HPR volume 15 issues 1 and 2: news (19 January 2021)
Updated 19 January 2022

© Crown copyright 2022
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/health-protection-report-volume-15-2021/hpr-volume-15-issues-1-and-2-news-19-january-2020
National norovirus and rotavirus surveillance for winter 2020 to 2021
The ongoing coronavirus (COVID-19) pandemic has adversely impacted the established national surveillance systems Public Health England (PHE) uses to monitor norovirus and rotavirus activity in England – specifically, there have likely been changes in ascertainment of these systems. Since mid-March 2020, there has been a substantial reduction in positive norovirus and rotavirus laboratory reports and enteric virus (EV) outbreak reports to PHE compared to the average for the same period during the previous 5 seasons.
It is likely that the interventions implemented to control COVID-19 have contributed to a reduction in both norovirus and rotavirus transmission – however, this decrease is considered to be multifactorial and not wholly attributable to a reduction in virus transmission.
Norovirus has the potential to cause significant disruption within the NHS and contributes to winter pressures[footnote 1]. It has been identified as a priority risk to the NHS and the ability of local health authorities to deliver the COVID-19 response this winter.
In December, PHE began publication of a fortnightly National norovirus and rotavirus bulletin for the 2020 to 2021 winter to provide an overview of activity in England. This bulletin temporarily replaces the Official Statistics national norovirus and rotavirus report, which is currently suspended due to the adverse impact of the COVID-19 pandemic on sampling and testing for enteric viruses and reporting of these results to PHE. Unfortunately, this means it is no longer possible to ensure the accuracy and consistency of this data, nor compare with that from previous seasons.
The data reported in the first bulletin, published on 17 December, provided a summary of norovirus and rotavirus activity in England up to reporting week 49 of the 2020 to 2021 season. Norovirus activity decreased substantially during weeks 12 and 13 of the 2019 to 2020 season and has remained lower than the 5-season average for the same period (2015 to 2016 and 2019 to 2020) throughout the 2020 to 2021 season. The cumulative total of norovirus laboratory reports up to week 49 of the 2020 to 2021 season (weeks 27 to 49, 2020) was 90.6% lower than 5-season average for the same period (see figure 1).
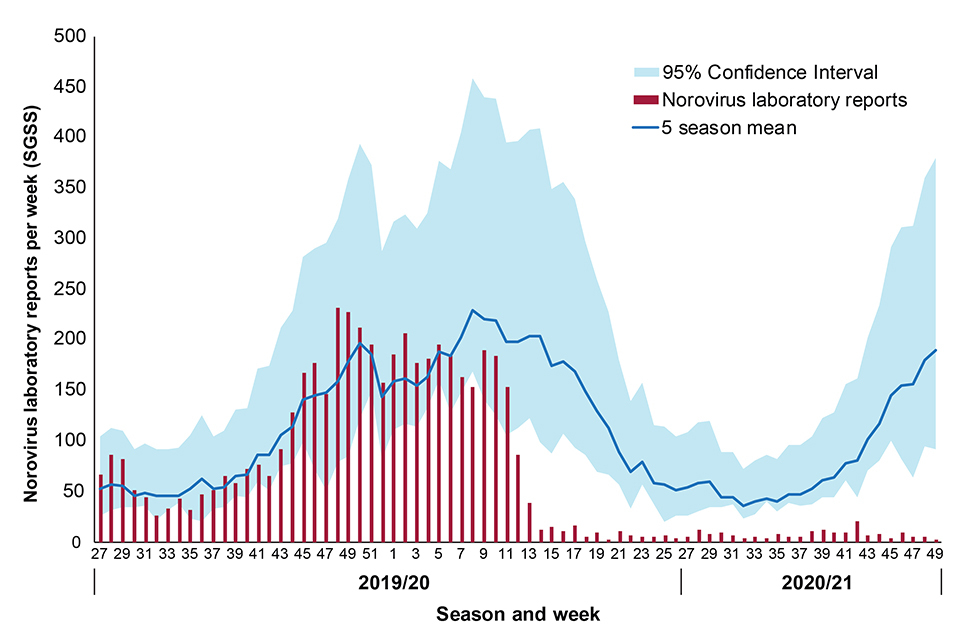
Figure 1: Cumulative total of norovirus laboratory reports up to week 49 of the 2020 to 2021 season (weeks 27 to 49, 2020).
(In order to capture the winter peak of activity in reporting period the norovirus season runs from week 27 in one year to week 26 in the next (that is, week 27, 2019, to week 26, 2020: July to June). Week number is calculated from specimen date. Data are based on laboratory geography and are faecal and lower GI tract specimen types only. Five-season averages for 2019 to 2020 and 2020 to 2021 seasons are calculated from the 5-season periods of 2014 to 2015 and 2018 to 2019, and 2015 to 2016 and 2019 to 2020, respectively.)
In addition to the new fortnightly bulletin, PHE’s Enteric Virus Unit (EVU), along with the Gastrointestinal Pathogens Unit, have developed a surveillance programme to ensure sufficient norovirus positive samples are obtained to carry out effective molecular surveillance throughout this winter. EVU provides a norovirus characterisation service to support national norovirus surveillance.
All PHE Regional Public Health and collaborating laboratories are reminded of the importance of continuing to refer samples to EVU for characterisation in order to maintain robust molecular surveillance of circulating strain diversity.
Further details for laboratories have been circulated (PHE [internal] Briefing Note 59 (December 2020). Norovirus surveillance in winter 2020 to 2021).
Infection reports in this issue
Invasive meningococcal disease (England): annual report 2019 to 2020.
Childhood vaccination coverage reports
Impact of COVID-19 on childhood vaccination to week 53.
-
Harris JP, Adams NI, Lopman BA, Allen DJ and Adak GK (2014). The development of web-based surveillance provides new insights into the burden of norovirus outbreaks in hospitals in England. Epidemiol. Infect. 142(8), 1590-1598. ↩