Government Update on the Infected Blood Compensation Scheme (HTML)
Updated 26 November 2025

© Crown copyright 2025
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/infected-blood-compensation-scheme/government-update-on-the-infected-blood-compensation-scheme-html
This page was updated on 30 October 2025 to reflect changes to be made by the Infected Blood Compensation Scheme (Amendment) Regulations 2025, which were laid in draft on 30 October 2025 in Parliament.
These regulations, which amend the March 2025 regulations, implement a number of recommendations in the Inquiry’s Additional Report and make a small number of other changes to improve the administration of the Scheme, or clarify the policy intent.
Now these regulations have been laid, they will be debated in the Houses of Parliament and, subject to approval, will become law by the end of 2025.
Related content
There are additional sources of information about the Infected Blood Compensation Scheme that may be helpful to review alongside this document:
- The Infected Blood Compensation Authority (IBCA) webpage, which will be updated with the latest information about the compensation scheme and the process for applying.
- IBCA’s contact information includes instructions on how to sign up for email updates.
- More information about interim compensation payments.
Introduction
The Infected Blood Scandal is an injustice that has spanned decades on an unprecedented scale: thousands have died, and sadly continue to die every week. Lives have been shattered, and justice denied.
No amount of money can make up for this suffering; however, the Government hopes the Infected Blood Compensation Scheme - referred to throughout this document as ‘the Scheme’ - will bring redress to people who have been impacted by this harrowing scandal.
The Scheme responds directly to and is in line with the recommendations made by the Infected Blood Inquiry, chaired by Sir Brian Langstaff. The Scheme design has also been informed by recommendations made by Sir Robert Francis KC and by the advice of the Infected Blood Inquiry Response Expert Group.
In August 2024, the Scheme was established in regulations. These regulations gave the Infected Blood Compensation Authority (IBCA) the powers to start making ‘core’ compensation payments to infected people, both living and deceased and to pay compensation for infected people registered with an Infected Blood Support Scheme (IBSS). However, the regulations did not give IBCA the powers it needed to pay all eligible people through every available compensation route.
The Infected Blood Compensation Scheme was established in full by the regulations that came into force on 31 March 2025. The additions and changes that made through these regulations include:
- Expanding the eligibility of the Scheme to include people who are affected;
- Introducing the supplementary compensation routes;
- Introducing provisions for people to claim multiple awards if they are both infected and affected, or affected multiple times over;
- Introducing provisions for people to return to the Scheme, should their condition worsen as a result of their infection; and
- Setting out in greater detail the health conditions that make someone eligible for the Severe Health Condition award.
The Government has now laid new draft regulations to make changes to the Infected Blood Compensation Scheme. These regulations will amend the March 2025 regulations to implement a number of recommendations in the Inquiry’s Additional Report, including:
- Removal the HIV start date (recommendation 3a).
- Removal of the minimum earnings threshold for a person to claim the exceptional financial loss award (recommendation 4c).
- Changes to the deeming provisions for the severity of Hepatitis C (recommendation 4d)
- Changes to affected estates (recommendation 8b).
- Date of diagnosis for Hepatitis B and C no longer has to be provided when applying for the scheme (recommendation 4e).
A small number of further changes will be implemented to improve the administration of the scheme. This includes:
- Changes to the severe health condition award to ensure that infected persons who developed a secondary psychotic disorder caused by their Hepatitis B or C infection, or by interferon treatment, are eligible for a Severe Health Condition award (regulation 13).
- Clarification of the current regulations is required to ensure end of life care packages are correctly configured for individuals with co-infections (regulation 8).
- Making provision in the regulations relating to the NHS transplant Scheme (regulation 3).
- Changes to bereaved partner payments following the Government commitment to re-opening bereaved partner applications to the IBSS for those bereaved after 1 April 2025 (regulation 11). These changes allow IBCA to pay 100% of the value of the infected individual’s support scheme payment to the bereaved partner for the 12 month period following the date of death of the infected individual. After that point, bereaved partners will receive 75% for life, in line with the entitlement for partners bereaved before 1 April 2025. Bereaved partners are eligible to register with an IBSS if their infected partner had not received compensation from IBCA
- Moving the dates of transfer of Infected Blood Support Scheme (IBSS) Payments from the IBSS to the IBCA to 2027(regulation 10).
- Allowing individuals to switch between their IBSS payments and a core award, and between periodic payments and a lump sum after receiving their compensation (regulation 12).
The regulations will be debated in Parliament and, subject to Parliamentary approval, will be in force by the end of year.
Purpose of this document
This document outlines the Infected Blood Compensation Scheme which will be delivered by the Infected Blood Compensation Authority (IBCA), an independent arm’s length body which was established in May 2024.
This is a summary document which has been created to help people to understand the Scheme. Whether an applicant is eligible for compensation (and what level of compensation they are eligible to receive) will be dependent on IBCA’s assessment of their circumstances. This assessment will always be based on the regulations for the Scheme.
This summary document replaces a previous explainer document published at the time the first regulations establishing the Scheme were laid in August 2024. This version has been updated throughout so that it reflects the additions and changes made to the Scheme as a result of the 2025 regulations and the draft amendment regulations laid in October. This explainer includes more detail on what different elements of the Scheme will look like (including the supplementary route and changes from the Inquiry’s Additional report). The summaries that explain how the Scheme will work for different groups of eligible people. The case studies created to support the understanding of the March 2025 regulations are still available. IBCA have created a compensation calculator which can estimate your claim.
Below are summaries of the Scheme as it will work for different groups of applicants, these should be read alongside this summary document:
Note on language
The Government recognises the individuality of the experiences of all those impacted by infected blood and does not intend to trivialise the hardship suffered by people across the UK through the language and terminology used in this document and other related guidance.
This document uses the term ‘victim(s)’ to refer collectively to anyone directly or indirectly impacted by infected blood who is eligible for compensation. In line with the language most commonly used throughout the Inquiry, the document refers to people infected with HIV, Hepatitis C and/or Hepatitis B as an ‘infected person’, and the associated family members and others who provided care for a person with an infection as an ‘affected person’.
Glossary of terms
This ‘explainer’ document sets out how the compensation scheme as a whole will work. This means it is long and uses some new or complicated terminology. To assist people in understanding the document and what it means for their own compensation award, the following ‘glossary of terms’ sets out what some common terms mean, in the context of the Scheme.
| Term | Definition |
|---|---|
| Applicant | A person who makes a formal application for compensation through the Infected Blood Compensation Scheme. |
| Bereaved affected dependent | A person who was financially dependent on an infected relative who is now deceased. |
| Bereaved partner | The partner of an infected person who has passed away as a result of infected blood related infections. |
| Carer | A person who provided extensive personal care or support for an infected person without receiving remuneration or reward for a period of at least 6 months, 16.5 hours a week. |
| Child | A person under the age of 18 who is either (directly/indirectly) infected or affected. |
| Child of infected people | A person, irrespective of age, who was cared for and lived with an infected parent. |
| Co-infection | Having more than one of the named infections, e.g. HIV and hepatitis C. |
| Core route | The main route through which all applicants are initially processed when entered onto the Scheme. It uses a tariff-based approach to calculate the amount of compensation payable to those eligible and has five categories of award in total. Eligibility for these categories will depend on whether an applicant is an infected or affected person. |
| Eligible Affected person | A person who is eligible for compensation under the Infected Blood Compensation Scheme because of their relationship to an eligible infected person (e.g. siblings, parents, children). The infected person may be alive or deceased. |
| Eligible Infected person | A person who is eligible for compensation under the Infected Blood Compensation Scheme because they were directly or indirectly infected with HIV and/or hepatitis B, hepatitis C, through the transmission of NHS-supplied blood, blood products or tissue. |
| Estate | A personal representative who makes a claim for compensation on behalf of a deceased infected person. |
| Exceptional Loss awards | The third category of awards available through the supplementary route, which compensates those who had higher costs than they were awarded by the core route. Formerly referred to as the ‘evidence-led sub-route’. |
| Healthy life expectancy | This refers to life expectancy where an infected person had not been infected. It is based on the Ogden Tables (a set of statistical methods used to calculate compensation for personal injury and fatal accidents in the UK). |
| IBCA | Infected Blood Compensation Authority. |
| IBCS | Infected Blood Compensation Scheme, also referred to in this document as ‘the Scheme’. |
| IBSS | Infected Blood Support Scheme. |
| Interim payments | Interim payments were in place whilst the Infected Blood Compensation Scheme was being established, and were made to infected people and bereaved partners who are registered with the Infected Blood Support Scheme. In October 2024, applications opened for interim payments to the estates of deceased infected persons, who were registered with an Infected Blood Support Scheme or Alliance House Organisation. On 21 July 2025, the Minister for the Cabinet Office announced a further interim payment of £210,000 to eligible estates, which means the total interim payment available totals £310,000. |
| Monoinfection | Having one of the named infections, e.g. Hepatitis B. |
| Non-Acute Hepatitis Infections | Clinically referred to as a long term ‘chronic’ hepatitis infection. For the purposes of the Infected Blood Compensation Scheme this means someone with an infection which is at severity level of either chronic, cirrhosis, decompensated cirrhosis, and/or liver cancer and/or liver transplantation. |
| Severe Health Condition awards | The second category of awards available through the supplementary route, which compensates those with specified severe health conditions caused by their infection. Formerly referred to as the ‘health impact subroute’. |
| Supplementary route | An additional route for exceptional cases where applicants must demonstrate that their circumstances necessitate a higher compensation payment than provided through the core route for autonomy, care and/or financial loss. This route requires more detailed evidence but any assessment made through this route will not delay a compensation offer made through the core route. |
| Tariff | All awards available through the core route of the Scheme are tariff based. Awards are determined based on the circumstances of an applicant, either by referencing a fixed number or calculated using a formula. The amounts and formulae are all set out in the relevant regulations. |
| The Scheme | The Infected Blood Compensation Scheme, also referred to in this document as ‘IBCS’. |
| Autonomy award for victims of unethical research | The first category of award available under the supplementary route, which compensates the victims who were subjected to unethical research practices. This award is only available for infected people that have already been accepted onto the Scheme under the core route. |
Infected Blood Compensation Scheme: Overview
The Scheme is a government-funded scheme designed to provide financial compensation to victims of infected blood in the UK:
- The Scheme will be open to both infected and affected people.
- The Scheme will be UK-wide, operated by an independent arm’s length body called the Infected Blood Compensation Authority (IBCA), led by Sir Robert Francis KC as interim Chair.
- Infected people registered with existing Infected Blood Support Schemes (IBSS) on or before 31 March 2025 will continue to receive regular support payments for life, if they wish. Bereaved partners of registered infected persons who passed away after 31 March 2025 may be eligible to register with an IBSS, if their infected partner had not received compensation from IBCA. Any support payments paid from 1 April 2025 will be taken into account when IBCA calculates the amount of compensation that a person is entitled to for the awards relating to their future financial loss and care costs.
- For the majority of applicants, tariffs will be used to calculate compensation. In defined circumstances, which are set out in this document, a further assessment of an applicant’s needs by IBCA under the supplementary route will help to ensure the appropriate compensation is awarded.
- Compensation tariffs for the Scheme have been informed, but not limited, by current practice in UK courts and tribunals.
- Interim compensation payments will be automatically deducted from the compensation awards made through the Scheme.
- For people diagnosed with an eligible infection before 1 April 2025, the Scheme will remain open to applications until 31 March 2031. For people diagnosed after 1 April 2025, the Scheme will remain open to applications for 6 years from the person’s date of diagnosis.
- Accepting compensation through the Scheme will not remove any right a person has to pursue a claim in court.
- Compensation payments made to infected and affected people through the Scheme will not impact their eligibility for means tested benefits.
- All compensation payments made through the Scheme will be exempt from income, capital gains and inheritance tax.
- IBCA began to make payments to infected people at the end of 2024, and the Government expects IBCA to begin payments to affected people in 2025.
Scheme design
The Scheme is based on the recommendations and principles put forward by the Infected Blood Inquiry (referred to throughout the document as ‘the Inquiry’). In line with these, the Government has sought to design a fair and comprehensive compensation scheme that will be quick and simple for eligible applicants to access. The Government’s priority is for compensation to be delivered as swiftly as possible and with the minimum possible delay.
The Scheme’s detailed design reflects the advice of the Infected Blood Inquiry Response Expert Group (referred to throughout this document as ‘Expert Group’), chaired by Professor Sir Jonathan Montgomery. The Expert Group brought together legal and clinical experts who were assisted by social care and actuarial specialists. The Expert Group’s Final Report was published in August. Since August 2024, the Expert Group has continued to advise on issues arising in engagement with the infected blood community and as the second regulations are drafted. An addendum report covering the matters on which the Group has provided advice since August 2024 has also been published. In September 2025, the Minister for the Cabinet Office established an Infected Blood Inquiry Response Technical Expert Group. The Technical Expert Group is assisting the Government in developing proposals, in response to the Inquiry’s Additional Report, for public consultation. Following that consultation, the Government will be in a position to finalise any changes to the Infected Blood Compensation Scheme, informed by the consultation findings and the Technical Expert Group’s advice.
The Scheme has also been informed by feedback from representatives of the infected blood community who, through engagement sessions with Sir Robert Francis KC and David Foley (Interim Chief Executive of the Infected Blood Compensation Authority) in June 2024, generously shared their views on the proposed compensation scheme design published by the previous Government.
Following these engagement sessions, the Minister for the Cabinet Office has continued to meet representatives of the infected blood community to hear their views and act on their feedback. Throughout the process of drafting the 2025 regulations, the Government gave careful consideration to the points raised in engagements, and reflected on the policy before drafting it in the regulations. This included extending the eligibility criteria of siblings under the Scheme to ensure fair compensation to those who have been devastatingly impacted as a result of their sibling’s infection.
The Government undertook engagement with key representative groups of the infected blood community in December 2024 on the unethical research practices award. A fact sheet outlining the policy proposals on these awards was shared and the Government requested written feedback from the selected groups on the proposed eligibility criteria for the award, which requires applicants to demonstrate they were treated at certain Haemophilia centres during the time period in which the Inquiry found that unethical research took place. Each submission was considered with careful attention, and each piece of evidence was reviewed in line with the Inquiry’s report to ensure all updates to the scope of the award made as a result of the engagement process were well founded in evidence found in the Infected Blood Inquiry (IBI). This is in line with Sir Robert’s recommendation following his own engagement with the community last summer.
As a result of the feedback received through this exercise, using evidence from the Infected Blood Inquiry Report, the scope of the award has been extended and more centres have been added to the eligibility criteria. These changes were then communicated to the community through official-led engagement and further meetings with the Minister for the Cabinet Office in January 2025.
The Inquiry held further hearings on the 7 and 8 May 2025 about the timeliness and adequacy of the Government’s response to compensation. On 9 July 2025, the Inquiry published its Additional Report on Compensation. The Inquiry made recommendations to the Cabinet Office and IBCA. The Government Response to the Additional Report was published on 21 July 2025.
The Government is grateful to the wide range of people whose experience and expertise have supported the design of this Scheme.
Applications to the Scheme
IBCA began making payments to infected people in 2024, and payments to affected people are expected to begin in 2025. IBCA is now working to expand the service to all cohorts by the end of 2025.
On 9 October, IBCA launched its registration service, for those seeking to make a claim. Further information is available on IBCA’s website on how to register.
Further updates on the delivery of the compensation Scheme can be found on IBCA’s website. You can sign up for email updates from IBCA.
Eligibility
The Scheme will recognise and provide financial compensation to victims of infected blood, both people who have been infected and those who are affected.
The Scheme has been designed to minimise, as far as possible, the burden on those applying. People registered on a current UK Infected Blood Support Scheme (IBSS) and those who were in receipt of support payments from one or more of the Alliance House Organisations (AHO)[footnote 1] will automatically be considered eligible for the Scheme. Beneficiaries of IBSS or AHO schemes may be required to provide some additional information in order for IBCA to determine their compensation award. IBSS beneficiaries will continue to receive support payments for life unless they choose an alternative payment option - see section Infected Blood Support Scheme (IBSS) payments for further detail.
Descriptions of the groups of people eligible for compensation through the Scheme are provided below.
Infected people
Infected people are those directly and indirectly infected, as summarised in the table below.
A directly infected person includes someone who through the use of NHS-supplied blood, blood products and/or tissue:
- is/was infected with HIV;
- is/was infected with an acute or chronic case of Hepatitis C;
- is/was infected with a chronic case of Hepatitis B;
- was infected with an acute case of Hepatitis B and died as a result of the Hepatitis B infection during the acute period, including reactivation of Hepatitis B infection leading to acute liver failure and death within 12 months.
An indirectly infected person includes someone who was infected:
- by transmission of infection, in defined circumstances, from a person who is or was directly infected (e.g. a person infected by their partner);
- by transmission of infection, in defined circumstances, from a person who was infected by someone who was directly infected (e.g. a child infected by their mother who was infected by her partner).
Where a person who was previously either directly or indirectly infected (as described above) has since recovered or their infection has cleared, they will still be eligible to apply for compensation through the Scheme.
Infected organs transplant Scheme
Individuals who have knowingly agreed to receive a transplant of an organ which is infected through the NHS transplant Scheme would not be able to claim compensation for that infection. Entitlement to compensation from any previous infection would not be affected. If the individual contracted another infection from the same transplant that they were not expecting, they would also still be eligible for compensation for that infection under the Scheme.
The Scheme will not have hard cut-off dates for determining whether a person is eligible for compensation based on when their infection was acquired. However, the evidence requirements will be higher where a person was infected after the introduction of screening of blood, blood products and tissue (see dates below). IBCA will provide detail on evidence requirements in due course.
The dates the Scheme will acknowledge for the introduction of screening are:
i. HIV infection - November 1985;
ii. Hepatitis C infection - September 1991;
iii. Hepatitis B infection - December 1972.
Affected people
Affected people are those who have suffered the impacts of infected blood through their relationship with an infected person (described above), as summarised in the tables below.
An affected person’s eligibility will be dependent on an infected person being identified as eligible for the Scheme. Once this has been confirmed, each eligible affected person can make their own claim for compensation. This is regardless of how many other eligible affected people come forward to claim.
Partners of eligible infected people. This includes:
- spouses;
- civil partners;
- partners cohabiting with an eligible infected person for at least one year following infection.
Where an eligible infected person has had more than one partner during the course of their infection, all partners who meet the above definition will be eligible for compensation in their own right.
Partners who separated from the eligible infected person prior to infection will not be eligible for compensation.
Parents of an eligible infected person, including:
- biological parents;
- adoptive parents;
- others acting in the capacity of a parent as described below (e.g. step parents, grandparents);
who
cared for and lived with an eligible infected person whilst that person was under the age of 18. The provision of care and accommodation must have continued or been expected to continue for a period of at least one year.
The age at which the child became infected does not affect a person’s eligibility. However, compensation rates will be higher for the parents of an infected person where the onset of infection began before the child turned 18 (and the parents cared for and lived with the infected child for at least one year) than for parents whose child was infected as an adult.
Children of an eligible infected person, including:
- biological children;
- adoptive children;
- others in the position of a child as described below (e.g. step children);
who
whilst under the age of 18, were cared for and lived with (for a period of at least one year) a parent who was, or later became, infected.
The age of a child at the time of a parent’s infection will not affect their eligibility but compensation rates will be higher for children who, whilst under the age of 18, lived with and were cared for by an infected parent (for at least one year), than for people whose parents were infected when they were in adulthood.
Siblings of eligible infected people, including:
- biological and adoptive siblings;
- step siblings;
- others in the position of a sibling as described below;
who
while under the age of 18, lived in the same household as an infected person for a period of at least 2 years (regardless of whether the infection occurred during this period), or who would have expected to have done so but for the infection.
Social Impact awards will be higher for siblings who, whilst under the age of 18, lived in the same household as an infected person for a period of at least 2 years after the onset of the infection, or would have been expected to live in the same household were it not for the impact of the infection.
Siblings who did not live in the same household as an infected person for a period of at least two years whilst under the age of 18 may be eligible for compensation as a carer (see eligibility definition below).
Carers of eligible infected people:
Carers of an eligible infected person (e.g. friends or family) who, without reward or remuneration, provided personal care or support greater than would otherwise reasonably have been expected. Such carers will be eligible for compensation in their own right where the provision of care averaged at least 16.5 hours of care per week over a time period of at least 6 months, after the infection.
Estate applications
Where a person who would have been eligible to apply to the Scheme as an infected person has died, the personal representatives of the deceased person’s estate may apply for compensation on behalf of the estate of the deceased infected person.
Following the recommendation made in the Inquiry’s Additional Report, the estates of affected individuals who would have been eligible for compensation but died before receiving it can apply to the Scheme. This applies specifically to affected individuals who passed away between May 21, 2024, and March 31, 2031.
Applications on behalf of a child or person who lacks capacity
Where an application relates to a child, it must be made by a person who has parental responsibility for them.Where an application is made in respect of someone who lacks mental capacity, the application must be made by an authorised representative.
Multiple claims
Some people eligible to receive compensation through the Scheme may have been affected by their relationship with multiple infected people. Other people may have themselves been infected and also affected by the infection of a loved one. This will be recognised in the compensation available. Further detail can be seen in the section Compensation awards where an applicant has multiple claims.
Compensation assessment
Compensation paid through the Scheme will be calculated in line with tariffs and based on the severity of infection and negative impacts suffered by victims in different aspects of their lives (see section Categories of Award).
For IBSS beneficiaries, further detail on how the continuation of support payments will be taken into account in calculating compensation awarded through the Scheme can be seen in the section Infected Blood Support Scheme (IBSS) payments.
The level of compensation offered to victims of infected blood through the Scheme is informed, but not limited, by current practice in UK courts.
Tariff-based approach
The Government has accepted the Infected Blood Inquiry’s recommended categories of award. The Government has also accepted the Inquiry’s recommendation that the scheme should be based on a tariff-based compensation framework for infected and affected people. The Scheme will use a tariff-based framework to calculate the amount of compensation payable to those eligible.
In practice, this means that compensation will be calculated based on set criteria and rates. Using a tariff approach will minimise the amount of information that people applying to the Scheme are required to provide. It will also help to ensure that compensation can be awarded more quickly than would otherwise be possible if all applications for compensation had to be individually assessed.
Core and Supplementary Routes
The Scheme will offer a core route and a supplementary route for awarding compensation. These routes will be different depending on whether someone is an infected or affected person.
Once accepted onto the Scheme, all eligible applicants will initially be offered a compensation package through the core route. The design of the tariffs means that the core route is expected to be suitable for the majority of applicants, with no further assessment of personal circumstances required.
In some exceptional cases, the level of compensation awarded through the core route may not be sufficiently reflective of the financial loss and care costs that an infected person has experienced as a result of their infection. This may be the case where, for example, an infected person had particularly high earnings prior to their infection and therefore suffered greater financial loss, or where they have suffered a particular associated health condition that meant they needed more care. For an affected person, a supplementary claim can be made if their financial loss was greater than the core route assumes based on their relationship to the infected person. For example, the core route does not assume that a parent would be financially dependent on their child.
Where an applicant can demonstrate that their defined circumstances mean that they need a higher compensation payment for care and financial loss in order to reflect the impact of the infection on their life, they will have the opportunity to apply for additional compensation awards through the supplementary route. Further detail can be found in the section Additional awards available through the Supplementary Route. For infected people, an offer will have to be made and accepted under the core route before an applicant can be assessed under the supplementary route. However, any assessment under the supplementary route will not delay the compensation offer made through the core route, nor will it affect the amount of compensation someone is eligible for through the core route.
The Government has published its response to the Inquiry’s Additional Report on compensation. This response outlines the areas in which the government will consult on. Further legislation will then be required to implement the outcome of the consultation.
Categories of Award
Under the Scheme, compensation will be calculated in line with the Categories of Award outlined in the table below. Each Category of Award recognises and compensates for the impacts of the infected blood scandal in different areas of a person’s life.
| Category of Award | Description |
|---|---|
| Injury award | This award recognises the physical and mental injury, emotional distress and injury to feelings that may have been caused or will in future be felt as a result of: infected blood and/or related medical treatments; the death of an infected person; the likely death of a loved one in the future. |
| Social Impact award | This award recognises the past and future social consequences that people with blood-borne infections may have suffered (e.g. stigma and social isolation). |
| Autonomy award | This award recognises the distress and suffering caused by the impact of disease, including interference with family and private life (e.g. loss of marriage or partnership, loss of opportunity to have children). |
| Care award | This award recognises the past and future care needs and associated costs for infected people. |
| Financial Loss award | This award recognises the past and future financial losses suffered as a result of infection. This includes both financial loss and loss of services (e.g. providing childcare). |
Infection Severity Banding
In line with the Infected Blood Inquiry’s recommendation, the Scheme will take into account the severity of infection suffered in calculating compensation. Where a person has suffered the impact of co-infection (e.g. they were infected with both HIV and Hepatitis C), this will also be reflected in the compensation awarded to them.
Where a person is automatically considered eligible for the Scheme as a beneficiary of an IBSS or AHO scheme, they may be required to provide some additional information in order for IBCA to determine their Infection Severity Band.
The Infection Severity Bands for the Scheme are outlined in the table below. The Infection Severity Bands have been designed in line with clinical diagnostic markers (i.e. recognised health conditions, for example, liver damage). This means that in most cases, an applicant’s Infection Severity Band at the time of their application should be easily identifiable from their medical notes.
| Infection Severity Bands | Notes on Severity Band definitions |
|---|---|
| Hepatitis B - Acute, where the infection resulted in a fatality in the acute period | Infection resulting in acute liver failure within 12 months of infection; Reactivation of Hepatitis B infection leading to acute liver failure and death within 12 months. |
| Hepatitis C - Acute | Transient, self-cleared infection usually within 6-12 months of exposure. |
| Hepatitis C or Hepatitis B - Chronic | Chronic infection characterised by: (a) Hepatitis B - infection with confirmed Hepatitis B surface antigen (HBsAg) positivity for longer than 6 months with detectable Hepatitis B virus DNA on a polymerase chain reaction test, if not on antiviral therapy. (b) Hepatitis C - infection with replicating Hepatitis C virus RNA. |
| Hepatitis C or Hepatitis B - Cirrhosis (liver damage) | Characterised by serious fibrosis scarring of the liver caused by long-term liver damage caused by infection; Treatment of B-cell non-Hodgkin’s lymphoma caused by infection - single round treatment (first line therapy); Type 2 or 3 cryoglobulinaemia caused by infection accompanied by membranoproliferative glomerulonephritis (MPGN). |
| Hepatitis C or Hepatitis B - Decompensated cirrhosis and/or liver cancer and/or liver transplantation | Decompensated cirrhosis caused by infection is characterised by the presence of: hepatic encephalopathy (confusion due to liver damage); ascites (accumulation of fluid in the abdomen); variceal haemorrhage (bleeding from dilated veins in the gullet or stomach); or, a Child-Pugh score greater than 7. Treatment of B-cell non-Hodgkin’s lymphoma caused by infection - multiple round treatment (second line therapy). |
| HIV | Single severity banding. |
| Co-infection of HIV and Hepatitis C or Hepatitis B | Co-infection severity bands will reflect the severity of the Hepatitis infection as described above and the HIV infection. |
Calculating compensation awards
This section provides detail on how compensation awards are calculated under the Scheme.
Calculating compensation for infected people and their estates
The table below sets out how compensation in each Category of Award is calculated for eligible infected people and their estates.
| Category of Award | Method of calculation | Supplementary awards available |
|---|---|---|
| Injury award | Fixed financial award determined by a person’s Infection Severity Band. This means that where a person has suffered an infection with a more significant medical impact, their Injury award will be higher. Higher Injury awards will also reflect where a person has suffered a co-infection (i.e. more than one infection). |
None |
| Social Impact award | Fixed financial award based on whether a person has suffered a monoinfection (i.e. one infection only) or a co-infection (i.e. more than one infection). The tariff rate does not vary with infection severity where a person’s infection was chronic (i.e. not acute). This recognises that regardless of a person’s infection, members of the public may have made assumptions that resulted in an infected person suffering stigma and/or isolation. A person with a co-infection will receive a higher tariff than a person having suffered a monoinfection. |
None |
| Autonomy award | Fixed financial award determined by a person’s Infection Severity Band. This means that where a person has suffered an infection with a more significant medical impact, their Autonomy award will be higher to reflect the increased interference with their family and private life. |
An uplift to the Autonomy award will be available for victims of unethical research practices. See section The Supplementary Route for Infected People for further detail. |
| Care award | Calculated based on a typical pattern of care needs[footnote 2] after infection and commercial care costs associated with the Infection Severity Band of a person’s infection. A single UK-wide rate is used to calculate the Care award. This means that the rate will not change based on where in the UK the person has or will in future receive care. Awards for acute infections are lower than awards for non acute infections which are likely to have required ongoing care. An infected person can choose for Care awards to be paid directly to affected people. |
Higher Care awards will be available where applicants can demonstrate higher care costs or care requirements than those assumed by the tariff. See section The Supplementary Route for Infected People for further detail. |
| Financial Loss award HIV and Hepatitis B/C (Chronic/ Cirrhosis/Decompensated cirrhosis and/or liver cancer and/or liver transplantation) infections |
Calculated based on the average anticipated loss of earnings suffered by an infected person as a result of their infection and subsequent treatment. Financial Loss award calculations take into account a person’s average loss of earnings in the years prior to the establishment of the Scheme, as well as future loss of earnings up to healthy life expectancy.[footnote 3] Financial Loss awards are based on net median UK earnings[footnote 4] + 5%, which amounts to £29,657 per annum prior to retirement age[footnote 5]. Financial loss from the age of 66 onwards is based on 50% of the financial award prior to that age to reflect a pension payout. For simplicity, all financial loss, whether past or future, is calculated using these average rates, rather than historic averages. The following assumptions have been made in calculating financial loss for living infected people: - For Hepatitis C - it is assumed that the introduction of effective treatments in 2016 improved an infected person’s ability to effectively manage their infection from 2017, and therefore their ability to work. These assumptions are not applied if an infected person was born before 1961. This is because the infected person will have been 55 years or older when effective treatment was introduced and may, therefore, have been less likely to be able to return to employment or increase their hours as their health improved. - For Hepatitis B - it is assumed that the introduction of effective treatments in 2008 improved an infected person’s ability to effectively manage their infection from 2009 and therefore their ability to work. These assumptions are not applied if an infected person was born before 1953. This is because the infected person will have been 55 years or older when effective treatment was introduced and may, therefore, have been less likely to be able to return to employment or increase their hours as their health improved. - For Hepatitis C and Hepatitis B co-infections - it is assumed that the introduction of effective treatments in 2016 improved an infected person’s ability to manage their infection from 2017, and therefore their ability to work. These assumptions are not applied if an infected person was born before 1961. This is because the infected person will have been 55 years or older when effective treatment was introduced and may, therefore, have been less likely to be able to return to employment or increase their hours as their health improved. - For HIV and HIV and Hepatitis co-infections - it is assumed that people will initially have lived without symptoms for a period of time following HIV infection before suffering an impact on their earning potential after the onset of symptoms. Given that it is not always easy to identify the timing of the onset of symptoms, financial loss compensation will be paid from the date of infection, with an increased rate following diagnosis. In addition to anticipated loss of earnings, a flat rate of £12,500 will be paid to all infected people (or their estate) to cover miscellaneous expenses including travel to appointments, extra cost of insurance etc. |
Higher Financial Loss awards will be available where applicants can demonstrate that they would have earned more than is assumed by the tariff, or were able to work less than is assumed by the tariff. See section The Supplementary Route for Infected People for further detail. |
| Financial Loss award (Acute Hepatitis B/C infections) |
Flat rate awards for Financial Loss are as follows: - Acute Hepatitis C infection: £12,500 - Acute Hepatitis B infection (where the person died of the infection in the acute period including the reactivation of Hepatitis B infection leading to acute liver failure and death within 12 months): £17,500 Both flat rate awards for this cohort of people include compensation to cover other miscellaneous costs incurred as a result of infection (e.g. increased insurance, additional transport). |
Higher Financial Loss awards are available where applicants can demonstrate that they would have earned more than is assumed by the tariff, or were able to work less than is assumed by the tariff. See section Additional awards available through the Supplementary Route for further detail. |
Paying Financial Loss awards
Where an infected person is living, the Financial Loss award is paid to the infected person directly.
Where an infected person is deceased:
- the award for past financial loss (i.e. from the point of infection to death) will be paid to the estate of the infected person;
- the award for future financial loss (i.e. years between death and healthy life expectancy age) will be paid to any affected people (as defined by the Scheme) who are dependents of that infected person (i.e. bereaved partner or children under 18).
Paying Care awards
Care awards are made to an infected person. An infected person can choose for some or all of their Care award to be paid directly to eligible affected people who provided them care.
Calculating compensation for affected people
The table below sets out how compensation in each Category of Award is calculated for eligible affected people.
| Category of Award | Method of calculation | Who is eligible? |
|---|---|---|
| Injury award | Fixed financial award determined by the affected person’s relationship to the infected person and the infection severity suffered by the infected person. Injury awards will be higher where the severity of a person’s infection means that the infection has caused or is expected to cause an early death in the future (i.e. HIV, Hepatitis B/C cirrhosis, Hepatitis B/C decompensated cirrhosis or liver cancer). |
All affected people |
| Social Impact award | Fixed financial award determined by the affected person’s relationship to the infected person. Social Impact awards are higher for affected people assumed to have lived with the infected person for at least 2 years after the onset of infection. Namely partners, children under 18, parents of infected children under 18 and some siblings. |
All affected people |
| Autonomy award | Fixed financial award determined by the affected person’s relationship to the infected person. | Autonomy awards are available for affected people who are likely to have experienced the most significant impact on their private lives and autonomy. This includes affected partners, parents and children only. Siblings and carers are not eligible for Autonomy awards. |
| Care award | Not available for affected people in their own right. | Care awards paid to infected people can be paid directly to affected people on the request of an infected person. |
| Financial Loss award | Financial Loss awards are only paid to affected people where the infected person has died. Where an infected person is deceased, financial loss from the point of death to the estimated healthy life expectancy age of the deceased is paid to the affected dependents (bereaved partners and children who were under 18 at the time of death) registered with the Scheme. Financial Loss awards to bereaved affected dependants, in defined circumstances, are as follows: - Partner of an infected person at time of death: £16,682 per annum until the healthy life expectancy of the deceased infected person. (£8,341 for years where the infected person would have been 66 or older). - Child under 18 at the time of the infected person’s death: £5,561 per annum, until the age of 18. (£2,780.50 for years where the infected person would have been 66 or older). - Child under 18 who has lost both parents to infected blood related infections: £22,243 per annum, until the age of 18. (£16,682.25 for years where one parent would have been 66 or older; £11,121.50 for years where both parents would have been 66 or older). There is no limit to the number of eligible bereaved affected people who can claim the Financial Loss awards. |
Bereaved partners and children Other bereaved affected people (disabled children over the age of 18, parents and siblings of infected people) will be eligible to receive Financial Loss awards if they are able to provide evidence of dependency on the infected person at the time of death and for at least six months prior to this point. See section Additional awards available through the Supplementary Route for further detail. |
Compensation awards where an applicant has multiple claims
There are some instances where a person may be eligible to make multiple claims for compensation. One example of this is where they have multiple loved ones who have been infected (for example, where a parent and a sibling have been infected). This means they are affected multiple times. In this case, IBCA will review all the claims at once and provide a single, comprehensive compensation award.
For example, an affected applicant who has three loved ones who have been infected, might make three claims for compensation at the same time. Under the Core Route, there are five categories of awards that applicants can receive compensation for. In the above example, an applicant would be entitled to multiple ‘Injury’ awards. However, for the ‘Social Impact’ and ‘Autonomy’ awards, they will only receive one of each award regardless of the overall number of claims they are entitled to. They may be entitled to further ‘Financial Loss’ awards depending on their circumstances. In summary, applicants eligible to make multiple compensation claims may be awarded several ‘Injury’ and ‘Financial Loss’ awards, but will only ever receive one ‘Social Impact’ and ‘Autonomy’ award. This is shown in the diagram below.
For an applicant who has multiple claims as an affected person
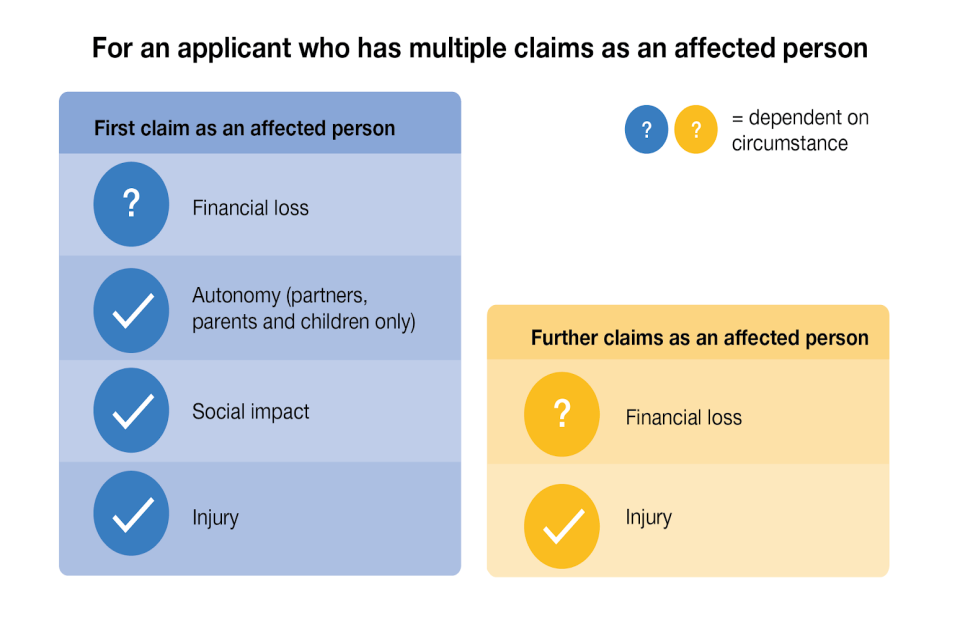
Image description:
Primary award (affected person)
- Financial loss (dependent on circumstances)
- Autonomy (partners, parents and children only)
- Social Impact
- Injury
Further claims as an affected person
- Financial loss (dependent on circumstances)
- Injury
A person may also be eligible to make multiple claims for compensation if they are both an infected and an affected person (for example, where the person is infected themselves and a family member has also been infected). In this case, IBCA will need to review and assess each claim separately as it is made. For example, a couple where both partners are infected might make individual claims for compensation. Once their claims are approved, they will then both be able to make a second claim for compensation as the partner of an infected person (i.e. an affected person). Applicants who this applies to will be entitled to compensation in all categories of award available to infected people, as well as additional ‘Injury’ awards corresponding to the number of affected claims made. Additional ‘Financial Loss’ awards may be available depending on circumstance. This is shown in the diagram below.
For an applicant who is both an infected and affected person
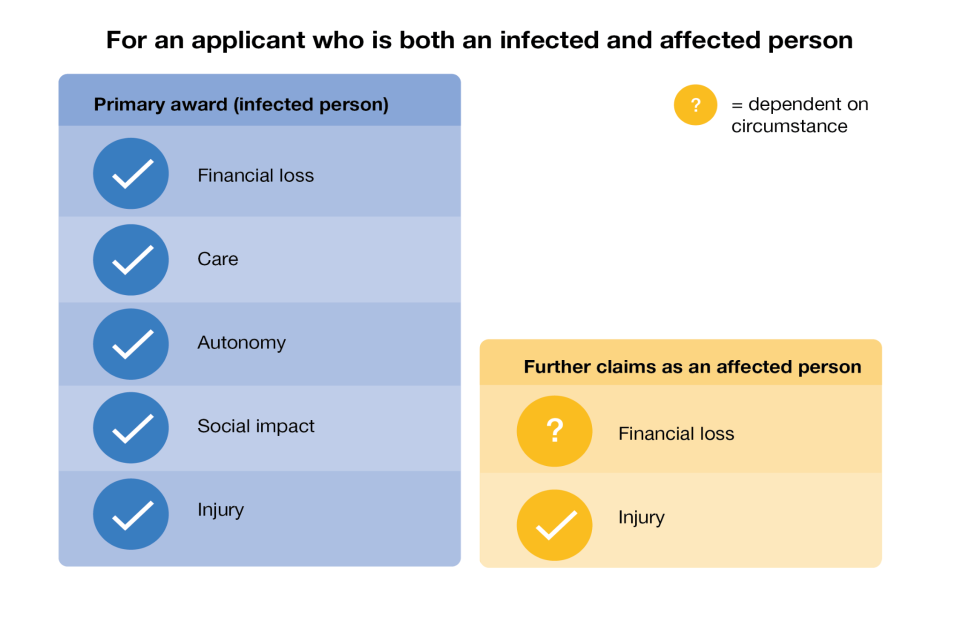
Image description:
Primary award (infected person)
- Financial loss
- Care
- Autonomy
- Social Impact
- Injury
Further claims as an affected person
- Financial loss (dependent on circumstances)
- Injury
The Supplementary Route for Infected People
There are additional awards available for infected people through the supplementary route for some categories of award. An applicant will need to go through their core route assessment before they can apply to the supplementary route. At this point, they will have the opportunity to indicate whether they would like to apply for a supplementary award. Applicants are not required to apply for supplementary route awards if they do not wish to.
Building on the core route, and where applicants can demonstrate eligibility, higher levels of compensation will be available for the ‘Autonomy’, ‘Financial Loss’ and ‘Care’ awards through the supplementary route.
An assessment under the supplementary route will not delay payment of the compensation offer made through the core route. In addition, someone’s core route compensation will never decrease as a result of applying to the supplementary route. However the amount of evidence required from the applicant for the Supplementary route is higher. This means that the assessment IBCA will undertake is likely to take longer than the core route assessment.
Applicants do not need to apply to every part of the supplementary route if they do not want to or they are not eligible. However, if they do want to apply for more than one award through the supplementary route, they will need to follow the order set out in the diagram below. This is because some aspects of the awards build on previous ones (for example, the Exceptional loss awards for financial loss build on the financial loss and care assessments made under the Severe Health Condition award). Supplementary route awards will be paid at the end of the full supplementary route assessment (i.e not after individual awards have been assessed and calculated). Please see the diagram below.
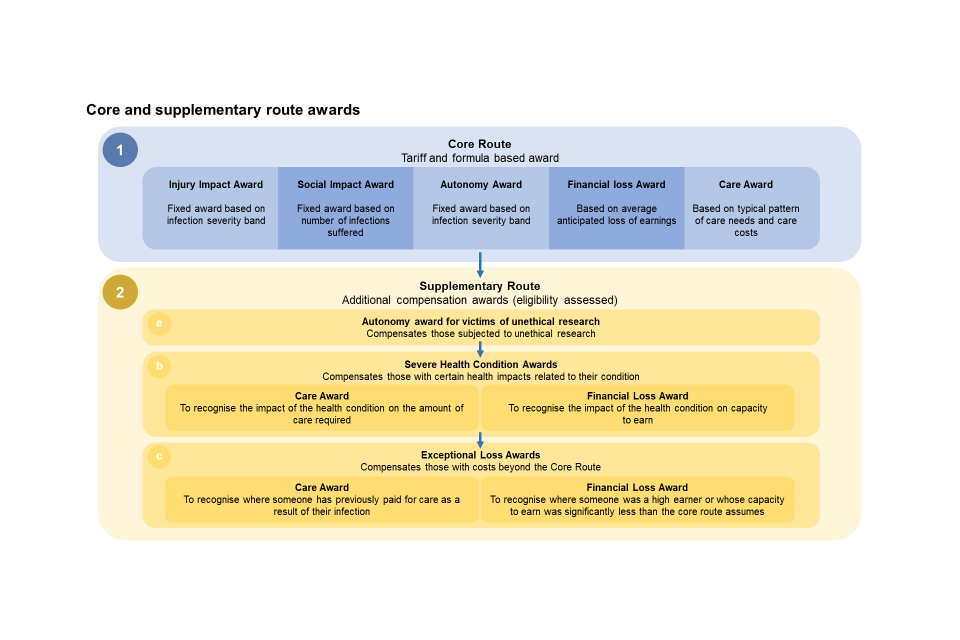
Image description:
1. Core route - Tariff and formula-based award
- Injury award: Fixed award based on infection severity band
- Social Impact Award: Fixed award based on number of infections suffered
- Autonomy Award: Fixed award based on infection severity band
- Financial loss Award: Based on average anticipated loss of earnings
- Care Award: Based on typical pattern of care needs and care costs
2. Supplementary Route - Additional compensation awards (eligibility assessed)
a. Autonomy Award for victims of unethical research: Compensates those subjected to unethical research
b. Severe Health Condition Awards: Compensates those with certain health impacts related to their condition
- Care award: To recognise the impact of the health condition on the amount of care required
- Financial Loss Award: To recognise the impact of the health condition on capacity to earn
c. Exceptional Loss Awards - Compensates those with costs beyond the Core Route
- Care award: To recognise where someone has previously paid for care as a result of their infection
- Financial Loss Award: To recognise where someone was a high earner or whose capacity to earn was significantly less than the core route assumes
Applying for awards through the supplementary route
Further detail on the awards available in these categories is set out below.
Supplementary route: Autonomy award for victims of unethical research
Additional Autonomy awards will be available through the supplementary route to recognise the suffering of victims subjected to unethical research practices. A flat rate award of £10,000 will be available to infected people (or their estates) who were victims of unethical research projects at a treatment centre or a participant in one of Dr Craske’s studies. A separate award of £15,000 will be available to all infected people (or their estates) who attended Lord Mayor Treloar College between 1970 and 1983 inclusive and who can therefore be assumed to have been subject to unethical research while at the College.
If eligible for both unethical research awards, an infected person will receive whichever award is highest (but not both). This means that if an infected person was subjected to research whilst they attended Lord Mayor Treloar College, and was also subjected to another unethical research project, they would therefore receive a single award of £15,000.
Eligibility criteria for the additional Autonomy award is based on research studies referenced by the Infected Blood Inquiry, during the time period where unethical research practices were identified to have taken place.
To claim the additional Autonomy award, an infected person will need to provide evidence to demonstrate that they meet the criteria set out below:
| Meet one of the criteria below | During the following date range |
|---|---|
| Participant in one of Dr Craske’s studies | 1974 - 1984 |
| Treatment at Oxford Haemophilia Centre | 1974 - 1984 |
| Treatment at Edinburgh Haemophilia Centre | 1974 - 1984 |
| Treatment at Newcastle Haemophilia Centre | 1974 - 1984 |
| Treatment at Royal Free Haemophilia Centre | 1974 - 1984 |
| Treatment at Glasgow Haemophilia Centre | 1974 - 1984 |
| Treatment at St Thomas’ Haemophilia Centre | 1974 - 1984 |
| Treatment at Cardiff Haemophilia Centre | 1974 - 1984 |
| Treatment at Manchester Haemophilia Centre | 1974 - 1984 |
| Treatment at Sheffield Haemophilia Centre | 1974 - 1984 |
| Attended Lord Mayor Treloar College | 1970-1983 |
In some of these locations, in addition to the main Haemophilia Centre, there were also separate Haemophilia Centres for children or children’s hospitals that may have treated bleeding disorder patients. Where this is the case, we have carefully reviewed the IBI evidence on research. We found no further evidence of unethical research projects carried out at any other Haemophilia centres or children’s hospitals other than those named above (with the exception of Lord Mayor Treloar College).
The Government has published its response to the Inquiry’s Additional Report on compensation. This response outlines the areas in which the government will consult on. Further legislation will then be required to implement the outcome of the consultation.
Supplementary route: Severe Health Condition award
Eligible infected people who have suffered from a specified rare severe health condition as a result of their infection may apply for additional compensation.
The Core route tariffs already take into account most of the severe health conditions that infected people are likely to experience as a result of their infection. The Severe Health Condition Award will be available to eligible infected people who have suffered from a specified rare severe health condition as a result of their infection, or treatment of their infection, that has not already been taken into account in the core awards.
The list of eligible severe health conditions has been developed following advice from the Infected Blood Inquiry Response Expert Group. The health conditions included are those that have clear clinical markers for which applicants will be able to provide specific evidence.
This means that the Scheme will therefore have different thresholds and eligibility requirements to the Infected Blood Support Schemes for the Severe Health Condition awards. Some impacts currently recognised by the IBSS ‘Special Category Mechanism’ (SCM) will not be recognised by the Severe Health Condition award. This is to make sure that the Severe Health Condition award provides compensation for rare severe health conditions that are not already included as part of someone’s core award compensation.
Eligibility
The core route already assumes that infected people will have experienced significant symptoms as a result of contracting an infection from infected blood, and this is reflected in the award tariffs available. This means that the Severe Health Condition award will be for those who can evidence a rare, severe health condition (hereby known as ‘qualifying Severe Health Conditions’) above and beyond the health conditions accounted for by the core route.
Health conditions relating to HIV, Hepatitis B or Hepatitis C infections that may qualify an applicant for a supplementary Severe Health Condition award are:
- Group One - Severe visual impairment;
- Group Two - Neurological disorders resulting in long-term severe physical or mobility disability;
- Group Three - Neurological disorders resulting in long-term severe neurocognitive impairment;
- Group Four - Severe psychiatric disorders potentially resulting in inpatient psychiatric care;
- Group Five - End-stage kidney disease requiring renal replacement therapy;
- Group Six - Other hepatic disorders[footnote 6] caused by Hepatitis B or Hepatitis C resulting in long-term severe disability.
The Government has published its response to the Inquiry’s Additional Report on compensation. This response outlines the areas in which the government will consult on. Further legislation will then be required to implement the outcome of the consultation.
Severe Health awards and IBSS route payments
The eligibility criteria that the Scheme uses for the Severe Health Condition award will not change the value of regular Support Scheme payments an IBSS beneficiary will continue to receive as part of their compensation package, if that is the option they choose. This will mean that IBSS beneficiaries who currently receive SCM payments (or equivalent IBSS category) will continue to do so without needing to provide further evidence, regardless of Severe Health Condition award eligibility.
Severe Health Condition - Financial Loss award
Under the core route, IBCA calculates an applicant’s financial loss by considering the severity of their infection and from this, assumes the level of financial loss expected for that person each year. For the supplementary route, these assumptions are adjusted once someone has been diagnosed with a qualifying severe health condition. Where someone can evidence a qualifying severe health condition, the amount of expected financial loss per year is adjusted. For groups 2, 3 and 4 (see above) there is an additional requirement that applicants were unable to work for all or part of the year. The applicant must provide evidence for this.
Applicants with HIV will not be eligible to receive any additional Financial Loss awards through the Severe Health Condition award. This is because the core award already assumes that people infected with HIV were unable to return to work after they were infected. This means that they already receive the highest financial loss tariff possible.
Infected people whose severe health condition was diagnosed after retirement age (age 66) will also not be eligible to receive any additional Financial Loss awards through the Severe Health Condition award. This is because the condition is unlikely to have impacted their earning potential, due to the age at which the severe health condition developed.
Below is a table summarising Financial Loss awards for each of the qualifying severe health conditions. Further, comprehensive detail on the qualifying severe health conditions and the compensation available through the supplementary route are provided in Annex C. Higher compensation available through the Severe Health Condition award will be calculated using the financial loss rates and care rates used in the core route.
Severe Health Condition - Care award
Someone’s care requirements may fluctuate across the period of their life when they were infected. Because this is a tariff-based scheme, the core route Care award assumes a standardised lifetime package of care based on the likely care costs for an infection.
However, for someone with a qualifying severe health condition listed above, this award removes this assumption of a standardised lifetime package of care, and replaces it with a care profile that attempts to better reflect the likely care costs of someone suffering from such a severe health condition.
This means someone would be eligible for an additional award when the number of years between diagnosis of a severe health condition and death (or healthy life expectancy for living infected people) is greater than the total number of years of care built into the core award. In simple terms, this means that applicants to the ‘Severe Health Condition Care award’ will receive additional care support if their assumed care needs (due to their severe health condition) are greater than that provided in the standard Care award provided as part of the core route.
Qualifying severe health conditions
| Severe health conditions | Condition | Financial Loss award | Care award modification* |
|---|---|---|---|
| Group 1 Severe visual impairment |
HIV | No additional award. | Domestic support and ad hoc care Equates to 6 hours per week: Support with heavier domestic tasks, attendance of medical appointments and household maintenance. |
| Group 2 Neurological disorders resulting in long-term severe physical or mobility disability Evidence of inability to return to work required. |
HIV | No additional award. | Low care Low care band equates to 16.5 hours per week consisting of 6 hours per week domestic support and 1.5 hours per day personal care. |
| Group 2 Neurological disorders resulting in long-term severe physical or mobility disability Evidence of inability to return to work required. |
Hepatitis | Financial loss for years following diagnosis is adjusted to 100% financial loss. This equates to £29,657 per annum from year of severe health condition diagnosis until age of 66 (retirement age) then the corresponding pension rate. |
Low care Low care band equates to 16.5 hours per week consisting of 6 hours per week domestic support and 1.5 hours per day personal care. |
| Group 3 Neurological disorders resulting in long-term severe neurocognitive impairment Evidence of inability to return to work required. |
HIV | No additional award. | Low care Low care band equates to 16.5 hours per week consisting of 6 hours per week domestic support and 1.5 hours per day personal care. |
| Group 3 Neurological disorders resulting in long-term severe neurocognitive impairment Evidence of inability to return to work required. |
Hepatitis Decompensated cirrhosis | Financial loss for years following diagnosis adjusted to 100% financial loss for years of severe health condition diagnosis beyond 4 years. This equates to £29,657 per annum from year of severe health condition diagnosis until age of 66 (retirement age) then the corresponding pension rate. | Low care Low care band equates to 16.5 hours per week consisting of 6 hours per week domestic support and 1.5 hours per day personal care. |
| Group 4 Severe psychiatric disorder Evidence of inability to return to work required. |
HIV | No additional award. | Domestic support and ad hoc care Equates to 6 hours per week: Support with heavier domestic tasks, attendance of medical appointments and household maintenance. Adjustment to low care upon provision of social services needs assessment confirming requirement for long term personal and domestic care as defined by scheme in the ‘low care’ band. Low care band equates to 16.5 hours per week consisting of 6 hours per week domestic support and 1.5 hours per day personal care. |
| Group 4 Severe psychiatric disorder Evidence of inability to return to work required. |
Hepatitis | Financial loss for years following diagnosis adjusted to 100% financial loss. This equates to £29,657 per annum from year of severe health condition diagnosis until age of 66 (retirement age) then the corresponding pension rate. |
Domestic support and ad hoc care Equates to 6 hours per week: Support with heavier domestic tasks, attendance of medical appointments and household maintenance Adjustment to low care upon provision of social services needs assessment confirming requirement for long term personal and domestic care as defined by scheme in the ‘low care’ band. Low care band equates to 16.5 hours per week consisting of 6 hours per week domestic support and 1.5 hours per day personal care. |
| Group 5 End-stage kidney disease requiring renal replacement therapy (RRT) |
HIV | No additional award. | Domestic support and ad hoc care from diagnosis of condition. |
| Group 5 End-stage kidney disease requiring renal replacement therapy (RRT) |
Hepatitis | Financial loss for years on dialysis adjusted to 100% financial loss. This equates to £29,657 per annum from year of severe health condition diagnosis untill age of 66 (retirement age). |
Domestic support and ad hoc care from diagnosis of condition. |
| Group 6 Other Hepatic disorders resulting in long-term severe disability |
Hepatitis | Living person with a Hepatitis B infection: For those born after 1953: Pre effective treatment (2008 and earlier): 70% financial loss, £20,760 per annum. For those born after 1953: Effective management from 2009: 60% financial loss, £17,794 per annum. For those born in or before 1953: 70% financial loss, £20,760 per annum. Living person with a Hepatitis C infection: For those born in or before 1961: 70% financial loss (£20,760 per annum). For those born after 1961: from diagnosis until 2017: 70% financial loss (£20,760 per annum). For those born after 1961: 2017 onwards: 60% financial loss (£17,794 per annum). Estate of a deceased infected person: Fixed financial loss award of £71,178. |
Living person with an infection Domestic support and ad hoc care Equates to 6 hours per week: Support with heavier domestic tasks, attendance of medical appointments and household maintenance. Estate of a deceased infected person: Up to 10 years additional domestic support and ad hoc care. |
*An applicant’s Severe Health Condition Care award will be dependent on the applicant’s Infection Severity Band and the number of years and type of care already included in the core Care award.
Supplementary route: Exceptional Loss awards (to recognise loss of earnings, and/or paid-for care costs)
Depending on their personal circumstances, we expect that there will be a small number of infected people who suffered greater financial loss or care costs as a result of their infection than the tariff-based compensation available under the core route. Infected people who can provide evidence of greater financial loss and/or care costs as a result of their infection will be able to apply for the Exceptional Loss awards through the Supplementary route.
The people eligible for these awards will be:
- infected people who were particularly high earners prior to infection and suffered a reduced ability to earn because of their infection; and
- infected people who paid more in care costs in the past (before 31 March 2025), or who paid for care during periods where the core route assumed past care was unpaid.
There are four specific Exceptional Loss awards available through the Supplementary route. Two are for different types of financial loss, and two are for different types of care costs:
- Financial Loss (PAYE earnings) award;
- Financial Loss (self-employment earnings) award;
- Care (excess deemed costs) award; and,
- Care (excess actual costs) award
In the 2024 version of this explainer document, these awards were collectively called the ‘Evidence-led supplementary sub-route’. The award names have been changed in this version of the explainer document so that they match the terminology used in the 2025 regulations to describe the different awards available.
Applicants will need to provide evidence of their personal circumstances to apply for these awards. They will need to provide evidence to show that their earning capacity was lower than that assumed by the scheme, or evidence that they paid for their past care. This evidence might be invoices of care costs, evidence of early medical retirement, and/or evidence of earnings. Because this award is to reflect someone’s personal circumstances, IBCA will require applicants to provide more evidence for the supplementary route than for the core route. However, it will still require less evidence than someone would be likely to need to provide if they were trying to claim through the Courts.
Because the Scheme uses tariffs to calculate someone’s compensation, it also means that compensation payments are unaffected by any benefits the applicant might have claimed in the past, or the impact that other non-related health conditions might have had on their life.
Whilst this means that the Scheme will be simple to access, and that people will receive compensation as soon as possible, it also means that the Government needs to make sure there is a limit on the highest level of award that the Scheme can offer someone.
The following Exceptional Loss awards are available:
a. Exceptional Loss awards for financial loss
There are two different awards available to provide additional compensation to infected people who earned substantially more than the assumed annual salary under the Core Financial Loss award and whose capacity to work was significantly reduced. These are the:
- Financial Loss (PAYE earnings) award;
- Financial Loss (self-employment earnings) award.
Applicants will need to provide evidence of their earnings before and after their ability to earn was adversely impacted by their infection, whichever of these awards they apply for. Because these awards look at someone’s individual circumstances, rather than using the earnings assumptions used by the Core and/or Severe Health Condition awards, applicants will have to provide more detailed evidence of their personal earnings and capacity to work.
The awards are based on lost earnings across the entire infection period, not just the years where an infected person’s capacity to earn was impacted. This is to make sure they are an accurate reflection of someone’s lifetime circumstances after they were infected.
This means that infected people who were able to keep working normally for a number of years after they were infected are unlikely to be eligible for an Exceptional Loss award for financial loss. This is because the award builds on the compensation that has already been awarded through the core route. Because the core route uses assumptions about the impact of an infection on someone’s ability to earn, an infected person in this circumstance will already have been given an award for financial loss to cover the years where they might, in fact, have been able to keep working normally. This means that when they provide evidence of their lost earnings, it may turn out that overall, taking into account the core route compensation, they are not actually eligible for any further financial loss award.
If someone is eligible for additional compensation through one of these awards, there will be a cap on the amount they are able to receive. The highest amount they will be able to receive per year is the same as the 90th percentile 2023 UK average salary, which is equivalent to £76,249 pre-tax and national insurance (or £54,028 net of tax and national insurance). The award to applicants with gross salaries above £76,249 per annum will be capped to this maximum.
The Core awards already provide a Financial Loss award from the point of infection. This is likely to provide appropriate compensation for most applicants for the reasons set out above, without them having to provide further evidence of loss. If they also qualify for the Severe Health Condition award this will itself add to the amount of compensation they receive for financial loss.
To acknowledge the Inquiry’s recommendation on effective treatment and the calculation of financial loss awards for those with Hepatitis B and C, amendments to the March 2025 regulations have removed the minimum earnings threshold for a person to claim the exceptional financial loss award. This will allow applications to show that they were unable to return to work, or unable to work at the assumed level, even after the introduction of effective treatments. Individuals will be able to bring forward evidence that their earning capacity was lower than that assumed by the scheme.
The award offered by the exceptional loss award will more closely reflect an applicant’s actual financial loss rather than assumptions used by the core route as it will reflect the actual salary and earnings capacity.
As these awards are based on an evidence-based assessment of the applicant’s actual circumstances, they will replace any tariff-based Financial Loss award already provided under the Supplementary route Severe Health Condition award. This could mean that for some applicants, an Exceptional Loss award for financial loss turns out to provide a lower amount than they would have received if they had only applied for the Severe Health Condition element of the Supplementary route. In this circumstance, the applicant would be awarded the new, lower amount of financial loss. It is therefore important for an applicant to consider if an Exceptional Loss award for financial loss is appropriate for their circumstances. IBCA will support applicants in making this decision.
Exceptional Loss awards for financial loss will have no impact on the Financial Loss awards an applicant will receive under the core route. This means that even if it turns out someone who applies to the Exceptional Financial Loss award should actually receive less than the core route amount (based on the evidence they provide), there will be no impact on their core route Financial Loss award. Applicants will always receive their core route Financial Loss award as a minimum.
The Supplementary Route includes two possible Exceptional Loss awards for financial loss. An applicant can apply to one, but not both, of these. The one they choose will depend on the type of income they were earning.
I. High earners: Employment income (PAYE earnings)
This award is designed to offer compensation to employed people whose ability to earn was adversely affected by their infection. If you are (or were) employed, you pay tax on your earnings through a system called Pay As You Earn (PAYE). When calculating an applicant’s compensation under this award, the Scheme will only consider basic pay, overtime pay and incentive pay (that is, the types of income covered by PAYE). The Scheme is unable to take account of income from dividends, shares, investments, capital gains, trusts and savings.
Applicants will need to provide evidence of any earnings from the point at which their earnings were first reduced, all the way through until the year they turn 66. To calculate the income they may have expected to earn were it not for the infection, applicants will also need to provide evidence of their annual salary before the infection reduced their ability to work and their earnings were reduced.
A progression multiplier will then be applied to an applicant’s salary before their capacity to work was reduced. This will work out an approximate lifetime average salary for that person, were it not for the impact of their infection on their ability to earn. The progression multiplier is based on Annual Survey of Hours and Earnings (ASHE) tables, which is in line with Sir Robert Francis’ recommendations. It is a way of compensating someone based on how their salary would have been likely to increase over the course of their career, taking into consideration their age and annual salary. Applicants will also have to provide evidence of any earnings they had after their ability to earn was reduced (this does not include benefits or Infected Blood Support Scheme payments). A compensation award will be made based on the difference between what someone could be expected to earn if they did not have an infection, and what they actually earned.
The award will include a pension award to recognise lost employer pension contributions. This is set at a defined contribution rate of 6.1%, reflective of common private sector occupational pension contribution rates as advised by the Expert Group.
II. High earners: Other earned income (self-employed)
This award is designed to offer compensation to infected people who are/were self employed (including members of partnerships), whose self employment earnings were adversely affected by their infection. The Scheme will only be able to consider certain types of earnings for this award. It is limited to considering trading profits and income from employment including basic pay, overtime pay and incentive pay. The Scheme is unable to take account of income from dividends, shares, investments, capital gains, trusts and savings.
Applicants will need to provide evidence of any earnings from the point their ability to earn was adversely affected by their infection, all the way through until the year they turn 66. To calculate the income an infected person may have expected to earn were it not for the infection, applicants will need to provide evidence of earnings for a full 5 years prior to the point at which their infection caused a reduction in earnings. These earnings will be averaged to calculate the annual amount an applicant would have likely earned if their ability to earn had not been impacted by the infection. Applicants will also have to provide evidence of any earnings they had after their ability to earn was reduced (this does not include benefits or Infected Blood Support Scheme payments). A compensation award will be made based on the difference between what someone could be expected to earn if they did not have an infection, and what they actually earned.
As self-employed people would not have received employer contributions to a pension, there is no award made for pension years for self-employed high earners.
b. Exceptional Loss awards for paid for care costs
The core route recognises that infected people will have needed care in the past, and that they should be compensated for this. However, it also assumes that past care for infected people was normally provided informally (by friends and family, for example). This means that, when awarding someone their core route award for past care, IBCA deducts 25% from 2024 commercial care rates to take into account certain costs (such as tax) which would have been paid by a professional but do not apply in the case of someone who provided care free of charge at the time.
The Exceptional Loss awards for paid for care costs each provide additional compensation to infected people who can provide evidence they paid for care in the past (on or before 31 March 2025) where the Scheme assumes care was provided gratuitously.
There are two different awards available to recognise paid for past care costs. These are described below:
I. Care (excess deemed costs) award - removal of 25% gratuitous care deduction for past care costs:
Applicants can apply for the 25% deduction on past care to be removed where they can provide evidence that they paid for their care in the past. Evidence of this paid-for care must be provided for a minimum of 6 months, and it must show the specific type of care provided. The paid-for care will then be matched to the appropriate care band (e.g. end of life care) recognised by the Scheme in the core awards. The 25% deduction for this specific care band will be removed from the Past Care award to reflect that the care was paid for.
II. Care (excess actual costs) award - care costs in excess of 2024 commercial rates:
Applicants can alternatively provide IBCA with evidence of all past care costs. If these exceed their total Severe Health Condition (if applicable) and core award for care, they will be eligible for this award. In this option, past care costs will be uprated to 2024 values using CPI. Then, an award will be calculated based on the excess amount paid for care beyond the total already provided through Severe Health Condition and core Care award. This new award will be capped at 25% of the amount an applicant would have been eligible for under the Severe Health Condition and core route and is paid in addition to those awards. This is in line with advice from the Expert Group that care costs in excess of this amount are likely to be in relation to other non-infection related comorbidities or age, rather than in relation to the infection itself.
Exceptional loss awards will not be available for care received after 31 March 2025. This is because future care is calculated using full 2024 commercial rates with no deduction applied.
The Supplementary Route for Affected People
The financial dependency award
The core route for affected people includes a Financial Loss award for bereaved partners and children, including an uplifted award for children who have lost both parents to infected blood related infections. There is an additional supplementary Financial Loss award available to bereaved affected people who were financially dependent on an eligible infected person at the time of the infected person’s death.
This supplementary award recognises that some affected people may have experienced a greater financial loss than the core route assumes based on their relationship to the infected person. For example, the core route does not assume that a parent would be financially dependent on their child. As such, affected people for whom this applies may be eligible to receive compensation to cover the period of time between the infected person’s death and healthy life expectancy.
The table below sets out eligible applicants for this award and the award amount. As for financial loss awards to infected people, financial loss awards to the affected will include a pension payout calculated at 50% for years where the infected person would have been aged 66 years or over. To claim this supplementary award, an affected person must first have been deemed eligible for compensation through the core route.
Supplementary Financial Loss Award
| Relationship | Eligibility | Award amount |
|---|---|---|
| Bereaved dependent parents | In scope where dependency can be evidenced | £5,561 per annum from the point of death to the estimated healthy life expectancy age of the deceased. (£2,780.50 for years where the infected person would have been 66 or older) |
| Bereaved dependent siblings | In scope where dependency can be evidenced | £5,561 per annum from the point of death to the estimated healthy life expectancy age of the deceased. (£2,780.50 for years where the infected person would have been 66 or older) |
| Bereaved children over the age of 18 with a disability that leads to dependence on a parent post-childhood | In scope for additional dependency payments | £5,561 per annum from the point of death to the estimated healthy life expectancy age of the deceased (less the core route Financial Loss award). (£2,780.50 for years where the infected person would have been 66 or older) Bereaved child who has lost both parents to infected blood related infections while under 18: £22,243 per annum from the point of death to the estimated healthy life expectancy age of the deceased, £16,682.25 for years where one parent would have been 66 or older; £11,121.50 for years where both parents would have been 66 or older (less the core route Financial Loss award) |
To be eligible as a bereaved parent or sibling, an applicant must provide evidence of sufficient financial dependence on the infected person (this could include, for example, provision of housing or meals), at the time of the infected person’s death. This dependency must also have been maintained over a period of at least six months prior to death.
Where dependency can be proved, it allows the affected person to receive a Financial Loss award when they were not otherwise eligible for one through the core route (e.g. a bereaved dependent sibling), or top-up their core Financial Loss award (in the case of bereaved children who have a continued claim after the age of 18 due to a disability).
Applicants for this award should indicate their intention to apply for it at the point of their initial application to IBCA. Eligible affected people will not be able to make a subsequent application for the supplementary dependency award after they have received and accepted their core route award.
Children under 18 who are not disabled, or bereaved partners, are not eligible for this award as they will already receive dependency payments through the Financial Loss award underpinned by the core route. It also does not include applicants who are only eligible as carers. This is because only carers who provided care without reward or remuneration (e.g. without payment) are eligible for the Scheme.
Infected Blood Support Scheme (IBSS) Payments
All infected beneficiaries registered with an IBSS before 1 April 2025 will continue to receive Support Scheme payments for life, should they choose to do so. In line with recommendation 9a of the Infected Blood Inquiry’s Additional Report, applications for bereaved partner support scheme payments have reopened for those bereaved after 31 March 2025 (where their infected partner had not received compensation from IBCA).
IBCA will take responsibility for making support scheme payments in a phased handover from January to March 2027. IBCA requested this delay to allow them to concentrate on accelerating the delivery of compensation and expanding the service this year, while ensuring there is no disruption to those receiving support scheme payments. The IBSS will continue to make payments until the new transfer dates.
Responsibility for making these payments will transfer from the IBSS to the IBCA on the following dates:
a. Wales Infected Blood Support Scheme on the 15 January 2027
b. Scotland Infected Blood Support Scheme on the 1 February 2027
c. Infected Blood Payment Scheme for Northern Ireland on the 1 February 2027
d. England Infected Blood Support Scheme on the 23rd March 2027
These payments will continue to be paid with no gap whilst waiting for IBCA to process compensation applications; but there will be a ‘switch over’ date when IBCA will start to make the payments, rather than the Support Schemes. This is to bring all administration into IBCA for consistency and simplicity. In practice, this ‘switch over date’ will not affect the regular payments that beneficiaries on the Support Schemes receive. IBCA and the Support Schemes will communicate with beneficiaries on what they can expect when the switchover happens.
The Cabinet Office and IBCA will continue to work closely with the Department of Health and Social Care, the Devolved Governments in Scotland, Wales and Northern Ireland and the IBSS administrators across the four nations to help ensure that the transfer to IBCA is as smooth as possible.
For infected and affected IBSS beneficiaries who choose to continue to receive Support Scheme payments for life, Support Scheme payments will not be taken into account when assessing an applicant’s Injury, Social Impact, or Autonomy awards, or in relation to past Financial Loss or past Care awards. Applicants will be able to access these parts of their compensation as a lump sum or periodic payment over 5, 10 or 25 years.
Support payments will continue to be paid to IBSS beneficiaries on an ex-gratia basis until 31 March 2025. From 1 April 2025 onwards, all IBSS beneficiaries will continue to receive support payments for life if that is the option they choose. Payments will be made at the April 2025 rate and the value of the support payments will be uplifted each year in line with the Consumer Price Index (CPI). Any support payments paid from 1 April 2025 will be taken into account when IBCA calculates the amount of compensation that a person is entitled to for the awards relating to their future financial loss and care costs. IBCA will compare the future financial loss award and future care award under the Scheme with the person’s estimated Support Scheme payments up to their healthy life expectancy.
This is because support scheme payments after 31 March 2025 will fund that person’s future financial loss and care costs until the end of their life. This is in line with the Inquiry’s recommendations that future support scheme payments are taken into account in respect of the future financial loss calculations under the Scheme. If the Scheme did not count support scheme payments against future financial loss and future care awards, the Scheme would be double compensating those who opt for this route.
For infected IBSS beneficiaries, where the awards under the Scheme are higher than the estimated Support Scheme payments, the person will receive a ‘Support Scheme top-up award’ which will be added to the compensation paid by IBCA. If the awards under the Scheme are lower, this will have no impact on the Support Scheme payments which will continue to be paid at the same rate, increasing annually in line with CPI. This is shown in the diagram below.
Total compensation package
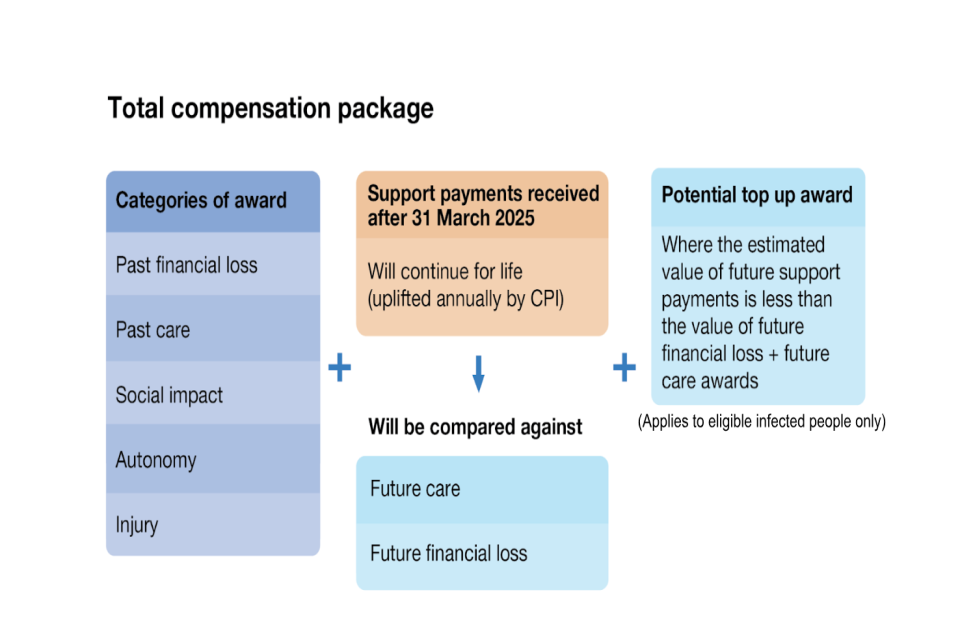
If preferred, an IBSS beneficiary can choose not to continue receiving support payments. They will instead be able to opt for compensation through the core route (in the same way as someone who is not an IBSS beneficiary).
This means that they would receive their future Financial Loss and Care awards as part of their total compensation package. Those choosing the core route will be able to receive their compensation as a lump sum, or as a series of periodic payments over 5, 10 or 25 years.
From 1 April 2025, any discretionary payments received by an IBSS beneficiary will be counted towards compensation calculations by the IBCA. This excludes payments for pre-payment prescription certificates or grants for talking therapy which will not be considered in compensation applications.
IBSS payments for bereaved partners
Bereaved partners registered with a Support Scheme will continue to receive their regular Support Scheme payments (including the yearly winter fuel payment) as part of their compensation package under IBCA. Under this route, a bereaved partner would receive their compensation as follows:
| Injury award | Same as the core route |
| Social Impact award | Same as the core route |
| Autonomy award | Same as the core route |
| Financial Loss (dependency) | Different from the core route offer. For bereaved partners who choose the IBSS route, financial loss will be paid according to the core route from the year after the infected person died, up to and including 31 March 2025. |
| Support Scheme payments | Paid from 1 April 2025 for life in place of core route financial loss (dependency) |
| - | The final award is less any interim payment of £100,000 where relevant, and/or any discretionary payments received from IBSS after March 2025 (excluding any grants for talking therapy) Support Scheme payments will be uplifted yearly for CPI. |
This means that those who are currently in receipt of IBSS bereaved partner payments will be offered a choice of the above, or the core route offer. If applicants choose the core route option, they will need to de-register from IBSS (or opt out once the Scheme moves under IBCA).
The Government committed to re-opening bereaved partner applications to the IBSS for those bereaved after 1 April 2025 where their infected partner had not received compensation from IBCA. Newly bereaved partners who register with an IBSS will be able to receive support scheme payments for life, as part of the compensation scheme, if they choose to do so.
Bereaved partner applicants will not be entitled to a ‘Support Scheme top-up award’ under the IBSS route.
Managing money received through compensation awards
Living infected and affected people receiving compensation through the Scheme will be able to choose to receive their award as:
- a single lump sum payment of the total compensation award;
or
- a series of regular payments (instalments) over a 5, 10 or 25 year period, which will be uplifted annually in line with CPI.
Individuals are able to switch between their IBSS payments and a core award, and between periodic payments and a lump sum after receiving their compensation from IBCA. This is in response to direct feedback from the community.
Where the infected person has died, estate representatives will receive compensation as a single lump sum payment which can then be distributed to beneficiaries of the estate as appropriate.
Where an affected person has died after accepting a claim but before receiving the full balance of their compensation, their estate will receive the remainder of the compensation as a single lump sum payment which can then be distributed to beneficiaries of the estate as appropriate.
IBCA provides financial advice and support that can assist people awarded compensation with managing their compensation awards, accessing financial services, and accessing benefits advice where relevant.
Return to the Scheme due to health deterioration: further core and supplementary route awards
The Scheme is designed to compensate infected people based on the severity of their particular infection. This is why the categories of award are different for the different severity bands. The scheme is also designed to compensate people on the likely progression of their infection, and the impact this is expected to have on their life. That is why, for example, the Care award takes into account the different care needs that someone will be expected to have across their whole life, on the basis of their infection severity.
However, there will be times where an infected person’s health deteriorates so that they change severity banding, or develop a new severe health condition. Depending on their exact circumstances and how much they have previously been awarded by the IBCA, an infected person in this situation may be eligible for more compensation in recognition of the impact this health deterioration is likely to have on their future life. This is known as a ‘return to the Scheme’.
The table below sets out the two circumstances in which someone can return to the Scheme for reassessment, and what the options are for each circumstance:
| Type of health deterioration | Infected people | Affected people |
|---|---|---|
| Infection Severity band change | If an infected person’s health deteriorates and they are diagnosed with a new condition that changes their severity band, they will be able to return to the Scheme for reassessment An infected person can return to the Scheme for reassessment as many times as their condition changes severity band. Return to scheme for a severity band change will result in a further core award payment. Return to scheme for a severity band change may also enable an infected person to apply for an Exceptional Loss award via the supplementary route. After their first application, an infected person will only be able to have their supplementary award reassessed once. |
No reassessment of their own claim following an infected person’s return to scheme. |
| Development of new Severe Health condition | If an infected person’s health deteriorates and they develop a new severe health condition (regardless of whether they were previously assessed to have a severe health condition), they may be able to return to the Scheme. Where an infected person develops a new severe health condition as a result of their infection, they can only return to the Scheme once. |
No reassessment of their own claim following an infected person’s return to scheme. |
If an infected person has already received compensation from IBCA before the second set of regulations were laid, they will be able to return to IBCA for an assessment under the Supplementary route without this being considered a return to the Scheme. This is to make sure they have the same opportunity as anyone else to receive a full core and supplementary route assessment as part of their initial application to IBCA.
An infected person will be asked to indicate whether they intend to apply to the supplementary route when they accept their core compensation offer. If they do not indicate their intention to apply for the supplementary route at this stage, any future assessment by IBCA in relation to a severe health condition will be considered a return to the Scheme.
An infected person cannot return to the Scheme for reassessment under the supplementary route unless they have first developed a new severe health condition, or they have changed severity band. If they have developed a new severe health condition or changed severity band, their reassessment can include consideration of any additional compensation owed through the Severe Health Condition award or Exceptional Loss award. If they have changed severity band, their reassessment can include an Exceptional Loss award. After their first application, an infected person will only be able to have their supplementary award (Exceptional Loss award or Severe Health Condition) assessed once.
For example:
A person infected with Chronic Hepatitis C first applied to IBCA in 2025 and was eligible for a core award (Infection Severity Band of Chronic) and a supplementary route Severe Health Condition award. They subsequently developed a new Severe Health Condition in 2030 and returned to IBCA for reassessment of their supplementary route Severe Health Condition award.
The infected person then developed cirrhosis of the liver in 2035 and returned to IBCA for reassessment due to a change in their Infection Severity Band. Their assessment in 2035 would include a reassessment of their core award and previous Severe Health Conditions. The reassessment in 2035 would not include an opportunity to apply for further supplementary route awards (e.g Exceptional Loss or Severe Health Condition) as the applicant had already returned to the Scheme for reassessment under the supplementary route in 2030. However, the applicant might be eligible for a further core award payment if IBCA determines there has been a change in their Infection Severity Band. Reassessment of the core award for the new infection severity band would include any previous Severe Health conditions for which IBCA had determined the applicant eligible.
Returning to the Scheme for a reassessment following a health deterioration will be possible regardless of the amount of time that has passed since a person’s initial assessment and award of compensation by IBCA. However, the reassessment does need to happen within six years of the diagnosis of the new health deterioration.
In the event of death during the application process
Infected people:
- Should an eligible infected person die after accepting their offer of compensation but before receiving their payment, their compensation award will be paid to the personal representative of their estate.
- Should an eligible infected person die before accepting their offer of compensation, their personal representatives will need to start a new application - IBCA will use evidence which supported the original application so that it does not have to be provided again.
- If an eligible infected person is in receipt of regular support payments (see section on Infected Blood Support Scheme payments) and/or compensation periodic payments at the time of their death, their support payments will stop and the outstanding balance of their total compensation award will be paid to the personal representative of their estate.
Affected people:
- The estates of those that would have been eligible as an affected person, but passed away between 21 May 2024 and 31 March 2031 and did not receive compensation will be eligible to apply.
Time limits for application
Infected Applicants and Estates
For people who are diagnosed before 1 April 2025, the Scheme will remain open to applications for compensation for 6 years from 1 April 2025 (until 31 March 2031). The proposed date for closing the Scheme to people with existing diagnoses will be reviewed within 3 years (by 31 March 2028) to ensure that it remains appropriate based on the numbers of applications and expected processing times.
For people who are diagnosed after 1 April 2025, the Scheme will remain open to applicants for 6 years from their date of diagnosis.
Affected Applicants
Once an infected person receives an offer of compensation from IBCA, the affected person is eligible to apply.
Where an infected person is diagnosed before 1 April 2025, the Scheme will remain open to affected applications for compensation for 6 years (until 31 March 2031).
For people diagnosed after 1 April 2025, the Scheme will remain open to affected applicants for 6 years from the infected person’s date of diagnosis.
Effect of other payments on compensation awarded under the Scheme
Infected Blood Support Schemes (IBSS) and Alliance House Organisations (AHO)
The Scheme is separate from the existing UK IBSS. Any ex-gratia support or payments (such as discretionary payments) received through the IBSS or earlier AHO[footnote 7] before 1 April 2025, will not be deducted from compensation paid through the Scheme.
Any support payments paid from 1 April 2025 will be taken into account when IBCA calculates the amount of compensation that a person is entitled to for the awards relating to their future financial loss and care costs.
From 1 April 2025, any discretionary payments received by an IBSS beneficiary will be counted towards compensation calculations by the IBCA. This excludes payments for pre-payment prescription certificates or grants for talking therapy which will not be considered in compensation applications.
Interim Compensation Payments
Where applicants to the Scheme have previously received interim compensation payments, these will be automatically deducted from the compensation award paid through the Scheme.
Other compensation awards
Any other past compensation awards received (e.g. those made by a court or tribunal or as part of an out-of-court settlement) will be deducted from compensation awards through the Scheme. This does not include any awards made by an AHO.
Should a person choose to pursue litigation after receiving compensation through the Scheme, compensation amounts previously awarded through the Scheme are likely to be deducted from any awards made through the courts.
Impact on tax and benefits
Taxation
Compensation payments made under the Scheme will be exempt from income, capital gains and inheritance tax. This is in line with tax exemptions for the first and second interim payments.
The inheritance tax relief provides a credit against any inheritance tax that would otherwise be charged on a person’s death. For example, if someone received £100,000 of compensation, their estate would have an inheritance tax credit of £40,000 to offset against any inheritance tax on their estate when they pass away.
On 26 November 2025, the Government announced that further updates to the Inheritance Tax disregard will be made to ensure that payments made under the Infected Blood Compensation Scheme and Infected Blood Interim Compensation Payment Scheme are relieved from inheritance tax in cases where the original infected or affected person eligible for compensation has died before the compensation is paid.
This means that an IHT credit will be automatically applied to the estate of the first living beneficiary of the infected or affected person’s estate. For example, this would mean that the children of a bereaved partner who inherits their infected partner’s estate and then dies would not face an IHT charge on the compensation they inherit.
This will apply to compensation payments made before or after 26 November 2025
The Government has also made changes to the rules on gifting compensation payments. The change means that the first living recipients of compensation payments will have two years in which to gift some or all of the compensation payment without an inheritance tax charge.
This will apply to gifts of compensation made on or after 4 December 2025.
Means tested benefits
Compensation payments made through the Scheme will not adversely impact means tested benefits received by people who are either infected or affected.
Where compensation payments are awarded to an estate of a deceased infected person by IBCA and are received by estate beneficiaries on distribution of the estate, the compensation awarded will not impact the recipient’s eligibility for means tested benefits.
Reviews and Appeals
If an applicant is dissatisfied with the outcome of their application to the Scheme, they will have the right to an internal review and the right to an appeal, subject to time limits. Any request for an internal review must be made by the applicant within three months of them receiving their original decision from IBCA. IBCA’s internal review process must be exhausted before the applicant can submit an appeal application. IBCA must take reasonable steps to make sure that the review is carried out by a member of staff who had no involvement in the making of the original decision. When they notify an applicant of the review decision (which they must do), they must give a reason for this decision. If a person is dissatisfied with the outcome of the internal review, they will be able to appeal the decision through the First-tier Tribunal, administered by HM Courts and Tribunals Service.
Rights to litigation
The Government hopes that the Scheme will enable victims of infected blood to receive due compensation without the need to go through a court or tribunal process to seek redress.
Accepting compensation under the Scheme will not, however, remove any right an eligible applicant might have to pursue litigation.
Should a person choose to pursue litigation, any compensation awarded through the Scheme is likely to be deducted from compensation awarded through the courts.
Annex A: Award Tables
Awards for infected people and estates of a deceased infected person
Table 1: Awards for an infected person with a monoinfection (or their estate)
| Category of Award | Hepatitis C or Hepatitis B (Chronic) | Hepatitis C or Hepatitis B (Cirrhosis) | Hepatitis C or Hepatitis B (Decompensated cirrhosis, and/or liver cancer and/or liver transplantation) | HIV |
|---|---|---|---|---|
| Injury award | £60,000 | £120,000 | £180,000 | £180,000 |
| Social Impact award | £50,000 | £50,000 | £50,000 | £50,000 |
| Autonomy award | £40,000 | £40,000 | £50,000 | £60,000 |
For detail on Financial Loss award available see section Further detail on Financial Loss awards
For detail on Care award available see Annex B
Table 2: Awards for an infected person with a HIV & Hepatitis C/B co-infection (or their estate)
| Category of Award | HIV and Hepatitis C (Acute) | HIV and Hepatitis C/ Hepatitis B (Chronic) | HIV and Hepatitis C/ Hepatitis B (Cirrhosis) | HIV and Hepatitis C/ Hepatitis B (Decompensated cirrhosis) | HIV and Hepatitis C/ Hepatitis B (liver cancer and/ or liver transplantation) or Hepatitis B where the infection resulted in a death in the acute period, including the reactivation of Hepatitis B infection leading to acute liver failure and death within 12 months |
|---|---|---|---|---|---|
| Injury award | £182,500 | £195,000 | £240,000 | £270,000 | £270,000 |
| Social Impact award | £70,000 | £70,000 | £70,000 | £70,000 | £70,000 |
| Autonomy award | £70,000 | £70,000 | £70,000 | £70,000 | £70,000 |
For detail on Financial Loss award available see section Further detail on Financial Loss awards
For detail on Care award available see Annex B
Table 3: Awards for an infected person with Hepatitis C & Hepatitis B co-infection (or their estate)
| Category of Award | Hepatitis C and Hepatitis B (Chronic) | Hepatitis C and Hepatitis B (Cirrhosis) | Hepatitis C and Hepatitis B (Decompensated cirrhosis, and/or liver cancer and/or liver transplantation) |
|---|---|---|---|
| Injury award | £75,000 | £150,000 | £225,000 |
| Social Impact award | £70,000 | £70,000 | £70,000 |
| Autonomy award | £70,000 | £70,000 | £70,000 |
For detail on Financial Loss award available see section Further detail on Financial Loss awards
For detail on Care award available see Annex B
Table 4: Awards for an infected person with acute Hepatitis C (or their estate)
| Category of Award | Hepatitis C (Acute) |
|---|---|
| Injury award | £10,000 |
| Social Impact award | £5,000 |
| Autonomy award | £10,000 |
| Financial Loss award | £12,500 |
| Care award | £500 |
| Total | £38,000 |
Table 5: Awards to the estate of an infected person who had an acute Hepatitis B infection where the infection resulted in a fatality in the acute period or where reactivation of Hepatitis B infection resulted in acute liver failure and a fatality within 12 months
| Category of Award | Hepatitis B (Acute where the infection resulted in a fatality in the acute period, including reactivation of the infection resulting in a fatality within 12 months) |
|---|---|
| Injury award | £180,000 |
| Social Impact award | £50,000 |
| Autonomy award | £50,000 |
| Financial Loss award | £17,500 |
| Care award | £41,188.49 |
| Total | £338,688.49 |
Awards for affected people
Table 6: Awards for affected people where the infected person had Hepatitis B (Acute, where the infection resulted in a fatality in the acute period, or where reactivation of Hepatitis B infection resulted in acute liver failure and a fatality within 12 months) or Hepatitis C/Hepatitis B (Cirrhosis) or Hepatitis C/Hepatitis B (Decompensated cirrhosis) or HIV or co-infection
| Category of Award | Partner | Child (where onset of parent’s infection began before the child turned 18) | Parent (where child’s infection started before age 18) | Siblings who whilst under the age of 18 lived in the same household as an infected person for at least 2 years after the onset of the infectionˣ | Carers; Parent (where onset of child’s infection began after age 18); Child (where onset of parent’s infection began after child turned 18); All other eligible Siblingsⱽ |
|---|---|---|---|---|---|
| Injury award | £86,000 | £40,400 | £65,400 | £22,000 | £22,000 |
| Social Impact award | £12,000 | £12,000 | £12,000 | £12,000 | £8,000 |
| Autonomy award | £16,000 | £6,600 | £6,600 | N/A | N/A |
| Financial Loss award | See section Further detail on Financial Loss awards | See section Further detail on Financial Loss awards | N/A | N/A | N/A |
| Care award* | N/A | N/A | N/A | N/A | N/A |
*Affected people are not eligible for Care awards in their own right. On the request of an infected person, Care awards available to infected people can be paid directly to affected people who provided care.
ˣ Siblings must have lived in the same household as an infected person for at least 2 years after the onset of the infection (or would have been expected to live in the same household were it not for the impact of the infection) whilst they were both under the age of 18.
ⱽ All other eligible siblings must have lived in the same household as an infected person for at least 2 years (or would have been expected to live in the same household were it not for the impact of the infection) whilst under the age of 18. This is the case even if that period was prior to the infection, including if the infection happened during adulthood.
Table 7: Awards for affected people where the infected person had Hepatitis C/Hepatitis B (Chronic)
| Category of Award | Partner | Child (where onset of parent’s infection began before the child turned 18) | Parent (where child’s infection started before age 18) | Siblings who whilst under the age of 18 lived in the same household as an infected person for at least 2 years after the onset of the infectionˣ | Carers; Parent (where onset of child’s infection began after age 18); Child (where onset of parent’s infection began after child turned 18); All other eligible Siblingsⱽ |
|---|---|---|---|---|---|
| Injury award | £34,000 | £20,000 | £20,000 | £20,000 | £20,000 |
| Social Impact award | £12,000 | £12,000 | £12,000 | £12,000 | £8,000 |
| Autonomy award | £16,000 | £6,600 | £6,600 | N/A | N/A |
| Financial Loss award | See section Further detail on Financial Loss awards | See section Further detail on Financial Loss awards | N/A | N/A | N/A |
| Care award* | N/A | N/A | N/A | N/A | N/A |
*Affected people are not eligible for Care awards in their own right. On the request of an infected person, Care awards available to infected people can be paid directly to affected people who provided care.
ˣ Siblings must have lived in the same household as an infected person for at least 2 years after the onset of the infection (or would have been expected to live in the same household were it not for the impact of the infection) whilst they were both under the age of 18.
ⱽ All other eligible siblings must have lived in the same household as an infected person for at least 2 years (or would have been expected to live in the same household were it not for the impact of the infection) whilst under the age of 18. This is the case even if that period was prior to the infection, including if the infection happened during adulthood.
Further detail on Financial Loss awards
Financial Loss awards for infected people
The tables below set out the Financial Loss award calculations for infected people.
Financial loss calculations are based on the ‘working lifetime’ of an applicant, from the age of 16 to 65 inclusive. For people who were infected before the age of 16, financial loss is calculated from 16 years old. For those infected after the age of 16, Financial Loss awards are calculated from the age of infection. After pensionable age (66 years old), financial loss is adjusted and calculated at 50% of the financial loss tariffs set out in the tables below. For chronic Hepatitis infections, calculations also take into account the dates at which effective treatments were introduced which are assumed to have affected a person’s ability to work. There is a disregard for the impact of effective treatments for those who were aged 55 or older when effective treatment was introduced. For HIV and HIV co-infections, calculations also take into account the date of diagnosis.
For HIV and all chronic Hepatitis infections, in addition to the financial loss calculation based on loss of earnings, a flat rate award of £12,500 is payable to compensate for notional miscellaneous expenses including, for example, travel to medical appointments and other additional costs (e.g. insurance). Financial compensation for miscellaneous expenses for acute infections is included in the flat rate Financial Loss awards for the acute infection severity bands.
Table 8: Financial Loss award based on disease progression (Hepatitis B)
For all non-acute chronic Hepatitis infections, calculations take into account the dates at which effective treatments were introduced which are assumed to have affected a person’s ability to work. There is a disregard for the impact of effective treatments for those who were aged 55 or older when effective treatment was introduced. This is because it is assumed that someone may have been less likely to be able to return to employment or increase their hours as their health approved, due to their age.
| Milestones for the introduction of major treatments | Chronic | Cirrhosis* | Decompensated cirrhosis, liver cancer* |
|---|---|---|---|
| For those born after 1953: Pre effective treatment (2008 and earlier) | £11,863 per annum | £23,726 per annum | £29,657 per annum |
| For those born after 1953: Effective management from 2009 | £5,931 per annum | £17,794 per annum | £29,657 per annum |
| For those born in or before 1953 | £11,863 per annum | £23,726 per annum | £29,657 per annum |
*Those who were diagnosed with a level 4 Hepatitis infection but are unable to evidence their disease progression will be deemed to have spent up to six years prior to this with a level 3 infection and be compensated accordingly.
Table 9: Financial Loss award based on disease progression (Hepatitis C or Hepatitis co-infection)
For all non-acute chronic Hepatitis infections, calculations take into account the dates at which effective treatments were introduced which are assumed to have affected a person’s ability to work. There is a disregard for the impact of effective treatments for those who were aged 55 or older when effective treatment was introduced. This is because it is assumed that someone may have been less likely to be able to return to employment or increase their hours as their health approved, due to their age.
| Milestones for the introduction of major treatments | Chronic | Cirrhosis* | Decompensated cirrhosis, liver cancer* |
|---|---|---|---|
| For those born after 1961: Pre-effective treatment (2016 and earlier ) | £11,863 per annum | £23,726 per annum | £29,657 per annum |
| For those born after 1961: Effective management from 2017 | £5,931 per annum | £17,794 per annum | £29,657 per annum |
| For those born in or before 1961 | £11,863 per annum | £23,726 per annum | £29,657 per annum |
*Those who were diagnosed with a level 4 Hepatitis infection but are unable to evidence their disease progression will be deemed to have spent up to six years prior to this with a level 3 infection and be compensated accordingly.
Table 10: Financial Loss award for HIV or HIV and Hepatitis co-infection (i.e. HIV and Hepatitis C or Hepatitis B), based on time of diagnosis of either infection
| Milestone for change in impact on earnings | HIV | HIV & Acute Hepatitis C | HIV & Chronic Hepatitis B/C | HIV & Cirrhosis Hepatitis B/C | HIV & Decompensated cirrhosis/ liver cancer Hepatitis B/C |
|---|---|---|---|---|---|
| Following diagnosis | £29,657 per annum | £29,657 per annum | £29,657 per annum | £29,657 per annum | £29,657 per annum |
| Point of infection to diagnosis | £14,829 per annum | £18,536 per annum | £18,536 per annum | £22,243 per annum | £22,243 per annum |
For people who suffered an HIV co-infection with acute Hepatitis B where the infection resulted in a fatality in the acute period, including where the Hepatitis B infection reactivates and resulted in acute liver failure and a fatality within 12 months, a flat rate of £5,000 will be added to the HIV Financial Loss award.
Financial Loss awards for bereaved affected partners and children
Where an infected person dies, bereaved partners and children (who were under the age of 18 at the time of the infected person’s death) are eligible to receive Financial Loss awards. This is due to the fact that the Scheme assumes these cohorts are most likely to have been financially dependent on the infected person. In such cases, a fixed rate Financial Loss award is available, as per the table below.
Other bereaved affected people (disabled children over the age of 18, and parents and siblings of an infected person) may be eligible to receive Financial Loss awards if they are able to provide evidence of financial dependency on the infected person at the time of death and for at least six months prior to the time of death.
Table 11: Financial Loss award for bereaved affected people
| Partner (partners at the time of the infected person’s death) | Child (while under 18) | Child (who has lost both parents to infected blood related infections while under 18) |
|---|---|---|
| £16,682 per annum (for years between infected person’s death and the healthy life expectancy age of the deceased infected person, before the year where the infected person would have turned 66) £8,341 per annum (for years between infected person’s death and the healthy life expectancy age of the deceased infected person, during or after the year where the infected person would have turned 66). |
£5,561 per annum (for years between infected person’s death and child turning 18, before the year where the infected person would have turned 66). £2,780.50 per annum (for years between infected person’s death and child turning 18, during or after the year where the infected person would have turned 66). |
£22,243 per annum (for years between infected people’ deaths and child turning 18, before the year where either infected person would have turned 66) £16,682.25 per annum (for years between infected people’ deaths and child turning 18, before the year where the second infected person would have turned 66). £11,121.50 per annum (for years between infected people’ deaths and child turning 18, after both infected people would have turned 66). |
Annex B: Assumed care requirements for each Infection Severity Band
Table 1: Care band descriptors and costs
The below table shows the bands used to calculate Care awards, with a breakdown of the assumed costs associated with past and future care.
| Care band | Care band description | Care cost (per annum)* |
|---|---|---|
| Domestic support and ad hoc care (Level 1 Care) |
6 hours per week Support with heavier domestic tasks, attendance of medical appointments and household maintenance |
£5,460 |
| Low care (Level 2 Care) |
16.5 hours per week (6 hours per week domestic support + 1.5 hours per day personal care) Domestic support (as above) plus personal care once per day including washing, dressing and grooming |
£23,424.72 |
| Moderate care (Level 3 Care) |
34 hours per week (6 hours per week domestic support + 4 hours per day agency home care) Domestic support (as above) plus increased personal care, assistance with meals and attendance of health appointments |
£51,285.92 |
| High care (Level 4 Care) |
41 hours per week (6 hours per week domestic support + 5 hours per day agency home care) Domestic support (as above) plus full personal care, full assistance with meals and attendance of health appointments and medication |
£62,742.40 |
| End of Life care (Level 5 Care) |
24 hour support (2 x 12 hour shifts) | £109,835.96 |
*As the Inquiry acknowledged, past care is likely to have been provided gratuitously. The awards for past care are therefore 25% lower than current commercial rates. This reflects the fact that where care was provided gratuitously, the associated cost would have been exempt from tax, national insurance and other costs, which would otherwise be payable if depending on a professional carer.
Table 2: Assumed care requirements for each Infection Severity Band
This table shows the assumed level and duration of care (in years) required for different infection severities, which are used to calculate Care awards under the Scheme.
| Infection Severity Band | End of life care band | High care band | Moderate care band | Low care band | Domestic support and ad hoc care |
|---|---|---|---|---|---|
| HIV | 0.5 | 1.5 | 7 | 5 | 10 |
| HIV and Hepatitis C (Acute) | 0.5 | 1.5 | 7 | 5 | 10 |
| HIV and Hepatitis C / Hepatitis B (Chronic) | 0.5 | 1.5 | 7 | 5 | 10 |
| HIV and Hepatitis C / Hepatitis B (Cirrhosis) | 0.5 | 1.5 | 7 | 5 | 10 |
| HIV and Hepatitis C / Hepatitis B (Decompensated cirrhosis, liver cancer and/or liver transplantation) | 0.5 | 1.5 | 7 | 5 | 10 |
| Hepatitis C (Acute) | N/A | N/A | N/A | N/A | N/A |
| Hepatitis C/ Hepatitis B (Chronic) | N/A | N/A | N/A | N/A | 10 |
| Hepatitis C/ Hepatitis B (Cirrhosis) | N/A | N/A | N/A | 6 | 10 |
| Hepatitis C/ Hepatitis B (Decompensated cirrhosis, liver cancer and/or liver transplantation) | 0.5 | 1.5 | 2 | 6 | 10 |
| Hepatitis B (Acute where the person died during the acute period, including the reactivation of Hepatitis B infection leading to acute liver failure and death within 12 months) | 0.5 | N/A | N/A | N/A | N/A |
Annex C: Severe Health Conditions eligible for supplementary route awards
The below table provides a list of severe health conditions (caused by HIV, Hepatitis B or Hepatitis C infection) that may qualify a person for additional Financial Loss and Care awards through the Severe Health Condition award.
Where an eligible infected person has suffered one of the listed severe health conditions as a result of their infection, further compensation may be available for the associated care costs and financial loss they experienced. Higher compensation available through the Severe Health Condition award will be calculated using the financial loss rates and care costs used in the core route. The amount of compensation awarded will depend on the duration of the severe health condition (or resultant treatment), as well as the Infected Blood Compensation Authority’s (IBCA’s) assessment against the Scheme regulations.
| Severe Health Condition caused by HIV, Hepatitis B or Hepatitis C | Severe Health Condition description |
|---|---|
| Group 1 Severe visual impairment Related to HIV |
Applicants would need to be registered as severely sight impaired (blind) and have evidence of one of the following opportunistic infections secondary to advanced HIV disease: A. Cytomegalovirus retinitis B. Varicella zoster virus necrotising retinitis C. Herpes simplex virus necrotising retinitis D. Toxoplasmosis chorioretinitis E. Optic neuropathy secondary to cryptococcal meningitis F. Cortical blindness secondary to Progressive Multifocal Leucoencephalopathy (PML) |
| Group 2 Neurological disorders resulting in long-term severe physical/ mobility disability Related to HIV / Hepatitis B and/or Hepatitis C Severity bands: Chronic Cirrhosis Decompensated Cirrhosis |
All applicants would need to provide evidence of a social services needs assessment confirming requirement for long term personal and domestic care as defined by scheme in the low care band for a physical or mobility disability. AND Applicants with an HIV infection would need to provide evidence of: A. One of the following central nervous system (CNS) opportunistic infections and neoplasia secondary to advanced HIV disease: i. Cerebral toxoplasmosis ii. CNS Tuberculosis iii. Cytomegalovirus encephalitis iv. Varicella zoster virus encephalitis v. Herpes simplex virus encephalitis vi. Epstein Barr virus encephalitis vii. Progressive multifocal leukoencephalopathy viii. Cryptococcal meningitis ix. Primary CNS lymphoma x. Thromboembolic disease secondary to bacterial / fungal endocarditis B. One of the following central nervous system (CNS) conditions secondary to or associated with HIV infection: i. HIV vacuolar myelopathy ii. Transverse myelitis iii. Thrombotic thrombocytopaenic purpura iv. Cerebrovascular ischaemic/ Haemorrhagic stroke v. Coagulopathies: Antiphospholipid syndrome C. One of the following peripheral nervous system and myopathic conditions secondary to or associated with HIV infection: i. Chronic inflammatory demyelinating polyneuropathy ii. Cytomegalovirus polyradiculopathy iii. HIV myopathy Applicants with a Hepatitis C infection would need to provide evidence of: A. Cryoglobulinaemic vasculitis induced neurological disease that results in severe mobility disability B. Peripheral neuropathy caused by mixed cryoglobulinaemic vasculitis that results in severe mobility disability Applicants with a Hepatitis B infection would need to provide evidence of: A. Peripheral neuropathy caused by mixed cryoglobulinaemic vasculitis that results in severe mobility disability B. Peripheral neuropathy occurring in the context of Hepatitis B associated polyarteritis nodosa (PAN) |
| Group 3 Neurological disorders resulting in long-term severe neurocognitive impairment and/or behavioural disorders Related to HIV / Hepatitis B and/or Hepatitis C Severity bands: Decompensated Cirrhosis |
All applicants would need to provide evidence of a social services needs assessment confirming requirement for long term personal and domestic care as defined by scheme in the low care band (level 2) for a neurocognitive impairment. AND Applicants with an HIV infection would need to provide evidence of one the following conditions for which HIV infection is considered the main underlying cause or is a major contributing factor: A. HIV brain and/or cerebrovascular disease resulting in neurocognitive impairment (dementia) and/or behavioural disorders B. Legacy opportunistic CNS infections secondary to advanced HIV disease, (for example Post infectious encephalitis or Progressive Multifocal Leucoencephalopathy (PML), resulting in neurocognitive impairment (dementia) and or behavioural disorders Applicants with a Hepatitis B or Hepatitis C infection would need to provide evidence of the following conditions: A. Chronic hepatic encephalopathy in association with a decompensated cirrhosis diagnosis of duration in excess of 4 years (the first four years being covered in the core award) |
| Group 4 Psychiatric disorders resulting in long term mental health disability Related to HIV / Hepatitis B and/or Hepatitis C Severity bands: Chronic Cirrhosis Decompensated Cirrhosis |
Applicants with a Hepatitis B and/or Hepatitis C and/or HIV infection would need to provide evidence of a diagnosis by a psychiatrist of one of the following conditions: A. Mood disorders: i. Depressive disorders ii. Bipolar disorders when brought forward by the blood infection or interferon treatment B. Anxiety and stress related disorders: i. Generalised anxiety and panic disorders ii. Post traumatic stress disorders iii. Adjustment disorders C. Psychotic disorders: i. Secondary psychotic disorders due to HIV brain disease, HIV related CNS opportunistic infection or neoplasia, or interferon treatment Supporting evidence For an uplift award to reflect provision of domestic care, all of the following must be provided as supporting evidence: A. Report from a consultant psychiatrist confirming (i) the diagnosis; (ii) the major role of blood borne infection or interferon treatment in the aetiology and / or course of the mental health disorder AND B. One of the following: i. Report from a consultant psychiatrist confirming the patient received consultant-led secondary mental health treatment for six months or more. ii. Evidence of inpatient admissions for treatment of mental health disorder iii. Evidence of history of sectioning under the Mental Health Act For an applicant to receive an uplift award to reflect provision of low care the applicant must satisfy criteria A, B and; C. Social services needs assessment confirming requirement for long term personal and domestic care as defined by scheme in the ‘low care’ band. |
| Group 5 End-stage kidney disease requiring renal replacement therapy (RRT) Related to HIV / Hepatitis B and/or Hepatitis C Severity bands: Chronic Cirrhosis Decompensated Cirrhosis |
Applicants with an HIV infection would need to provide evidence of an end-stage kidney disease listed below which has required renal replacement therapy (RRT) for minimum of 3 months: A. HIV associated nephropathy B. HIV associated immune complex chronic kidney disease C. Drug associated kidney disease in conjunction with treatment with foscarnet sodium or cidofovir or tenofovir disoproxil Applicants with a Hepatitis B infection would need to provide evidence of condition below in addition to renal replacement therapy (RRT) for a minimum of 3 months: A. Membranous Nephropathy B. Membranoproliferative glomerulonephritis including in the presence of mixed cryoglobulinaemic vasculitis C. IgA nephropathy D. Tenofovir disoproxil induced renal failure Applicants with a Hepatitis C infection would need to provide evidence of condition below in addition to renal replacement therapy (RRT) for a minimum of 3 months: A. Membranoproliferative glomerulonephritis including in the presence of mixed cryoglobulinaemic vasculitis |
| Group 6 Other Hepatitis-associated disorders resulting in long-term severe disability Related to HIV / Hepatitis B and/or Hepatitis C Severity bands: Chronic Cirrhosis Decompensated Cirrhosis |
Applicants with a Hepatitis C infection would need to provide evidence of one of the following autoimmune diseases caused by or exacerbated by interferon treatment for Hepatitis C: A. Coombs positive haemolytic anaemia B. Idiopathic fibrosing alveolitis of the lung C. Rheumatoid arthritis Applicants with a Hepatitis C infection would need to provide evidence of one of the following: A. Sporadic porphyria cutanea tarda causing photosensitivity with blistering B. Immune thrombocytopenic purpura C. Type 2 or 3 mixed cryoglobulinaemia accompanied by: cerebral vasculitis; dermal vasculitis; or, peripheral neuropathy with neuropathic pain Applicants with a Hepatitis B infection would need to provide evidence of one of the following autoimmune diseases: A. Coombs positive haemolytic anaemia – caused by or exacerbated by interferon treatment for Hepatitis B B. Idiopathic fibrosing alveolitis of the lung – caused by or exacerbated by interferon treatment for Hepatitis B C. Rheumatoid arthritis – either related to the virus directly or caused by or exacerbated by interferon treatment for Hepatitis B D. Aplastic anaemia where treatment results in long term severe disability |
Scheme summaries for people applying to the Scheme
The following cohort-specific summaries provide an overview of the relevant information about the Scheme for different groups of applicants. The information provided in these summaries is relevant to applicants across all four nations.
Illustrative case studies are provided to show how compensation is calculated in different scenarios. These case studies are based on realistic but fictitious scenarios, with names and profiles created for the purposes of illustration only. Whether an applicant is eligible for compensation and what level of compensation they are eligible to receive will be dependent on the Infected Blood Compensation Authority’s assessment based on the regulations for the Scheme.
These summaries have been updated to reflect the 2025 regulations and amendment regulations.
-
The Macfarlane Trusts, the Eileen Trust, the Skipton Fund, the Caxton Foundation and MFET Ltd ↩
-
Average care requirements used as a basis to award compensation are set out at Annex B. ↩
-
Healthy life expectancy is determined using the Ogden Tables 8th Edition (PDF, 4.5MB). ↩
-
Median salary according to Annual Survey of Household Earnings (all occupations) published by the Office of National Statistics in 2023. The median salary is then deducted for Tax and National Insurance contributions. ↩
-
Retirement age is set at 66 for both men and women. ↩
-
This may include those currently assessed by existing IBSS in the following categories: Hepatitis Special Category Mechanism (EIBSS); ‘Severely Affected’ Hepatitis C (SIBSS); Hepatitis C Stage 1 Plus (WIBSS); Hepatitis C Stage 1 Enhanced Payments (IBPS NI). ↩
-
The Macfarlane Trust, the Eileen Trust, the Skipton Fund, the Caxton Foundation and MFET Ltd ↩