Global high consequence infectious disease events: summary January to August 2021
Updated 3 April 2025

© Crown copyright 2025
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/high-consequence-infectious-diseases-monthly-summaries/global-high-consequence-infectious-disease-events-summary-january-to-august-2021
Interpreting this report
The report provides detailed updates on known, high consequence infectious disease (HCID) events around the world as monitored by PHE’s epidemic intelligence activities.
It is divided into 2 sections covering all the defined HCID pathogens. The first contains contact and airborne HCIDs that have been specified for the HCID Programme by NHS England. The second section contains additional HCIDs that are important for situational awareness.
Each section contains information on known pathogens and includes descriptions of recent events. If an undiagnosed disease event occurs that could be interpreted as a potential HCID, a third section will be added to the report.
Likelihood assessment
Included for each disease is a ‘likelihood assessment’ – the likelihood of a case occurring in the UK – based on past UK experience and the global occurrence of travel-associated cases. There are currently 3 categories: Low, Very Low and Exceptionally Low.
When considering clinical history, it is important to remember that cases can and do occur outside of the usual distribution area. It is not possible to assess accurately the risk of cases presenting to healthcare providers in England but taken together it is inevitable that occasional imported cases will be seen.
Events found during routine scanning activities that occur in endemic areas will briefly be noted in the report. Active surveillance, other than daily epidemic intelligence activities, of events in endemic areas will not be conducted (for example, actively searching government websites or other sources for data on case numbers).
The target audience for this report is any healthcare professional who may be involved in HCID identification.
Incidents of significance of primary HCIDs
Contact HCIDs
Crimean-Congo haemorrhagic fever (CCHF)
| Geographical risk areas | Endemic in Central and Eastern Europe, Central Asia, the Middle East, East and West Africa. First locally acquired case in Spain 2016 (HAIRS risk assessment). |
|---|---|
| Sources and routes of infection | • bite from or crushing of an infected tick • contact with blood or tissues from infected livestock • contact with infected patients, their blood or body fluids |
| UK experience to date | Two confirmed cases (ex-Afghanistan 2012, ex-Bulgaria 2014). |
| Likelihood assessment | Low – rarely reported in travellers (23 cases in world literature). |
| Recent cases or outbreaks |
Spain has reported 2 cases of CCHF in 2021, as of the end of August. Both cases were in the region of Castile-León. In Pakistan, 5 cases of CCHF were reported in Balochistan and 2 in Sindh in 2021, as of the end of August. In April 2021, Uganda identified 2 children with confirmed CCHF, with links to a family that kept goats. CCHF is known to be present in livestock in Uganda. In Turkey, 243 cases of CCHF, including 13 deaths, were reported as of May 2021. In July 2021, media reported a fatal case of CCHF in Tbilisi, Georgia. Fatal cases of CCHF were also identified in Iraq during July 2021, in the governorates of Diyala, Kirkuk and Dhi Qar. In August 2021, cases of CCHF were reported in Stavropol and Rostov in Russia. In Kazakhstan, a case of CCHF was reported in the Kyzylorda region in August 2021. |
{kind=link}
Ebola virus disease
| Geographical risk areas | Sporadic outbreaks in Western, Central and Eastern Africa. |
|---|---|
| Sources and routes of infection | • contact or consumption of infected animal tissue (such as bushmeat) • contact with infected human blood or body fluids |
| UK experience to date | Four confirmed cases (1 lab-acquired in the UK in 1976, 3 healthcare workers associated with West African epidemic, 2014 to 2015). |
| Likelihood assessment | Very Low – other than during the West Africa outbreak, exported cases are extremely rare. |
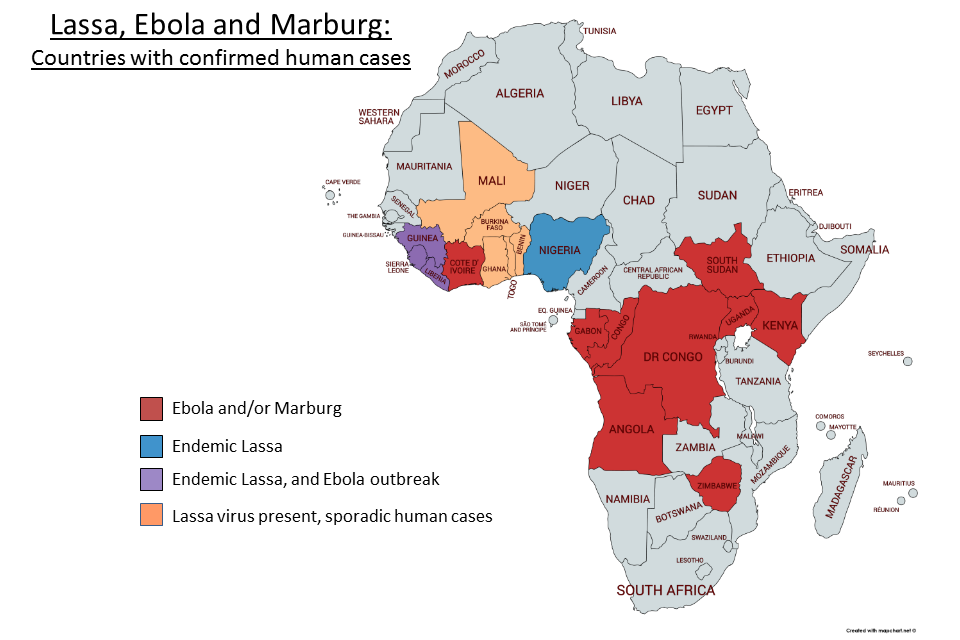
| Recent cases or outbreaks | In the Democratic Republic of the Congo (DRC), 12 cases of Ebola virus disease (11 confirmed and 1 probable) were reported in North Kivu province during an outbreak between February and May 2021. In Guinea, 23 cases (16 confirmed, 7 probable) were reported in N’zérékoré prefecture, during an outbreak between February and June 2021. On 31 August 2021, the World Health Organization (WHO) announced that no evidence of Ebola virus was found after testing an individual who was previously suspected of having Ebola virus disease in Côte d’Ivoire. Diagnosis of Ebola virus disease was also excluded in a suspected case in Burkina Faso. |
{kind=link}
Lassa fever
| Geographical risk areas | Endemic in sub-Saharan West Africa . |
|---|---|
| Sources and routes of infection | • contact with excreta, or materials contaminated with excreta from an infected rodent • inhalation of aerosols of excreta from an infected rodent • contact with infected human blood or body fluids |
| UK experience to date | Fourteen cases since 1971, all ex-West Africa. |
| Likelihood assessment | Low – overall Lassa fever is the most common imported viral haemorrhagic fever (VHF) but still rare (a total of 35 imported cases reported globally since 1969). |
| Recent cases or outbreaks | In Nigeria, there have been 2,876 suspected and 365 confirmed cases of Lassa fever so far in 2021, as of 29 August. Seventy-three deaths have been reported, with a case fatality rate of 20%. This is lower than the cases reported in the same period in 2020 (5,574 suspected, 1,072 confirmed cases and 225 deaths). COVID-19 infection prevention and control measures may have contributed to the decrease in Lassa fever cases. Liberia reported a total of 91 suspected cases of Lassa fever between 1 January and 18 August 2021, of which 15 (16.5%) were confirmed. There were 11 deaths among the confirmed cases (case fatality rate: 73%). This is a decrease compared to 2020, when 147 suspected and 40 confirmed cases were reported between 1 January and 9 August. Sierra Leone has reported 13 cases of Lassa fever in 2021, as of 5 August. There have been 9 fatalities (case fatality rate: 69%). In Guinea, 5 confirmed cases of Lassa fever including 4 deaths (case fatality rate: 80%) have been reported this year, as of 17 August. |
Marburg virus disease
| Geographical risk areas | Sporadic outbreaks in Central and Eastern Africa. |
|---|---|
| Sources and routes of infection | Contact with infected blood or body fluids. |
| UK experience to date | No known cases in the UK. |
| Likelihood assessment | Very Low – globally, 5 travel-related cases previously reported in the literature. |
| Recent cases or outbreaks | On 6 August 2021, the Ministry of Health of Guinea informed WHO of a confirmed fatal case of Marburg virus disease in Guéckédou, south-western Guinea. This is the first known case in Guinea and in West Africa. None of the contacts identified developed symptoms. The follow-up period for the contacts ended on 25 August 2021. |
Airborne HCIDs
Influenza A(H7N9) virus
| Geographical risk areas | All human infections acquired in China. |
|---|---|
| Sources and routes of infection | • close contact with infected birds or their environments • close contact with infected humans (no sustained human-to-human transmission) |
| UK experience to date | No known cases in the UK. |
| Likelihood assessment | Very Low (PHE Risk Assessment). |
| Recent cases or outbreaks | No confirmed or suspected human cases were reported between January and August 2021. |
Influenza A(H5N1) virus
| Geographical risk areas | Human cases predominantly in South East Asia, but also in Egypt, Iraq, Pakistan, Turkey and Nigeria. Highly pathogenic H5N1 in birds much more widespread, including in the UK. |
|---|---|
| Sources and routes of infection | • close contact with infected birds or their environments • close contact with infected humans (no sustained human-to-human transmission) |
| UK experience to date | No known cases in the UK. |
| Likelihood assessment | Very Low (PHE Risk Assessment). |
| Recent cases or outbreaks | In April 2021, 7 human cases of avian influenza A(H5N1) were reported in Nigeria, from Kanu (4 cases) and Plateau (3 cases) states. All cases were poultry workers and exposed to infected birds. There is no evidence of human-to-human transmission. On 21 July 2021, WHO was notified of National IHR focal point of one fatal human case of avian Influenza A(H5N1) from Haryana state, northern India. This is the first reported case of human infection of influenza A(H5N1) virus in India. The patient was under the age of 18 and had underlying health conditions. The source of infection was unknown, and no other cases were identified. |
Middle East respiratory syndrome (MERS)
| Geographical risk areas | The Arabian Peninsula – Yemen, Qatar, Oman, Bahrain, Kuwait, Saudi Arabia and United Arab Emirates. |
|---|---|
| Sources and routes of infection | • airborne particles • direct contact with contaminated environment • direct contact with camels |
| UK experience to date | Five cases in total – 3 imported cases (2012, 2013 and 2018), 2 secondary cases in close family members of the second case, 3 deaths. |
| Likelihood assessment | Very Low (PHE Risk Assessment). |
| Recent cases or outbreaks | Between January and August 2021, there were 13 cases of MERS-CoV, including 5 deaths, identified globally. Of these cases, 12 were located in Saudi Arabia and one in the United Arab Emirates. |
Monkeypox virus
| Geographical risk areas | West and Central Africa. |
|---|---|
| Sources and routes of infection | • close contact with an infected animal or human • indirect contact with contaminated material, such as bed linen |
| UK experience to date | To date, there have been 7 cases of monkeypox reported in the UK. In May 2021, a case of monkeypox was identified with prior travel from Delta State, Nigeria. Two family members were subsequently identified as having monkeypox. Prior to these 3 cases, there had been only 4 cases of monkeypox reported in the UK, including 3 cases previously imported from Nigeria (2 in September 2018 and one in December 2019). One other case, in 2018, was a healthcare worker who acquired infection following contact with contaminated bed linen. |
| Likelihood assessment | Very Low – reported outside Africa for the first time in 2018. |
| Recent cases or outbreaks |
Cases of monkeypox continue to be reported in Nigeria. In 2021, 79 suspected and 23 confirmed cases have been identified, as of 31 August. No deaths have been reported. During 2020, there were 8 confirmed cases in total. In the DRC, 2,523 cases and 66 deaths associated with monkeypox were reported between 1 January and 8 August 2021. Three confirmed cases were reported in the UK during May and June 2021 (as above). The US reported an imported case of monkeypox from Nigeria in July 2021. |
Nipah virus
| Geographical risk areas | Outbreaks in Bangladesh and India. South East Asia at risk. |
|---|---|
| Sources and routes of infection | • direct or indirect exposure to infected bats • consumption of contaminated raw date palm sap • close contact with infected pigs or humans |
| UK experience to date | No known cases in the UK. |
| Likelihood assessment | Exceptionally Low – no travel-related infections in the literature. |
| Recent cases or outbreaks | No confirmed or suspected cases were reported between January and August 2021. |
Pneumonic plague (Yersinia pestis)
| Geographical risk areas | Predominantly sub-Saharan Africa but also Asia, North Africa, South America, Western US. |
|---|---|
| Sources and routes of infection | • flea bites • close contact with infected animals • contact with human cases of pneumonic plague |
| UK experience to date | Last outbreak in the UK was in 1918. |
| Likelihood assessment | Exceptionally Low – no travel-related infections in the literature. |
| Recent cases or outbreaks | In Ituri province, DRC, 118 suspected plague cases and 13 deaths have been reported in 2021, as of 8 August. In 2020, 461 suspected cases and 31 deaths were reported in the province. Madagascar reported 21 confirmed and 37 suspected cases of bubonic plague between January and March 2021 (last data point available). An estimated 9 deaths were reported. Plague is endemic to Madagascar, where 200 to 700 cases are reported each year. In the US, one death caused by plague was reported in Colorado in July 2021 and one case of bubonic plague was confirmed in New Mexico in August 2021. China also reported a case of bubonic plague in August 2021 in a livestock worker from Inner Mongolia Autonomous Region. |
Severe acute respiratory syndrome (SARS)
| Geographical risk areas | Currently none. Two outbreaks originating from China 2002 and 2004. |
|---|---|
| Sources and routes of infection | • airborne particles • direct contact with contaminated environment |
| UK experience to date | Four cases related to 2002 outbreak. |
| Likelihood assessment | Exceptionally Low – not reported since 2004. |
| Recent cases or outbreaks | No confirmed or suspected human cases reported since 2004. |
Incidents of significance of additional HCIDs
Argentine haemorrhagic fever (Junin virus)
| Geographical risk areas | Argentina (central). Limited to the provinces of Buenos Aires, Cordoba, Santa Fe, Entre Rios and La Pampa. |
|---|---|
| Sources and routes of infection | • direct contact with infected rodents • inhalation of infectious rodent fluids and excreta • person-to-person transmission has been documented |
| UK experience to date | No known cases in the UK. |
| Likelihood assessment | Exceptionally Low – travel-related cases have never been reported. |
| Recent cases or outbreaks | No confirmed or suspected cases were reported between January and August 2021. |
Bolivian haemorrhagic fever (Machupo virus)
| Geographical risk areas | Bolivia – limited to the Department of Beni, municipalities of the provinces Iténez (Magdalena, Baures and Huacaraje) and Mamoré (Puerto Siles, San Joaquín and San Ramón). |
|---|---|
| Sources and routes of infection | • direct contact with infected rodents • inhalation of infectious rodent fluids and excreta • person-to-person transmission has been documented |
| UK experience to date | No known cases in the UK. |
| Likelihood assessment | Exceptionally Low – travel-related cases have never been reported. |
| Recent cases or outbreaks | No confirmed or suspected cases were reported between January and August 2021. |
Lujo virus disease
| Geographical risk areas | Single case acquired in Zambia lead to a cluster in South Africa in 2008. |
|---|---|
| Sources and routes of infection | • presumed rodent contact (excreta, or materials contaminated with excreta of infected rodent) • person-to-person via body fluids |
| UK experience to date | No known cases in the UK. |
| Likelihood assessment | Exceptionally Low – a single travel-related case has been reported. No cases have been reported anywhere since 2008. |
| Recent cases or outbreaks | No confirmed or suspected human cases reported since 2008. |
Severe fever with thrombocytopenia syndrome (SFTS)
| Geographical risk areas | Mainly reported from China (south-eastern), Japan and Korea. First ever cases reported in Vietnam and Taiwan in 2019. Serological evidence of SFTS in Pakistan. |
|---|---|
| Sources and routes of infection | • presumed to be tick exposure • person-to-person transmission described in household and hospital contacts, via contact with blood or bloodstained body fluids |
| UK experience to date | No known cases in the UK. |
| Likelihood assessment | Exceptionally Low – not known to have occurred in travellers. |
| Recent cases or outbreaks | In August 2021, a fatal case of SFTS was reported in Fukuoka Prefecture, Japan. The case, who was reported to have a tick bite mark, was hospitalised on 16 August and died on 21 August. Note: Chinese authorities do not provide publicly available data on cases of SFTS. |
Andes virus (Hantavirus)
| Geographical risk areas | Chile and southern Argentina. |
|---|---|
| Sources and routes of infection | • rodent contact (excreta, or materials contaminated with excreta from an infected rodent) • person-to-person transmission described in household and hospital contacts |
| UK experience to date | No known cases in the UK. |
| Likelihood assessment | Very Low – rare cases in travellers have been reported (PHE risk assessment). |
| Recent cases or outbreaks | As of August, no confirmed or suspected cases of Andes virus have been reported in 2021. Cases of hantavirus have been reported in Argentina, Chile and Taiwan by media, however, whether the cases were due to Andes virus is not confirmed. |
Influenza A(H5N6) virus
| Geographical risk areas | Mostly China. New strain in Greece in March 2017, and subsequently found in Western Europe. |
|---|---|
| Sources and routes of infection | Close contact with infected birds or their environments. |
| UK experience to date | No known cases. |
| Likelihood assessment | Very Low – not known to have occurred in travellers (PHE risk assessment). |
| Recent cases or outbreaks | In 2021, to the end of August, there have been 16 human cases of avian influenza A(H5N6) reported globally. Of these cases, 15 were reported in Mainland China and one case was detected in Laos. This was the first time a human case of avian influenza A(H5N6) was detected in Laos. |
Influenza A(H7N7) virus
| Geographical risk areas | Sporadic occurrence, including Europe and the UK. |
|---|---|
| Sources and routes of infection | • close contact with infected birds or their environments • close contact with infected humans (no sustained human-to-human transmission) |
| UK experience to date | No known cases. |
| Likelihood assessment | Very Low – human cases are rare, and severe disease even rarer. |
| Recent cases or outbreaks | No confirmed or suspected human cases of H7N7 were reported between January and August 2021. |