | Core research question: What support do victims/survivors receive through the Pilot?To understand what services are provided, how these are arranged and maintained and which are most utilised. | 20 mins |
| Limitations of the Pilot | Core research question: What are the limitations of support received through the Pilot? To understand the main factors preventing provision of support, barriers to help seeking through the Pilot and friction towards | 30 mins |
| Wider impact of the Pilot | Core research question: What are the potential effects of the Pilot on victims/survivors?To understand disengagement with the Pilot and impact on victims/survivors. | 15 mins |
| Wrap up | Closing remarks, thanks and next steps. | 5 mins |
NOTE TO FACILITATOR: READ THIS: Important things to keep in mind when doing the interviews
- the main question is in bold; you do NOT need to ask all the sub-questions and use all the probes; follow what the participant is saying and probe into those topics, while trying to make sure to get a wide-angle view, as well as diving deep into specific topics.
- always follow-up and probe to understand ‘why’ and ‘how’ ; the aim is to get to the why things are done the way they are done and what’s helping and getting in the way of service provision for victim/survivors.
- use open-ended questions - ‘what’, ‘how’, ‘in what ways’, ‘can you tell me more about’; avoid close-ended questions which result in yes/ no answers, for example, ‘is this’, ‘did you’
Set-up - 5 mins
Introductions - to yourself and BIT
Provide background info
- the Pilot is a pilot that aims to provide a support net for victim/survivors of domestic abuse who do not have access to public funds and, as a result of these restrictions, are unable to access safe accommodation in order to escape abusive relationships
- BIT are conducting an evaluation which seeks to establish how the SMV pilot scheme is implemented, the challenges it faces and how it could be improved
- we know that each of you are specialists in this field and have a lot of experience in supporting victim/survivor’s; whilst this is really important, we ask that for the next 90 minutes you refrain from discussing wider experiences of victims and focus on the SMV pilot scheme and the victims which you have assisted through the scheme
Provide focus group details - Should take up to 90 mins
-
aim of this focus group is to understand your experiences and views about the SMV pilot scheme. We really want to hear about what the Pilot looks like in practise, specifically what works well about it and what doesn’t
- we would like to know your thoughts and point of view - there are no right or wrong answers to any of the questions and anything that you have to say will be valuable to us
- we may prompt you or call on you by name, but you are under no obligation to answer any of the questions. If anything makes you uncomfortable or you simply do not know the answer, please just say
- thank all participants for taking the time to speak with us
Reiterate key points
- but, anything you say in this discussion will be anonymised before sharing it with others; in any reports, information will be presented in aggregate, quotes de-identified and no names will be used
- if you feel uncomfortable answering a question we can just skip it or we can stop the interview
- we will be taking notes throughout (so there are 2 of us) but no names will be formally recorded
Check if they have any questions before starting
Gain consent - Are you happy to start the focus group?
Background - 10 mins
[To understand participant roles and experiences with service provision.]
To get to know you, I’d like to hear a bit about what you do. Can you tell me:
- what is your role?
- how long have you been in your role for?
- what is your involvement with the Support for Migrant Victims pilot?
NOTE TO FACILITATOR: Ask the above questions collectively. Move around the room and allow each participant to respond to all three questions. Try to keep this to 90 seconds per participant. No need to probe here, this is just an introduction to ease people into the FG.
However, if you are unclear on what specific roles involve, you can return to this after the round of introductions. Optional prompts:*
- you mentioned [X]. Can you tell me what that involves day-to-day?
- how much contact do you have with the victims/survivors receiving support?
- what parts of the Pilot are you responsible for?
Understanding the core elements of the Pilot - 20 minutes
[To understand what services are provided, how these are arranged and maintained and which are most utilised]
First of all we are going to discuss the core elements of the Pilot as well as your perceptions of how the Pilot works in practice.
What types of support are provided to victims/survivors through the Pilot?
- probe: accommodation, financial, mental health, medical, legal, safety plans?
Are there any additional support services the Pilot connects them to?
- probe: counselling, therapy, immigration lawyers, medical, immediate safe spaces, family and children, sexual health, community forums, education, language/translation
- have you faced any challenges in working with those services as part of this Pilot?
What do you perceive to be the most crucial part of the Pilot and why?
Limitations of the Pilot - 30 minutes
[To understand the main factors preventing effective provision of support, and barriers to help seeking through the Pilot]
Next, I’d like to focus on challenges you face across the Pilot.
From your perspective managing the Pilot, have there been any services or Pilot elements that have been particularly challenging to deliver?
- have you faced any trouble in meeting demand for certain services?
- have there been any aspects of the support you haven’t been able to deliver as you envisioned?
Are there any factors that make it harder for victims/survivors to access or engage with support?
- probe: Languages, finances, access to immigration lawyers, lack of trust, lack of understanding, lack of consistency, fear of repercussions, Children’s Act?
- at what stage in the process of support provision are the barriers most clear?
- are the barriers to service provision attributed to the Pilot not having access to the service requested or barriers from a victim perspective?
- are there any processes in place for when a victim/survivor begins to disengage?
Are there any types of support that you feel victims/survivors need but are unable to access through the Pilot?
- what are the most commonly requested services which the Pilot is unable to arrange? Why?
- how often are services requested which the Pilot does not provide?
Wider impact of the Pilot - 15 mins
[To understand the impact of the Pilot on victims/survivors.]
What impact do you see the support having on victims/survivors?
- what are the potential effects of the Pilot on victim/survivor independence?
- how can that impact be improved?
If you had to identify one key cause for that impact not being maximised, what would that be?
To end with, I would like to know your opinion of how effective you think the Pilot is in offering comprehensive, wrap-around support for victims/survivors.
If I presented you with a scale of 1 to 10 with 1 representing a victim receiving absolutely zero support and 10 representing a victim becoming completely independent from the perpetrator and empowered in all other aspects of their lives, where on this scale would you put the support currently provided by the Pilot?
Wrap up - 5 mins
Lastly, is there anything I did not ask that you wish I had? Anything you would like to add or clarify?
We have come to the end of the focus group. I would like to thank each of you for taking the time to speak with me today and for providing me with your raw and honest reflections of the Pilot. I remind you that everything discussed today will be de-identified as we take this forward within the project.
Should you have any further questions regarding this research, please contact {name}.
-
Figures for SBS include victims/survivors supported by any additional providers. ↩
-
Home Office (2020). Migrant Victims of Domestic Abuse. Review Findings. Available at: https://www.gov.uk/government/publications/migrant-victims-of-domestic-abuse-review [Accessed on: 19 July 2022]. ↩
-
HRH Queen Elizabeth II (2017). Queen’s speech. Cabinet Office. Available at: https://www.gov.uk/government/speeches/queens-speech-2017 [Accessed on: 19 July 2022]. ↩
-
House of Lords & House of Commons (2019). Draft Domestic Abuse Bill: First Report of Session 2017-2019. Available at: https://publications.parliament.uk/pa/jt201719/jtselect/jtddab/2075/2075.pdf [Accessed on: 19 July 2022]. ↩
-
Home Office (2020). Migrant Victims of Domestic Abuse. Review Findings. Available at: https://www.gov.uk/government/publications/migrant-victims-of-domestic-abuse-review [Accessed on: 19 July 2022]. ↩
-
Additional providers were funded by SBS through the Pilot. ↩
-
Process evaluations are concerned with understanding how an intervention (the Pilot) was delivered in practice, in comparison to the intended implementation. In contrast, impact evaluations are concerned with intervention effectiveness and the impact on measurable outcomes. ↩
-
Duplicates were identified by inspecting the organisation name, IP addresses and completion time. One response was identified as a duplicate from the comments. ↩
-
The Framework Approach is a qualitative method that enables researchers to systematically analyse qualitative data and spot patterns across different participants. See: Ritchie, J., Lewis, J., Nicholls, C. M., & Ormston, R. (Eds.). (2013). Qualitative research practice: A guide for social science students and researchers. Sage. ↩
-
We received more than one response from 6 organisations from different regions of operations. ↩
-
“Child support” was one of the response options, but there may be differences in what it entails across providers. Based on our other research activities, we believe this is unlikely to refer to provision of government Child Support funding. It may relate to childcare or other forms of support. ↩
-
We did receive multiple responses for six organisations with the same email address from different geographies. These were all included, as they represented different regional operations for their organisation. ↩
-
Figures for SBS include victims/survivors supported by any additional providers. ↩
-
In this graph, we have excluded data entries where there was no data on services needed (all columns were empty for the entry). This was due to data collection issues for some service providers on these variables. ↩
-
Based on provided costs; not all costs were provided for each service. ↩
-
We have included ‘grouped outcomes’ to aid understanding. This was not directly captured in the monitoring data and is subject to our interpretation. ↩
-
Duplicates were identified by inspecting the organisation name, IP addresses and completion time. One response was identified as a duplicate from the comments. ↩
-
We will aim to sample one or 2 men if we need additional sample. ↩
-
Only one victim/survivor from Central Asia in Q2 (July to September 2021) and Q3 (October to December 2021) - could look at Q1 (April to June 2021) if needed. ↩
-
Few DVILR (no DDVC) in Q2 (July to September 2021) and Q3 (October to December 2021) - could look at Q1 (April to June 2021) if needed. ↩
-
Few Modern Slavery in Q2 (July to September 2021) and Q3 (October to December 2021) - could look at Q1 (April to June 2021) if needed. ↩
-
Note, there were no interviewees from Bawso. ↩
-
Each of these delivery partners was responsible for delivering the Pilot in different regions of the UK. SBS were the primary delivery partner and responsible for administering the funding across the other delivery partners. ↩
-
These delivery partners could request funding for specific cases through SBS. ↩
-
Ritchie, J., Lewis, J., Nicholls, C. M., & Ormston, R. (Eds.). (2013). Qualitative research practice: A guide for social science students and researchers. Sage. ↩