
Annual Report for 2022
Updated 17 July 2023

© Crown copyright 2023
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/raib-annual-report-2022-published-2023/annual-report-for-2022
Our Purpose: We independently investigate accidents to improve railway safety and inform the industry and the public.
1. Chief Inspector’s review of 2022
The railway industry and its people have faced a difficult year in 2022. Knock-on effects of the pandemic and other wider events have affected everyone in some way, and RAIB is no different. Also, a number of valued colleagues have retired or moved out of operational roles during the year, which has naturally led to considerable change in the Branch. Despite the challenges, we have continued to investigate and produce thorough, high-quality reports covering a wide range of accidents, so lessons continue to be learned.
In March 2022, we published our report into the catastrophic derailment at Carmont which made 20 recommendations. I talk more about this in the ‘Management of bad weather’ theme below. We have now received the initial responses to the recommendations from the Office of Rail and Road (ORR) which explain what actions the industry has or is taking, and the ORR status assigned to each recommendation. These responses are tabulated in section 9. I am pleased to see that a lot of effort is being put into addressing the recommendations by the railway industry and associated bodies, and there is no doubt that considerable progress has been made. However, as all but two recommendations remain open, there is still some way to go.
As well as the accident at Carmont, RAIB also published a report into a fatal accident involving a track worker at Surbiton in 2022 and subsequently, in early 2023, reports into fatal accidents involving a train driver at West Worthing and a member of the public at Lady Howard level crossing in Surrey. Such accidents devastate the lives of families and friends of those who lost their lives. Other accidents we have investigated also involved injury, trauma and loss. While relatively rare, such events still have life-affecting and far-reaching consequences for those involved.
The railway is statistically very safe, but we must still look very carefully at what causes accidents and affects their consequences. This is one of the most important ways by which the railway has historically improved safety and reduced harm, and rightly continues to do so.
There are six main themes which have run through our investigative work during 2022; these make up the next section of this review.
1.1 Safety of track workers
One of the things that railways rely on for safe operation, is properly maintained infrastructure. Such maintenance work is often hard and has the potential for serious harm to those undertaking it; managing the risks is vital.
This year we published our investigation report into the accident at Surbiton in early 2021 (report 05/2022), in which a track worker was struck by a train and tragically killed. Thankfully, while no track workers lost their lives in 2022, it is worth noting that previously, after a period of almost five years with no fatalities involving moving trains, track maintenance staff died in accidents each year from 2018 to 2021.
At Surbiton, the accident happened probably because a patroller, who was carrying out inspections and was also responsible for the group’s safe system of work, had become distracted and lost awareness of his position relative to the line the train approached on. The patrol was being undertaken with protection provided by unassisted lookouts. Although this was the usual practice for these inspections, working with unassisted lookouts is the least safe type of system allowed for when working on track. This method of work had not been challenged in the years leading up to the accident.
While working adjacent to an open line, a lookout was struck by a train and injured at Chalfont & Latimer on the London Underground network in April 2022 (report 05/2023). The track worker, who was acting as a lookout, was walking with their back to the oncoming train and stepped into its swept path to gain a better view of the track ahead. While issues such as unfamiliarity with the location and site briefings not being effective were what caused the accident, underlying these was the fact that London Underground’s processes for managing track worker safety did not adequately control the risk to staff working on lines that are open to traffic.
ORR and Network Rail have continued to make great strides in recent years towards radically altering the way track maintenance activities are delivered on the GB mainline railway. A fundamental move away from working on lines that are open to traffic and reliance on warnings provided by lookouts, commonly known as red zone working (more recently referred to in applicable standards as ‘warning safe system of work’), has taken place. This has involved enormous change including increased automation of track inspections, better planning of the interactions between track work and train services and greater use of technology to protect those working on the railway. In terms of reductions in red zone working, this has been a great success and should be applauded.
However, other investigations in 2022 suggest that considerable risk can still exist on a railway with low levels of red zone working. Our safety digests covering near misses at Uphill Junction (safety digest 02/2022), Paddington (safety digest 07/2022) and Bulkington (safety digest 02/2023) and the ongoing investigation into a very close near miss at Penkridge, suggest that considerable risk still exists.
The railway has been rightly moving to work at the higher end of the hierarchy of risk control by using improved technology and planning to reduce the occasions that workers are on or about lines that trains are running on. This has reduced the risk to track workers. However, whether working in planned red zones or not, lower-level risk controls relating to safety behaviours and site safety leadership remain important, if we are to avoid the type of near miss we continue to see, that one day may turn out to be another tragedy.
1.2 Railway operations
In both the 2020 and 2021 Annual Reports, we drew attention to the issue of distraction and its effect on train driver performance. Whether such distraction is a result of fatigue, mobile device use or other factors, it has been a feature of a number of investigation reports in 2022.
We have seen buffer stop collisions at Kirkby (report 07/2022) and Enfield (report 13/2022), along with Signals Passed at Danger (SPADs) at Sileby, leading to a near collision (report 06/2022), and at Doncaster (leading to a collision, ongoing investigation). Following two previous years including similar incidents, this is a concern.

Train driving, and maintaining full concentration on that task, is demanding. Despite this, errors leading to significant consequences are rare, partly because of driving becoming so professionalised and partly because of the engineered safeguards in place. However, to reduce the occurrence and effects of driver distraction, we need to look at both areas. Organisations need to consider the level of support they provide drivers, for example, in terms of fatigue and lifestyle management. The railway also needs to think carefully about technology. Twenty years after its introduction as a stop-gap measure, does the Train Protection and Warning System (TPWS) provide sufficient mitigation of risk now? The railway has also been researching improved technology to detect and monitor driver awareness and alertness. Such systems have had a very positive effect in parts of the light rail industry.
We have recommended as a result of the Kirkby investigation that the Rail Safety and Standards Board (RSSB), in consultation with relevant stakeholders and bodies representing staff, should undertake further research into how the detection and mitigation of a loss of alertness or attention in train drivers can be improved. Encouragingly, work is progressing in this area.
Universal, fully automatically protected train operation is likely to be many years away on the mainline railway. Meanwhile, in the face of a number of serious events involving distraction and evolving technology, the railway needs to examine very carefully what more can be done to either avoid or mitigate the effects of the rare errors drivers will inevitably make.
Another area where drivers can be helped is by better provision of information. Of particular note have been a number of groups of diverse and distributed incidents relating to Blanket Emergency Speed Restrictions (BESRs). The use of such speed restrictions was widened after the Carmont derailment. Very heavy rain (report 08/2021), Storm Franklin (RAIB letter to industry), and extreme heat in summer 2022 (safety digest 06/2022) led to the application of such speed restrictions as a risk mitigation measure. However, in each case, a number of trains passed through the affected areas at well above the allowed speed because of breakdowns in communication. In the case of emergency speed restrictions, the railway still largely relies on drivers reading and remembering notices posted where they book on for duty. In the current era of easy communication, there must be another way to convey information that is an essential component of mitigating certain weather-related risks.
1.3 Management of bad weather
Although railway safety in the UK has been steadily improving over recent decades, the tragedy at Carmont is a reminder of just how disruptive and potentially dangerous Britain’s weather can be. The railway industry is aware that it needs to continue to become smarter about the way it counters this threat, and to better exploit remarkable modern technology that enables the prediction and tracking of extreme weather events such as summer convective storms. There is also an urgent need for the railway to provide real-time decision-makers with the information, procedures and training they need to manage complex and widespread weather-related events across the rail network.
No one wants to shut down the railway every time it rains. Railways need to operate safely and reliably in most weather conditions. If they are not able to achieve this, potential passengers will be forced onto the roads, which are undoubtedly much more dangerous in bad weather conditions.
Clearly there is a balance to be struck and technology can help to get this balance right. Modern weather forecasting and monitoring systems can spot the truly exceptional events before they occur and as they happen, so allowing railway operators to implement precautionary measures when it is prudent to do so. This would benefit the safety of the line (by restricting train speeds, or suspending operations, when necessary) while reducing the need for imposing blanket speed restrictions over areas that are not at significant risk.
It is important not to dismiss this truly harrowing accident as a one-off event. The railway industry needs to continue to think through the implications of severe weather on its infrastructure, while also looking at the behaviour of trains should they derail after striking obstructions such as washouts and landslips. These are some of the areas RAIB’s report into the Carmont derailment (report 02/2022) sought to address and the status assigned by ORR in early 2023 to each of the industry’s responses are tabulated in section 9.

1.4 The safety of people getting on and off trains
Sadly, there are two platform edge accident scenarios RAIB repeatedly sees. In one, a passenger falls between the train and the platform edge, the person responsible for train dispatch (driver, guard or platform staff, depending on circumstances) is not aware of what has happened and the train is allowed to leave the platform. In the other, more common, scenario, a passenger attempts to board the train as the doors are closing and becomes trapped in the doors. The technical systems are unable to detect their presence (usually because the trapped object is thin and/or deformable, for example, a hand or a bag strap) and again the person responsible for dispatch is not aware of this and the train departs. Such events occur in both mainline and tram operations.
In 2022, we have published three digests covering five such incidents. The first relates to a passenger who, after their hand became trapped in a closing train door, was forced to run alongside the train at Wood Street station in London (safety digest 01/2022). The driver noticed what was happening and stopped the train. The second relates to a passenger who was dragged around 13 metres before falling onto the platform at Shudehill tram stop in Manchester (safety digest 04/2022), after their bag became trapped in a departing tram’s closing doors. They sustained injuries to their face and hand. The third digest (safety digest 05/2022) covers three incidents in the space of a week where passengers were dragged at different north London stations with their respective hand, walking stick and umbrella in departing train doors. There is no indication that any of these passengers were injured. However, as numerous accidents in previous years have shown, such incidents can easily be much worse, causing death and serious injury.
The broad lessons of such events have remained the same over a number of years:
- Those responsible for dispatching trains need sufficient support, equipment (including the ability to stop the train directly themselves) and training
- Train or tram door interlocks cannot be relied on in all cases; a thorough final visual check (via CCTV systems in some cases) is vital
- Operating companies must continue to educate passengers, particularly that train and tram doors do not behave like lift doors, a commonly-held misconception
- Platform-to-train side gaps should be minimised
- Ever-improving obstacle detection technology should be pursued
- Risk should be assessed, and consequent spending decisions made, at individual platforms and not aggregated over many
1.5 Safety at level crossings
Level crossings are the only places where members of the public normally interact with railway operations other than when travelling by train. It is vital that they understand the potential dangers and act accordingly. In last year’s Annual Report, we talked about the risk at user worked level crossings, where a person wishing to cross the railway with a vehicle has to operate gates or barriers themselves. They are expected to gain the knowledge of how to do that safely by reading signage and being briefed by the authorised user of the crossing, the person or organisation with rights of access over it. At the time, such crossings had featured in 22 of our reports and safety digests since 2005. With the publication of reports about Coltishall Lane (report 03/2022) and Kisby (report 12/2022) in 2022, that is now 24. At Coltishall Lane, motorists on a public road narrowly avoided being hit by a train. At Kisby, a tractor and trailer on a private road was hit, resulting in injury to the train driver, destruction of agricultural equipment, derailment of a railway wagon, damage to a locomotive and a lucky escape for the tractor driver. In both cases, the crossing was not used correctly because the users did not know how to.

Signage is provided, but as previous RAIB reports have explained, the instructions on it are not user-friendly or clear. In response to earlier RAIB recommendations, Department for Transport (DfT) has for some time intended to introduce new regulations to improve the signage. This remains ongoing, revised designs exist and DfT envisages the current legislative programme will allow implementation in 2023. However, RAIB had previously recommended in our report into the accident at Frognal Farm (report 12/2018) that as well as reviewing signage, Network Rail with ORR and DfT support, should also consider the practicality and feasibility of the current arrangements by which authorised users are expected to brief and inform other potential users of such crossings. This is in view of the increased dependence of occupiers on delivered goods and services from a plethora of sources, and other factors which may increase the number of crossing users. In essence, we still have a nineteenth-century concept in a twenty-first century environment.
The fatal accident at Lady Howard footpath level crossing (report 01/2023) and near miss with a number of young people at Farnborough North level crossing (report 04/2023) were both cases where the high risk associated with a particular crossing was understood, but insufficient action had been taken in a timely way to properly mitigate the risk. Closing or modifying crossings is complex and can be expensive. Balancing spending priorities, local stakeholders content with the status quo, changing available technology and relatively rapid turnover of the type of staff involved in such work are some of the issues we often see. There are a large number of footpath and bridleway crossings, used by many people and many trains. It is virtually inevitable that if crossings known to present a high risk to the user remain with insufficient mitigation for prolonged periods, this will manifest itself in near miss incidents and possibly worse.
1.6 Management of low adhesion
There are two distinct consequences associated with low adhesion that RAIB has investigated in 2022.
Near Salisbury on 31 October 2021 (ongoing investigation), a passenger train was unable to stop in advance of a red signal, which it passed. It then ran onto a junction and collided with the side of another train travelling more slowly in the same direction as they entered Fisherton Tunnel. This caused serious injury to the train driver, minor injuries to passengers and significant damage to both trains and the infrastructure. It was the first collision between two passenger trains travelling at speed that RAIB has investigated since its inception in 2005. If the train had passed the signal less than a minute earlier, it would have hit another train travelling in the opposite direction, almost certainly with far more severe consequences. One of the causal factors was very low wheel/rail adhesion on the approach to the red signal.
At Pencoed (report 03/2023), a loaded wagon developed wheel flats probably as a result of a wheelset not rotating as the train braked over an area of very low adhesion. When the wheelset with flats started rotating again, the flatted wheel caused rail breaks along the route. Although these consequences are not particularly severe, wheel flats, however caused, can lead to derailments such as occurred at both Llangenech (report 01/2022), where a tanker train derailed, spilled its contents, caught fire, and polluted watercourses, and Carlisle (ongoing investigation) where a cement wagon ended up in the river Petteril. In both these cases, the railway was closed for weeks for expensive recover and repair operations and at Llangenech the environmental effects lasted for months.
The use of steel wheels on steel rails means that rolling resistance is low, so a single locomotive can haul a heavy train very efficiently. One of the downsides, however, is that the friction between the wheel and rail varies considerably with the effects of moisture, rust, leaf fall and other contaminants. The railway handles this in a number of ways: vegetation management, defensive driving, operational measures to allow trains more distance to brake in, on-train technology to modify or make best use of available adhesion, and taking active measures to make the rails less slippery. This wide range of measures is usually very effective at managing the risk. However, issues with adhesion have existed for as long as the railway and are an inherent part of it; considerable vigilance remains necessary if accidents, such as those we have seen recently, are to be avoided.
1.7 Concluding thoughts
The six themes relate to the areas that our investigative work in 2022 suggests are most significant.
I have deliberately chosen not to include the role of management assurance under headings that refer to specific examples, because the role of assurance in the management of safety is a feature of most investigations we undertake. As I noted last year, management assurance is not just about audits and compliance checks. Formal processes need to be complemented by a culture that encourages information to flow, so those in positions of responsibility understand ‘what is’, rather than ‘what should be’ or ‘what they wish it to be’. People at any level need to be able to speak up about the reality of what concerns them without risk to themselves, in order that managers are fully aware of what is happening in their organisation. This is not easy: giving a boss or an employing organisation bad news may well not be in someone’s interest. However, to manage safety effectively and reduce the risks associated with the types of events we investigate, the industry must continue to strive to understand how to make management assurance really work.
I have become more concerned in the last year about the perils of forgetting what history has taught us. I have started to wonder whether recent accidents suggest that the railway is indeed forgetting the lessons of the disaster at Clapham in 1988 which was a result of faulty wiring in the signalling system. We have introduced an additional ‘summary of learning’ on our website this year which explains this in more detail.
When, in September 2022, RAIB published the Dalwhinnie report (report 10/2022) about a signalling system failure that led to a derailment, I wrote, ‘Wiring within a signalling system is safety-critical and needs to be carefully checked and tested when engineering work is carried out. It is essential that long-established processes and assurance principles, introduced and developed as a result of earlier accidents, are followed.

Those who don’t remember the past are condemned to repeat it, has been said in many ways by many people. When it comes to fully understanding the importance of hard-learned lessons around the wiring of railway signalling, the accident at Dalwhinnie needs to act as another salutary reminder to the industry.’
Only a month or so later, in October 2022, a train passed a red signal in Derbyshire and was braked to a stand; the signal should have been showing a yellow aspect. The train behind then passed the same signal showing a yellow aspect when it should have been showing a red one and stopped behind the first train. This was caused by a wiring error; in this case there were no significant consequences and we will publish our investigation findings in due course. However, next time the price for not learning the lessons of the past may be much higher.
Perhaps unsurprisingly, there is considerable overlap between the 2022 themes, and the themes in 2021 and the years before. At both a high level and in very specific instances, as illustrated in the safety at level crossings theme, the railway almost always knows what risks are present and, in many cases, understands the risk well. The problem is often how long it takes to sufficiently mitigate a known risk and the occurrence of accidents and incidents in the intervening time.
Many things can slow efforts to mitigate known risks appropriately. Examples such as difficulties with external stakeholders, navigating over-complex processes, the need to prioritise when resource is limited, banking on upgrades that don’t arrive when expected, over-optimism in the programming of solutions and allowing ‘the perfect to be the enemy of the good’ have occurred throughout railway history, and still do. Explanations or justifications of individual delays in the implementation of appropriate mitigation often seem reasonable, particularly in a complex environment with competing pressures, but there does appear to be a pattern that the industry needs to reflect on.
To conclude, I would like to thank my colleagues at the Branch and those who assist us. RAIB is made up of expert and dedicated people who work tirelessly to extract the safety lessons from accidents to help make the railway safer for those who work and travel on it. It is not always easy, but it is hugely worthwhile work. We are invariably assisted by many other organisations, and by the people who have been involved in accidents or have been affected by the consequences, sometimes in stressful and difficult circumstances. Our aim is simply to improve railway safety and inform, and I am extremely grateful to all those who assist us in this.
Andrew Hall
Chief Inspector of Rail Accidents
May 2023
2. Our priorities
During 2022, our priorities were:
- maintaining the production of high-quality, timely investigations
- keeping up with changes in technology and industry structure
- recruiting, developing and keeping the right expertise
- continued positive engagement with the rail industry and other statutory bodies
- preserving and enhancing RAIB’s international contacts
- resolving (with other AIBs and the Chief Coroner) issues around legal judgements that set out how coroners and the AIBs interact
- working with other railway accident investigators in the UK to share good practice and to help improve the quality of investigations
3. Operational activity
Our operations are governed by law. The Railways (Accident Investigation and Reporting) Regulations 2005 (the Regulations) describe the types of accidents and incidents the UK’s railway and tramway industries are required to report to us.
Between 1 January and 31 December 2022, we received 461 notifications, deploying to 22 of these to carry out a preliminary examination on site. We identified a further 23 events requiring a preliminary examination which we carried out remotely. Reviewing the findings of each of these examinations allows us to determine the most appropriate response.
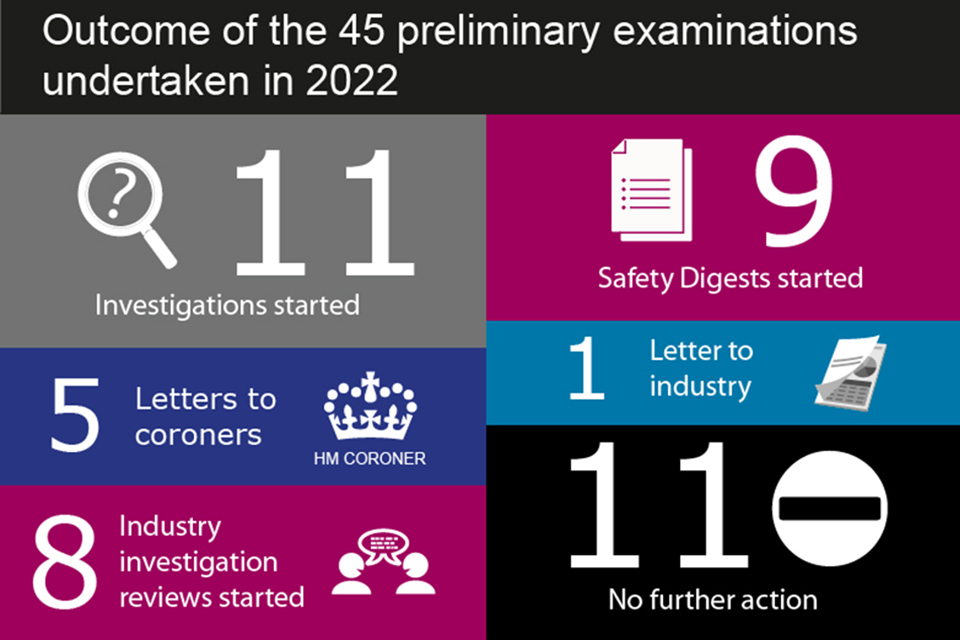
During 2022, RAIB published or issued the following:

RAIB did not issue any urgent safety advice during 2022.
Find out more about how we work and the regulations that govern what we do.
3.1 Accidents investigated by RAIB
RAIB has a duty to investigate all serious railway accidents as defined by the Regulations. These include derailments and collisions of rolling stock resulting in the death of one person, serious injuries to five or more people, or extensive damage to rolling stock, infrastructure or the environment.
We will also investigate incidents and accidents which, under slightly different circumstances, could have led to a serious accident, and which have an obvious impact on railway safety regulation or the management of safety.
We may investigate other notifiable railway accidents where an investigation will contribute to our mission to improve the safety of railways and to prevent recurring railway accidents and incidents.
Before the United Kingdom’s exit from the European Union, RAIB was also required to investigate serious accidents by Article 19(1) of the Railway Safety Directive (EU Directive 2004/49/EC). We were required to report the number of these mandatory investigations separately from non-mandatory investigations of events which under slightly different conditions might have led to a serious accident as defined in Article 19(2). RAIB will no longer report these separate classifications, as it is not a requirement of UK law.
The total number of investigations below therefore includes those mandated by UK law and other accidents investigated in line with our statutory aims.
During the five-year period 2018 to 2022, we started 120 full investigation reports and safety digests.
| Categories | Full investigations | Safety digests |
|---|---|---|
| Events involving moving trains (staff) (25) | 13 | 12 |
| SPAD or unauthorised train movements (15) | 10 | 5 |
| Events involving moving trains (passengers and members of the public) (15) | 10 | 5 |
| Level crossing accidents and near misses (14) | 9 | 5 |
| Freight train derailments (10) | 7 | 3 |
| Collision with an obstacle (9) | 4 | 5 |
| Runaway incidents (9) | 6 | 3 |
| Collisions with other trains (8) | 7 | 1 |
| Passenger train derailments (7) | 3 | 4 |
| Train defects (4) | 2 | 2 |
| Near miss - other (3) | 1 | 2 |
| Infrastructure failures (1) | 1 | 0 |
Twenty-five involved railway employees and moving trains (such as accidents to track maintenance workers) and fifteen involved passengers and moving trains (such as a passenger trapped in train doors and dragged). Fourteen involved harm, or the risk of harm, to people at level crossings.
We also investigated 17 derailments (7 involved passenger trains and 10 involved freight trains), 15 unauthorised train movements, 9 collisions with obstacles, 9 runaways and 8 collisions with other trains.
3.2 Northern Ireland and the Channel Tunnel
RAIB deployed once to Northern Ireland in 2022 but did not investigate the event further. RAIB has continued to liaise with Northern Ireland Railways (NIR) and the safety regulator, Department for Infrastructure (NI), on matters relating to accident investigation and safety learning.
There were no RAIB deployments to the Channel Tunnel or investigation activity related to it in 2022.
We continue to maintain good working relationships with our counterparts in the Republic of Ireland (the Railway Accident Investigation Unit; RAIU), and France (the Bureau D’enquetes sur les Accidents de Transport Terreste; BEA-TT), and with the relevant infrastructure managers, railway undertakings, and safety authorities.
Memoranda of Co-operation (MoC) with RAIU and BEA-TT remain in place. The MoC with RAIU is an agreement on how RAIB and RAIU will co-operate in the event of an accident or incident on or near the international frontier or involving an international train service. Similarly, the MoC with BEA-TT is an agreement on how RAIB and BEA-TT will co-operate in the event of an accident or incident in the Channel Tunnel system (which includes the terminals in Folkestone and Coquelles).
The regulatory regime in the Channel Tunnel is currently in transition. Regulatory supervision of the Channel Tunnel is undertaken by the Intergovernmental Commission (IGC) (for the UK part) and the l’établissement public de sécurité ferroviaire (for the French part).
The UK and French governments are working together to agree a Technical Framework Agreement governing the safety and interoperability requirements for railway operations and rail accident investigation in the tunnel.
RAIB and BEA-TT have been party to these discussions and have agreed text for inclusion in the agreement, which will reflect the intent of both bodies to co-operate in the event of an accident or incident.
Once this agreement takes effect, ORR will assume the role of safety authority for the UK half of the tunnel. The IGC will continue to have responsibility for its functions under the Treaty of Canterbury and the Fixed Link Concession Agreement.
4. Recommendations
Recommendations made as part of an investigation are designed to improve railway safety. They aim to reduce the chance of a similar accident occurring, or to reduce the consequences if such an event were to happen again.
Our recommendations identify organisations we consider best placed to implement the changes required. We refer to these organisations as the ‘end implementers’. These include railway and non-railway, as well as private and public sector bodies.
Most recommendations are addressed to the appropriate safety authority. For the GB railways, this is ORR. In Northern Ireland it is the NI Department for Infrastructure (who are advised by HSENI). The safety authority for the UK part of the Channel Tunnel system is the Intergovernmental Commission until ORR takes on this role under the new Channel Tunnel Technical Framework agreement.
If a recommendation relates to an organisation not regulated by the railway industry’s safety authority it can be addressed to any other public body as such.
The law requires the safety authority to ensure that end implementers consider our recommendations and act on them where required. The Regulations require end implementers to provide full details of the measures they intend to take, or have taken, to implement the recommendation to the safety authority.
The safety authority is required to give each recommendation proper consideration and take appropriate action. It should also inform us of any measures taken in response to the recommendation, or the reasons why no measures are being taken.
We collect information on actions taken in response to our recommendations. This information is generally based on reports we receive from the safety authority (usually ORR). Any public bodies who are the recipients of our recommendations are required to respond directly to us.
4.1 2022 recommendation distribution
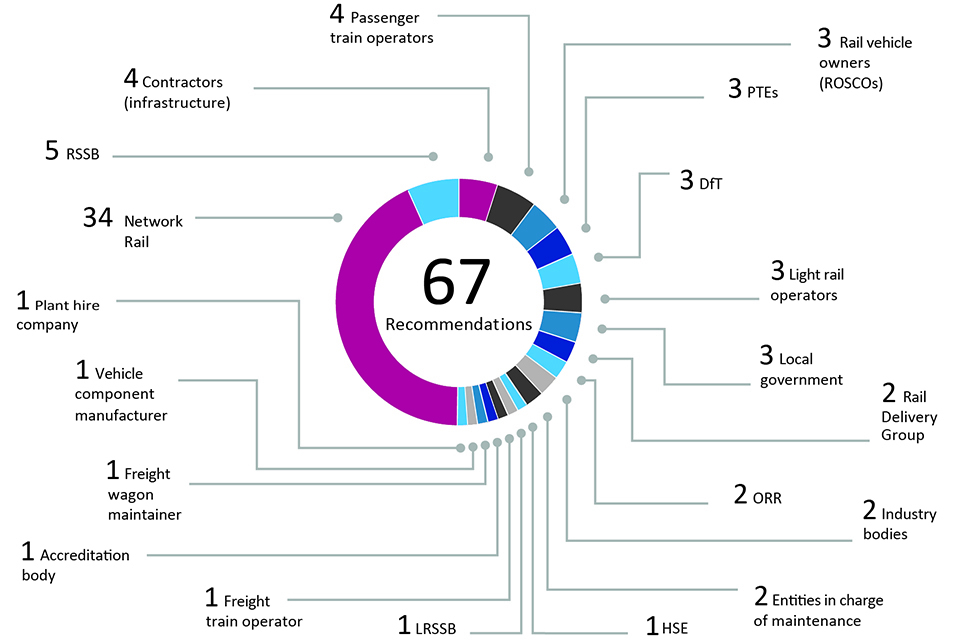
In 2022, we made 67 recommendations directed to 77 end implementers. These included infrastructure owners, train operators, and other authorities. However, some recommendations were made to more than one end implementer.
4.2 The current status of RAIB recommendations
The latest status for each recommendation is available in our index of RAIB recommendations. The index provides information as supplied by the relevant safety authority or public body. Each entry is linked to a recommendation status response that provides the full text of each recommendation.
Responses to recommendations are categorised as:
i. Implemented: all actions to deliver the recommendation have been completed
ii. Implementation ongoing: work to deliver the intent of the recommendation has been agreed and is in the process of being delivered
iii. Implemented by alternative means: the intent of the recommendation has been satisfied in a way we did not identify during the investigation
iv. Progressing: the relevant safety authority has yet to be satisfied that an appropriate plan, with timescales, is in place to implement the recommendation; and work is in progress to provide this
v. Awaiting response: the relevant safety authority has yet to receive a report from the end implementer on the actions that have been taken, or are planned, in response to an RAIB recommendation
vi. Insufficient response: the relevant safety authority considers that the response received from an end implementer is insufficient
vii. Non-implementation: recommendation considered, and no implementation action is to be taken
In 2022, ORR introduced an additional category for recommendations addressed to it:
viii. Closed – carry forward: ORR intends to take no further action as it has been superseded by another recommendation.
Status of recommendations by the year that they were made (as reported to RAIB by 31 December 2022)

Between 2018 and 2022, the status of our recommendations was:
- 54.7% are either implemented, or their implementation is ongoing
- for 19.2% of recommendations the safety authority has yet to be satisfied that an appropriate plan, with timescales, is in place for implementation (that is, the response is still ‘progressing’)
- for 25.7% of recommendations the safety authority has still to report that a sufficient response has been received (these are mainly recommendations made during 2022)
- for 0.4% of recommendations the relevant safety authority considers that the response received from an end implementer is insufficient
- No recommendations have been reported as not being implemented or carried forward
In the five-year period from 2017 to 2021 (that is, those recommendations more than one year old on 31 December 2022) 77.6 % of them have been reported as implemented or are in the process of being implemented to an agreed timebound plan.
4.3 Areas of concern to RAIB
We receive updates on the status of each recommendation from the safety authority, or other public body, to whom the recommendation was addressed. When we receive these responses, we may have concerns about the way an organisation has responded to a recommendation, or about the information provided to us by the safety authority.
In such situations, we will discuss our concern with the relevant safety authority or public body, before recording any remaining concerns in the next Annual Report. The following summaries are those issues identified during 2022.
When we record concerns regarding the actions taken in response to recommendations, we highlight them according to the following categorisation:
Red – we have concerns that no actions have been taken in response to a recommendation.
Blue – we are concerned that the actions taken are inappropriate or insufficient to address the risk identified during the investigation.
White – we note that substantive actions have been reported but we still have concerns about the underlying risk.
Report 07/2020 – Freight train derailment at Willesden High Level Junction
Recommendation 3 - Blue
Intent of recommendation – that Network Rail review and update its management of earthwork structures so that any ongoing movement identified in a supporting earth embankment leads to appropriate monitoring of the associated track. It is also intended that Network Rail look at how the staff responsible for the management of earthworks structures and track maintenance inform each other of potential issues.
ORR status – Implemented
RAIB concern - ORR reported that Network Rail had provided a plan aimed at improving communication and transfer of information between their earthwork management and track maintenance teams.
However, RAIB is concerned that the action taken by Network Rail only addresses the second part of the recommendation’s intent and there is nothing in the proposed actions that considers monitoring track geometry when movement of an earthwork structure is detected.
Report 14/2019 – Fatal accident at Twerton
Recommendation 2 - White
Intent of recommendation – that heritage railways, which use stock that passengers can lean out of, review their relevant risk assessments and implement any additional mitigation measures necessary to achieve an acceptable level of safety.
ORR status – Implemented
RAIB concern – ORR initially wrote to the 50 largest heritage railways (based on passenger steam miles) asking them to act upon recommendation 2 and requesting a response setting out the actions taken to assess the risk of passengers leaning out of a vehicle, or why no action was needed. ORR subsequently received responses from 38 of the 50 operators it wrote to. In January 2023 ORR wrote to any of the 20 largest heritage railways which had not responded to the initial letter. It has now received a response from these railways.
ORR continues to consider the management of this risk through general inspections undertaken as part of its proactive inspection programme for heritage railways.
While RAIB notes the actions taken in respect of the larger heritage railways and understands that this reflects a prioritisation by ORR as the safety authority, RAIB is unable to establish if substantive action has been taken by the 176 smaller heritage railway operators in response to this recommendation.
Report 03/2021 – Track worker struck by train near Roade
Recommendation 3 - White
Intent of recommendation – that Network Rail should consider ways of minimising the need for personnel to access the track as part of implementing electrical safety arrangements.
ORR status – Implemented
RAIB’s concern – ORR found that Network Rail had completed a review of the overhead line electrification (OLE) isolation process. In February 2022 this review made time-bound recommendations relating to OLE isolation including:
- a review of live working tasks
- the issuing of new equipment and improving competency standards
- the application of the hierarchy of risk controls to ensure that the starting point for any task is to consider full isolation
- reviewing planning and maintenance documents and practice
- reducing the number of occasions when separate isolations are required
ORR found that Network Rail had completed a similar review on conductor rail equipment which was due to report in June 2022.
RAIB’s concern is that no details of the results of the conductor rail review were provided, meaning that their effectiveness at minimising the need for personnel to access the track in conductor rail areas cannot be assessed.
Report 08/2020 – Collision between mobile elevating work platforms at Rochford
Recommendation 4 - White
Intent of recommendation – that Network Rail, in conjunction with other stakeholders, review the means of warning currently used to alert staff to a dangerous situation on or near the track, and consider whether suitable equipment should be issued.
ORR status – Implemented
RAIB concern – ORR stated that Network Rail had, in conjunction with its principal contractors and RSSB, reviewed relevant warning systems. Network Rail stated that it was unable to identify a ‘value for money’ engineering solution as part of this review but would continue to work with suppliers to consider new warning systems as they become available.
ORR reported that Network Rail concluded that the warning systems in place during the accident would have been adequate if used correctly and other causal factors were of greater significance.
RAIB’s concern is that the conclusion drawn by Network Rail that the warning systems in place at the time of the accident were adequate suggests that the need for such a recommendation is not accepted. While possible solutions were stated as considered on a ‘value for money’ basis, there is also no evidence presented that cost was considered against safety benefit and shown to be grossly disproportionate.
5. Summaries of learning
The last 17 years of operation have provided us with insights into a range of accidents and their causal factors. This has allowed us to identify recurrent themes. From 2019, we have shared this information with the industry as a series of ‘summary of learning’ documents. As we gather more information, we will add to and update them as necessary. The themes listed in the 2021 Annual Report were:
1 – Design and operation of user worked level crossings
2 – Protection of track workers from moving trains
3 – Managing risk at the platform-train interface
4 – Safe management of abnormal train-operating events
6 – Safe design, operation and maintenance of on-track plant and trolleys
7 – The safe management of weather-related events which affect train operation
8 – The integrity of train braking systems
Where appropriate, they have been updated to incorporate learning from 2022.
This year, we have added a further topic:
9 – Wrong side failures of signalling
Find out more information on each of these areas.
6. Safety and funding
6.1 RAIB’s own safety record
At RAIB, we continue to work to ensure that we have the highest standards for health, safety, and wellbeing in all aspects of our work. We have updated our health and safety governance arrangements by incorporating learning from accidents and incidents. Two minor incidents involving our staff were recorded in 2022.
We continue to develop our relationships with external partners, in particular the air and marine investigation branches. We co-operate and share best practice across a variety of work areas including health, safety and wellbeing.
6.2 Funding
Our operating budget for the 2021-22 financial year was around £5.1 million.
7. Other activities
7.1 Working with academia
Building relationships with universities specialising in subjects relevant to our investigations helps ensure we keep up to date with the latest scientific developments in fields such as mechanical engineering and human factors.
These relationships are also two-way: as well as offering universities sources for ideas and assistance for student projects in areas that benefit RAIB, our inspectors delivered guest lectures to the University of Southampton and The Loughborough Design School. We also provide assistance to the Fundamentals of Accident Investigation and Advanced Rail Accident Investigation courses at Cranfield University.
7.2 External events
During 2022, we participated in a number of external events, either in person or virtually. By promoting and sharing safety learning identified through our investigations, we are able to fulfil our primary mission of informing the industry and public.
We spoke at events hosted by ORR, RSSB, IMechE, Sheffield University, Police Scotland, UK Pathology, Rail Safety Forum, Parliamentary Advisory Council for Transport Safety, the Institute of Occupational Health and Safety and the National Police College (England and Wales) among others.
Find out more about our previous presentations.
7.3 Rail accident investigators’ good practice seminar
Due to circumstances beyond our control, we took the decision to cancel the planned Railway Accident Investigators’ Seminar in November 2022.
Looking forward, we are already putting plans in place to host a seminar for 2023, bringing together guest speakers and investigators from across the industry to share and learn from collective knowledge and experience.
7.4 Road Safety Investigation Branch
We continued to provide support to the Road Safety Investigation Branch (RSIB) as it moves closer to becoming operational. Find out more about RSIB.
7.5 International relations
RAIB has been a longstanding member of the International Transportation Safety Association (ITSA). ITSA is an international network of heads of independent safety investigation bodies, covering all modes of transport, including aviation, marine, railways, road transport, pipelines and underground infrastructure. The membership includes major investigation bodies across five continents, such as the NTSB in the USA and the ATSB in Australia.
Although the UK left the European Union, we maintain relationships with the EU National Investigation Bodies. We are members of National Investigation Body Task Group 1 (Peer Review) and Task Group 2 (Guidance Documents) providing considerable mutual benefit.
RAIB receives periodic requests for assistance from investigation bodies from around the world and, if resource allows, aims to provide it. Such assistance was provided once in 2022.
7.6 The Accident Investigation Chiefs’ Council
The Accident Investigation Chiefs’ Council (AICC) comprises a non-executive chair and the Chief Inspectors from Air, Marine and Rail Accident Investigation Branches.
AICC aims to promote the AIBs’ effectiveness, efficiency and resilience through collaboration: establishing common positions on issues of mutual interest, including the development of joint Memoranda of Understanding and other collaborative working arrangements; developing joint policy across the three Branches; and actively promoting the AIBs as centres of excellence.
Find out more about the role of AICC, its terms of reference and its Memorandum of Understanding.
8. Table of RAIB investigations started, published or ongoing during 2022
(Items prefixed with the letter ‘SD’ are safety digests, the remainder are full investigations)
*As a result of ongoing legal proceedings, this completed report has not been placed on the RAIB website. Embargoed copies were issued on 09/11/2022 to allow the rail industry to start acting on RAIB’s safety recommendations.
9. Response to RAIB recommendations made in the Carmont investigation
Since the end of 2022, progress has been reported by the industry and ORR has updated its assessment of the status of actions taken in response to RAIB’s recommendations on the Carmont investigation. Shown below is a summary table based on information provided by ORR to RAIB on 9 March 2023.
| Status [footnote 1] | Explanation |
|---|---|
| Open (O) | ORR reports that the end implementer(s) has/have taken the recommendation into consideration and is/are taking action to implement it. |
| Closed (C) | ORR reports that the end implementer(s) has/have taken the recommendation into consideration and has/have taken action to implement it. |
| Rec. | Subject | End implementer(s) |
|---|---|---|
| 1 | Contract and project management | Network Rail (O) |
| 2 | New works and maintenance processes | Network Rail (O) |
| 3 | Drainage design | Network Rail (O) |
| 4 | Mixed cutting examinations | Network Rail / Amey (C) [footnote 2] |
| 5 | Reporting incomplete examinations | Network Rail (C) |
| 6 | Mitigating rainfall-related threats | Network Rail (O) |
| 7 | Control room capability | Network Rail (O) |
| 8 | Management assurance of control room functions | Network Rail (O) |
| 9 | Learning from previous events | Network Rail (O) |
| 10 | Risk assessment of mitigating controls | Network Rail (O) |
| 11 | Route proving trains | Network Rail (O) |
| 12 | Derailment mitigation | Network Rail / RDG (O) |
| 13 | Infrastructure-mounted derailment containment | Network Rail (O) |
| 14 | Lifeguards | HST owners (O) [footnote 3] |
| 15 | Glazing | RSSB (O) |
| 16 | Folding tables | Angel Trains (O) [footnote 3] |
| 17 | Secondary impact protection for drivers | RSSB (O) |
| 18 | Corrosion limits | Owners of MkIII stock (O) [footnote 3] |
| 19 | Pre-1994 crashworthiness | Operators of HSTs (O) [footnote 3] |
| 20 | Fire properties of batteries | RSSB (O) |
Version control
| Version | Date | Description of change |
|---|---|---|
| v1.0 | 22 May 2023 | Initial issue |
| v2.0 | 17 July 2023 | Twerton Recommendation 2 concern updated following clarification of action taken by ORR |
-
Effective from 1 January 2023, ORR introduced four new statuses to replace the eight described in Section 4.2. These are: ‘Open’, ‘Closed’, ‘Insufficient response’ and ‘Superseded’. ↩
-
ORR has accepted Network Rail’s justification for not involving Amey in this recommendation. ↩
-
Recommendations 14, 16, 18 and 19 are being taken forward by RSSB on behalf of industry. ↩ ↩2 ↩3 ↩4