
Annual Report for 2023
Published 23 May 2024

© Crown copyright 2024
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/raib-annual-report-2023-published-2024/annual-report-for-2023
Our Purpose: We independently investigate accidents to improve railway safety and inform the industry and the public.
1. Chief Inspector’s review of 2023
At RAIB, 2023 has, in many ways, been similar to 2022. The statistics and themes presented in this report bear that out. The railway industry and those associated with it have faced another difficult year and RAIB is not immune to the sort of pressures and effects of wider events that the industry faces. However, we continue to draw lessons from the wide range of accidents we have investigated and publish reports which clearly explain the often-complex issues behind them.
We have recruited and are training five new inspectors who will return our active inspector numbers to planned strength, after the retirement of a number of valued colleagues in recent times.
RAIB started one investigation into a fatal accident in 2023, which occurred in December at Stratford London Underground station. The investigation into this tragic event is currently ongoing. While having less serious consequences, other accidents we have investigated involved injury and distress. The lessons that can be derived from accidents and incidents that are not fatal should be as powerful and taken as seriously as those that are. They are naturally more numerous and, as well as providing specific learning, can help paint a picture about organisational culture, the effectiveness of management assurance or levels of risk. The more seriously these accidents and incidents are taken, the less likely we are to face fatal accidents and larger-scale catastrophic events such as the derailment at Carmont in August 2020.
The report into that accident was published in March 2022 and given its severity, we have separately tabulated the status of the twenty recommendations in section 9. In accordance with our legal framework, this information was provided to RAIB by the Office of Rail and Road (ORR). A lot of work has been undertaken and progress with closing the recommendations made. However, the majority remain open and there is a considerable way to go.
Train and tram travel in the UK remains statistically very safe. As the accidents and incidents referred to in this report demonstrate, that does not in itself provide immunity from things going wrong. Maintaining safety requires continuous learning and eternal vigilance.
There are six main themes that have run through our investigative activity in 2023; these make up the next section of this review.
1.1 Safety of track workers
Trains can only run safely if the track is properly maintained. This work can be difficult and carries with it the potential for harm as illustrated below.
While working adjacent to an open line, a track worker was struck by a train and injured at Chalfont & Latimer on the London Underground network in April 2022 (report 05/2023). The track worker, who was acting as a lookout, was walking with their back to the oncoming train and stepped into its swept path to gain a better view of the track ahead. While issues such as unfamiliarity with the location and site briefings not being effective were what caused the accident, underlying these were the fact that London Underground’s processes for managing track worker safety did not adequately control the risk to staff working on lines that are open to traffic.

The near miss at Penkridge (report 09/2023), where a line blockage was being used, is another reminder that working on the track remains hazardous. In this incident, track workers split into two groups, with the person responsible for their safety remaining with one group and no safe system of work in place to cover the revised working arrangement. This was a result of a misunderstanding between the track workers and almost cost two people their lives. If a group of track workers has to be split, arrangements must be put in place to ensure that the safety of all members of the group are maintained. Communication must be such that everyone fully understands what safe systems of work are in place.
At Bulkington (safety digest 02/2023), the track worker involved in the near miss was the controller of site safety (COSS) for a team working on the track nearby. The team had been working within the four-foot (the space between the rails) of a line which was under possession (closed to normal rail traffic). This incident occurred because the COSS moved from a position of safety within the four-foot of lines that were blocked to railway traffic to a position very close to an open line. The COSS stated they did this to gain better visibility of the approaching train due to a concern that it may have been travelling towards the workgroup, who were working on one of the lines under possession.
Network Rail has made huge progress in reducing the amount of work undertaken on lines open to traffic. This reduction and the increasing use of technology is reducing the number of near miss incidents that are occurring. London Underground is also taking measures to reduce working on open lines. These changes are welcome. However, the number of near misses we still see shows that some risks have not gone away; great care is still needed. Planning, site discipline, familiarity with location, and work groups knowing precisely where they are and which lines are open to traffic at any given time are still vital.
1.2 The safety of people getting on and off trains
The year saw RAIB investigate platform-train incidents on a heritage railway, a tram network and on London Underground.
In January 2023, a passenger alighting from a train at a Great Central Railway station lost their footing and sustained a serious injury (report 13/2023). The train had made a planned stop at platform 1. The door used by the passenger opened onto the platform end ramp, approximately 1.6 metres beyond the end of the level part of the platform. The passenger, who was visually impaired, lost their footing and fell while alighting from the train because they were unable to safely negotiate the step down onto the platform end ramp.
This was because the level platform was only around 2 metres longer than the distance needed to safely accommodate all of the train’s doors, and the train’s brakes were not performing in a consistent, predictable manner. Measures implemented by the railway had not effectively controlled the risk of passengers using doors which were not adjacent to usable platforms. RAIB identified two underlying factors, that the heritage railway did not have effective processes for learning lessons from operational experience, and had no effective process to support the identification, management and monitoring of risk.
This is not the more usual ‘trap and drag’ type of platform-train interface accident we investigate; some people may regard it as more straightforward. Nevertheless, it caused serious injury to a person and revealed significant underlying factors that investigations over the years suggest may be more widespread in the heritage sector.
More typical of the type of accident we investigate was the dragging of a passenger alongside a departing tram at Beeston Centre tram stop, on the Nottingham tram network (safety digest 04/2023).
Shortly before the tram departed, the passenger had placed a hand and a walking stick into the closing doors of the tram, in an unsuccessful attempt to prevent them from closing. Once the doors closed, the walking stick became trapped. The driver was unaware that the stick was trapped and started the tram. The passenger held onto their walking stick as the tram departed and was pulled alongside the tram for around three seconds, before falling against the tram and landing on the edge of the tram stop.
While our investigations are not yet complete, the same type of issues occurred on London Underground. In February 2023, a centenarian passenger’s coat became trapped in the doors of a northbound Northern line train at Archway station. As the train departed, the passenger was dragged for approximately 2 metres, until their coat came free from the door. The passenger and their companion both fell to the ground during the accident, with the passenger sustaining a serious injury. The train stopped after it had travelled for about 20 metres. In April, a second passenger’s coat became trapped in the doors of a southbound Northern line train at Chalk Farm station. This passenger was dragged for just under 20 metres, until their coat became free of the doors. The passenger fell onto the platform during the accident and sustained minor injuries. The train did not stop and continued its journey.
At Stratford London Underground station in December 2023, a passenger fell from a platform with no train present and remained on the track and was struck, possibly by a number of trains, before being discovered by London Underground station staff. The tragic accident, which is still under investigation, resulted in fatal injuries being sustained by the passenger.
Last year’s Annual Report listed some broad lessons that can be drawn from platform-train interface accidents over the years; they apply to all types of railway and tramway. The events of 2023 have not altered them. Given their importance and widespread applicability, they are worth repeating:
-
Those responsible for dispatching trains or trams need sufficient support, equipment (including the ability to stop the train directly themselves) and training
-
Train or tram door interlocks cannot be relied upon in all cases; a thorough final visual check (via CCTV in some cases) is vital
-
Operating companies must continue to educate passengers, particularly that train and tram doors do not behave like lift doors, a commonly held misconception
-
Platform-to-train gaps should be minimised, not just at the doorways but along the length of the vehicles
-
Ever-improving obstacle detection technology should be pursued
-
Risk should be assessed, and consequent spending decisions made, at individual platforms and not aggregated over many, in an area or on a particular line
1.3 Management of low adhesion
Railways’ and tramways’ use of steel wheels on steel rails means that rolling resistance is low and that heavy loads can be transported very efficiently. One of the downsides, however, is that the friction between the wheel and rail varies considerably with the effects of moisture, rust, leaf fall and other contaminants. This issue generally manifests itself in one of two ways, both of which have been graphically illustrated in RAIB reports published this year.
At Pencoed and Llanharan (report 03/2023), flat spots on the wheels of a freight wagon caused considerable track damage. They were caused by a wheelset locking up under normal braking over an area of very low adhesion. At Petteril Bridge (report 10/2023), similar causes resulted in much more severe consequences, because the flat spots on a freight wagon wheelset resulted in it not rotating over many miles of travel, leading to what are known as false flanges. When the damaged wheels encountered pointwork at Petteril Bridge Junction, the wagon derailed, leading to more wagons derailing, significant infrastructure damage and a cement wagon falling into the River Petteril.

Near Salisbury on 31 October 2021 (report 12/2023), train reporting number 1L53, the 17:20 hrs South Western Railway passenger service from London Waterloo to Honiton, passed a red signal and collided with the side of train 1F30, the 17:08 hrs Great Western Railway passenger service from Portsmouth Harbour to Bristol Temple Meads. At the point of collision, train 1L53 was travelling at approximately 52 mph (84 km/h) and train 1F30 at 20 mph (32 km/h). The collision took place at Salisbury Tunnel Junction, which is on the immediate approach to Fisherton Tunnel, near Salisbury in Wiltshire.
The impact of the collision caused the front two carriages of train 1L53 and the rear two carriages of train 1F30 to derail. Both trains continued some distance into Fisherton Tunnel before they came to a stop. Thirteen passengers and one member of railway staff required treatment in hospital as a result of the accident, which also caused significant damage to the trains and railway infrastructure involved. A potentially far more serious collision between train 1L53 and an earlier train travelling in the opposite direction was avoided by less than a minute.
The causes of the accident were that wheel/rail adhesion was very low in the area where the driver of train 1L53 applied the train’s brakes, that the driver did not apply the train’s brakes sufficiently early on approach to the signal protecting the junction to avoid running on to it, given the prevailing low level of adhesion, and that the braking systems of train 1L53 were unable to mitigate this very low adhesion. RAIB has made ten recommendations to reduce the probability of a repeat of such a serious accident.
The railway manages adhesion risk in a number of ways: vegetation management; defensive driving; operational measures to allow trains more distance in which to brake; technology to modify or make best use of available adhesion; trackside detection of certain train faults; and taking active measures to make the rails less slippery. In future, technology will play an ever-increasing role and the railway is working on evolving technologies to reduce the risk further.
It is important that different parts of the railway fully co-operate to clearly understand and manage risks associated with low wheel-rail adhesion. There are three particular reasons for this: the issue is an inherent part of operating with steel wheels and rails; the physical wheel-rail interface can also be an interface between infrastructure managers and companies that operate trains; and the consequences of not mutually managing the risk can be very serious.
1.4 Overspeeding
At around 10:20 hrs on 17 April 2022, the 08:20 hrs Lumo service from Newcastle to London King’s Cross, passed over three sets of points at Spital Junction at the northern approach to Peterborough station at excessive speed (report 06/2023). The maximum permitted speed over the junction is initially 30 mph (48 km/h), reducing to 25 mph (40 km/h). The data recorder from the train indicated that the first set of points had been traversed at a speed of 76 mph (122 km/h). The speed of the train over the junction resulted in sudden sideways movements of the vehicles. This led to some passengers being thrown from their seats and luggage falling from the overhead storage, with some passengers receiving minor injuries.
Although the train did not derail, and no damage was caused, post-incident analysis has indicated that the train was close to a speed that would have led to it overturning, and it was likely that some of the wheels of the vehicles lifted off the rails. RAIB’s investigation found that the overspeeding was caused by the train driver not reacting appropriately to the signal indication they had received on approach to the junction. This signal indication was a warning that the train was to take a diverging route ahead which had a lower speed limit than the straight-ahead route which they were expecting to take.
At around 13:00 hrs on 4 May 2023, the 09:54 hrs Sunderland to King’s Cross service, operated by Grand Central did exactly the same thing, albeit a little slower. Although the second incident is still under investigation, these two potentially catastrophic events raise some serious questions about the management of this type of overspeeding risk on the railway.
In a different context, on the morning of 14 July 2023, Network Rail issued fourteen blanket speed restrictions (BSRs, previously referred to in some cases as blanket emergency speed restrictions (BESRs)) in anticipation of heavy rainfall, which had been forecast for two days across Scotland (safety digest 06/2023). Information about the BSRs was sent by Network Rail by email to those signal boxes and train operating companies which would be affected. After receiving updated weather information, Network Rail sent information about four additional BSRs at 21:45 hrs to the same recipients as the initial BSRs. Network Rail intended these additional BSRs to be imposed at 04:00 hrs on 15 July, the following day. One of the additional BSR notifications, reference SCR8026, applied to a 2.25 mile (3.6 km) section of railway between Blackford signal box (at the south end of the BSR) and Gleneagles station (to the north). This BSR imposed a temporary maximum permitted speed of 40 mph (65 km/h) from 04:00 hrs to 19:00 hrs on 15 July. The normal maximum permitted speed between these locations was 90 mph (145 km/h).
Around 05:30 hrs on 15 July, the signaller at Blackford signal box observed a northbound freight service operated by Direct Rail Services (DRS) pass through the speed restriction, apparently without reducing speed. The next two trains to pass the signal box were southbound ScotRail passenger services and both observed the BSR. However, the next northbound ScotRail passenger service appeared to the signaller to again pass without reducing speed. The immediate lessons are around clear and robust processes and communication.
More generally, the railway is coming to a crossroads on the issue of overspeeding. Although very different, the overspeeding events above are not protected by an engineered solution. In both sets of circumstances there is a total reliance on an individual signaller or driver to react correctly to information given or presented. Train Protection and Warning System (TPWS) was introduced around twenty years ago, but it was not intended for temporary speed restrictions and an exemption was granted against fitment for protection against overspeeding at diverging junctions. TPWS was also not intended to provide 100% protection in circumstances where it is fitted. TPWS fitment was a stopgap measure while the railway waited to fit automatic train protection, which would bring with it features to supervise the speed of trains. Universal fitment of such technology is a long time away. Does TPWS provide sufficient mitigation of overspeeding risk now and into a possibly long-term future?
1.5 Understanding the integrity of assets
The 2022 Annual Report referred to the management of bad weather, particularly in the context of the tragic Carmont accident. The causes of that accident also include the associated issue of understanding the integrity of assets that are subject to our changing climate.
The investigation of a train travelling over a track washout at Haddiscoe (report 07/2023) found issues related to both weather management and understanding asset integrity, in this case the assets of a third party.
At about 07:45 hrs on Sunday 30 January 2022, a passenger train, which was travelling from Norwich to Lowestoft, ran onto a washed out section of track between Reedham and Haddiscoe stations. The train, which was crewed by a driver and a guard, was carrying five passengers. The driver had seen that the track was flooded ahead of the train and so brought it to a stand. Once the train had stopped, the driver noticed that the ballast was washing away under the train. While preparing to drive back towards Reedham, the situation worsened and a section of ballast washed away, leaving a large void under the track on which the train was standing.
As the driver moved the train it started to lean over. The driver therefore made the decision that it was too dangerous to continue moving the train, and they and the guard evacuated the five passengers.
RAIB’s investigation found that unusually high water levels existed on the day of the incident due to a combination of tidal surge and tidal locking. Localised low spots in the flood defences next to the track concerned then allowed this water to enter the railway. The train involved was not prevented from entering the flooded section of track because Network Rail was not aware that water was entering the railway at this location. RAIB also found that Network Rail’s flood risk management processes were not effective at warning that the track at Haddiscoe was at serious risk of flooding. Underlying factors were that the Environment Agency’s management of flooding risk in the area did not account for, and was not required to account for, the impact of localised flooding on the railway, and that Network Rail was not effectively managing the risks to its assets and services associated with third party flood defences.

At around 18:40 hrs on Friday 10 February 2023, the 17:34 hrs Great Western Railway service from London Paddington to Hereford struck some brick rubble on the single line at Yarnton, between Oxford and Charlbury (report 01/2024). This had fallen onto the track from a failed wing wall adjacent to the line, and which formed part of a bridge carrying a local road over the railway.
The train was travelling at around 58 mph (93 km/h) when the collision occurred and sustained damage but did not derail. There were no injuries to the traincrew or passengers on the service. The wing wall, which included a hidden defect, was known to be in poor condition and collapsed when it was no longer able to carry the load imposed by the embankment it was supporting. Action had not been taken to address risks associated with the wing wall’s deteriorating condition because effective control measures had not been put in place. Our recommendations included the need to improve the process of evaluating defects and improve asset knowledge of wing walls.
These two accidents illustrate some of the difficulties Network Rail faces in understanding asset condition. The age and often undocumented history of its own assets and the fact that some third party assets can affect the railway only add to these difficulties. However, the understanding of asset integrity is crucial in the face of a changing climate.
With respect to third parties, the solutions must lie around integrated approaches: integration of flood risk with weather management strategies, and improved interaction between Network Rail and third party agencies responsible for infrastructure that is crucial to the protection or safety of the railway.
1.6 Corporate memory
On occasions in the past, my predecessor and I have questioned whether the railway is losing corporate memory in relation to wrong side failures of signalling equipment as a result of undetected wiring errors. The 35th anniversary of the major accident at Clapham, in which 35 people died and 484 were injured, was 12 December 2023. That tragedy led to wholesale changes in the way signalling equipment was installed and tested. However, in recent years RAIB has investigated accidents at Waterloo (report 19/2018) and Dalwhinnie (report 10/2022), and an incident at South Wingfield (report 11/2023), each a result of an undetected wiring fault leading to a wrong side failure of signalling equipment.
Most recently at South Wingfield, a train travelling between Derby and Chesterfield unexpectedly encountered a signal displaying a red (stop) aspect. The previous signal had displayed a green (proceed) aspect. As the train was travelling at 100 mph (161 km/h), it was unable to stop before the red signal and passed it by about 760 metres. The train’s driver called the signaller straight away to report the incident. About 17 minutes later, the following train approached the signal which was now displaying a yellow (caution) aspect.
After passing the signal, while travelling at about 20 mph (32 km/h), the driver of the second train saw the taillights of the first train stationary ahead of it and braked to a controlled stop. The second train stopped about 75 metres from the rear of the first train, with both trains now in the same signal section. There were no significant consequences and both trains were able to continue their journeys after obtaining permission from the signaller.
The signal had displayed incorrect aspects to the drivers of the two trains as the wiring controlling its red and yellow aspects was crossed on two terminals in a nearby equipment cabinet, which was where a cable running to the signal was connected to the rest of the signalling system. This cable had been disconnected and reconnected during track engineering work the previous night and this work had introduced the wiring cross, which was not identified when the signal was tested afterwards. The testing was affected by a combination of time pressure, tester workload and possibly by unfamiliarity with the configuration of the signalling equipment.

By the time of South Wingfield, Network Rail had taken steps as a result of previous incidents to assure the signal maintenance testing carried out by its own staff. This had led to a decrease in the number of wrong side failures due to wiring faults. However, an underlying factor at South Wingfield was that this work had not yet included testers employed by contractors; a situation Network Rail is now remedying.
The incidents at Waterloo, Dalwhinnie and South Wingfield saw the integrity of the signalling system being compromised by the incorrect application of the processes developed following the 1988 Clapham Junction accident. Those with personal knowledge of Clapham know the importance of these processes but, as they continue to retire or move away from frontline jobs, this has impacted on the corporate memory vital to achieving safety. On the 35th anniversary of the accident, RAIB supported a number of rail industry organised events intended to raise awareness of the ongoing importance of the lessons learned from the accident and of the need to rigorously apply processes and standards when working on signalling equipment.
Questions about corporate memory have also been raised by an RAIB investigation in a completely different area. At London Gateway (report 14/2023), 5 wagons of a 33-wagon intermodal freight train derailed at low speed as the train was entering the rail terminal at London Gateway port, Essex. The derailment started when wheels on a wagon in the middle part of the train suddenly lifted off the track, just before reaching the port boundary, with the other wagons becoming derailed as they passed over points within the rail terminal. While no one was injured, infrastructure damage disrupted rail freight access into and out of the port for 14 days.
The first derailed wagon was the unloaded centre wagon of a triple-wagon, which was made up of three individual wagons permanently coupled together. The wagons on the train either side of the unloaded centre wagon were all loaded, and a train brake application had recently been made when the derailment occurred. A longitudinal train dynamic simulation model, specially developed as part of the investigation, showed that compressive forces generated in the train were larger towards the middle of the train, where the triple-wagon was located, and rapidly increased to a maximum as the centre wagon approached the place where it became derailed. Data from the train’s on-train data recorder showed that this was shortly after brake forces acting on the locomotive had peaked and that the train’s brakes would have been starting to release.
Among other issues, the investigation found that the risks associated with the longitudinal dynamic behaviour of long freight trains are not well understood in the rail industry and that there are limited processes, tools, and knowledge resources available to assess and manage them. This was identified as an underlying factor. However, design and operational issues associated with longitudinal train dynamics have long been recognised as factors affecting derailment risk. British Rail’s internal derailment investigation guidance from the 1980s provides useful historical context. It mentions traction and braking effects, buffer interaction, and coupling tightness as important influences.
Research published in 2006 by RSSB reviewed UK railway derailment data for the ten- year period between 1992 and 2002. It identified 33 derailment events that were due to longitudinal train dynamic effects. Of these, 27 events related to the presence of sudden severe longitudinal braking forces. Although the rail industry was historically aware of issues such as traction and braking effects and buffer interaction, RAIB found that it had undertaken little research to further develop its understanding of longitudinal train dynamic behaviour and the risk it may pose to modern freight train operation.
Longitudinal train dynamics have not been a recurrent factor in RAIB freight derailment investigations, and it is probable that derailments of this nature have not been occurring as regularly as they once did. This may be due to the type of rolling stock now in service and recent operating trends. With fewer derailments of this type occurring, it is possible that the need to develop understanding in the field has not been considered a priority by the rail industry. However, with an understandable desire to move more freight by rail, using longer and heavier trains, the things that were perhaps more important to the railway in the past may become important again.
1.7 Concluding thoughts
We have not included level crossings as a theme this year, but we did publish one level crossing accident report into a near miss with multiple pedestrians at Farnborough North (report 04/2023).
At the time of publication I wrote:
Behind the incident was an issue of the type RAIB has seen before. Historically the railway knew of the risks at this crossing and ongoing efforts were being made to replace it with a footbridge. This was proving time consuming and difficult, as is sometimes the case when planning decisions are involved.
In the meantime, additional warning lights were installed, and a crossing attendant was provided to remotely control electromagnetic locks on the gates, thereby reducing risk. However, a known residual risk was that the crossing’s users might not respond correctly when the audible alarm and warning lights were activated by an approaching train. In this case people held open the gates for each other as the train approached, meaning the attempted application of the gate locks by the attendant had no effect. If a known level of residual risk is allowed to persist for a long time, the chances of it manifesting itself as an accident or serious incident will inevitably rise. This is what happened at Farnborough North and is why the incident holds a powerful lesson.
This point is not unique to Farnborough North or level crossing incidents. It can be seen over the years in many circumstances and in many organisations. The railway knows virtually all the risks and usually has a good idea of the levels, but sometimes struggles to address them sufficiently, before being caught out by the risk manifesting itself as a significant event.
Why is this? I’d suggest: industry complexity; difficult interaction with third parties; optimism bias; changing spending priorities; an over-belief that the past always predicts the future; waiting for the ‘better’ solution; and rapid turnover of people in certain areas. There will almost certainly be things I have missed, but what that short list shows is that some of these issues are to a degree inevitable. That makes it all the more important to continually re-evaluate residual risk when circumstances change, including an extension of the time the risk is intended to exist. The fact that a residual risk is low does not alter the fact that the longer it is allowed to exist, the more likely it is to manifest itself as an accident or incident of the kind with which RAIB becomes involved.
To conclude, I would like to thank all my colleagues at the Branch, those organisations who assist us and those involved in accidents with whom we interact. Accidents are, by their nature, unwanted and traumatic for those involved. RAIB’s job is to independently investigate accidents to improve safety and to inform the industry and the public. Throughout railway history, the lessons from accidents have driven safety improvements which have in turn made such events ever more rare. It is my sincere hope that our work in 2023 has done that.
Andrew Hall
Chief Inspector of Rail Accidents
May 2024

2. Operational activity
RAIB’s operations are directed by The Railways (Accident Investigation and Reporting) Regulations 2005 (the Regulations). The Regulations describe the types of accidents and incidents the UK’s railway and tramway industries are required to report to us.
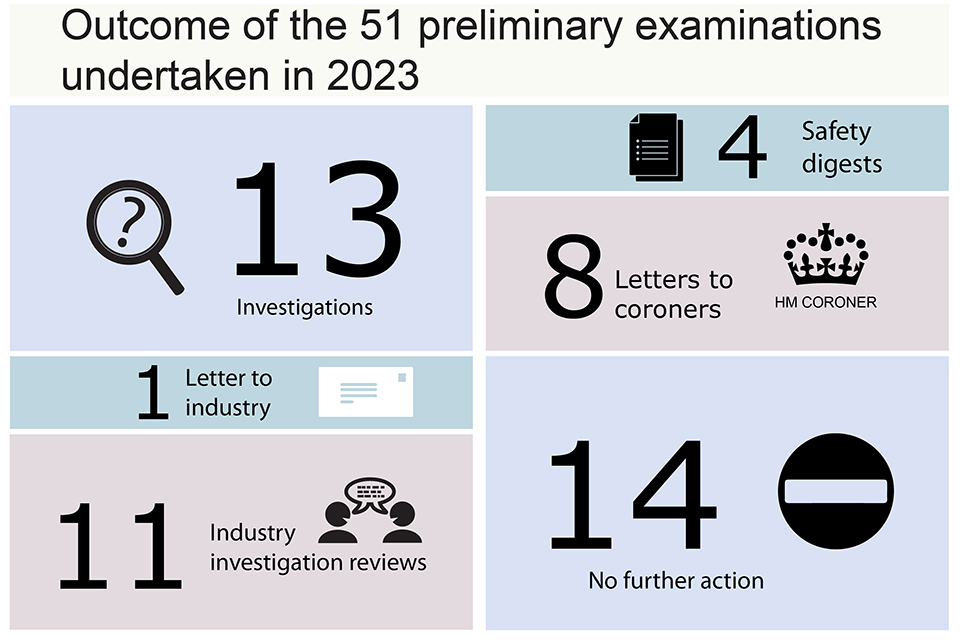
In the operational year 1 January to 31 December 2023, we received 433 notifications. From these we undertook 51 preliminary examinations. Of these, 13 became full investigations with a further 4 resulting in us preparing safety digests to inform the industry. A further 11 preliminary examinations lead to us starting industry reviews, with 8 more being closed by writing to the coroner. Following our initial reviews, we concluded 13 required no further action. One preliminary examination was closed by us writing to the industry.
2.1 Accidents investigated by RAIB
RAIB has a duty to investigate all serious railway accidents as defined by the Regulations. These include derailments and collisions of rolling stock resulting in the death of one person, serious injuries to five or more people, or extensive damage to rolling stock, infrastructure or the environment.
We will also investigate incidents and accidents which, under slightly different circumstances, could have led to a serious accident, and which have an obvious impact on railway safety regulation or the management of safety.
We may investigate other notifiable railway accidents where an investigation will contribute to our mission to improve safety.
If the learning from an accident or incident is widely applicable, but we have covered it previously or it is primarily about compliance, we may choose to produce a safety digest. This is shorter than a full investigation report and includes safety learning but not recommendations.
During the five-year period 2019 to 2023, we started 107 full investigations and safety digests. Eighteen involved railway employees and moving trains (such as accidents to track maintenance workers) and thirteen involved passengers and moving trains (such as a passenger trapped in train doors and dragged). Eleven involved harm, or the risk of harm, to people at level crossings.
We also investigated fourteen derailments (six involved passenger trains and eight involved freight trains), seventeen unauthorised train movements, eleven collisions with obstacles, nine collisions with other trains and six runaways.
| Categories | Full investigations | Safety digests |
|---|---|---|
| Events involving moving trains (staff) (18) | 9 | 9 |
| SPAD or unauthorised train movements (17) | 12 | 5 |
| Events involving moving trains (passengers and members of the public) (13) | 9 | 4 |
| Level crossing accidents and near misses (11) | 7 | 4 |
| Collision with an obstacle (11) | 6 | 5 |
| Collisions with other trains (9) | 8 | 1 |
| Freight train derailments (8) | 7 | 1 |
| Passenger train derailments (6) | 3 | 3 |
| Runaway incidents (6) | 4 | 2 |
| Train defects (4) | 2 | 2 |
| Infrastructure failures (2) | 2 | 0 |
| Near miss - other (2) | 0 | 2 |
3. Northern Ireland and the Channel Tunnel
RAIB did not deploy to Northern Ireland in 2023, nor publish any reports relating to accidents there. However, RAIB has continued to liaise with Northern Ireland Railways (NIR) and the safety regulator, Department for Infrastructure (NI), on matters relating to accident investigation and safety learning.
There were no RAIB deployments to the Channel Tunnel or investigation activity related to it in 2023.
We continue to maintain good working relationships with our counterparts in the Republic of Ireland (Railway Accident Investigation Unit; RAIU), and France (the Bureau D’enquetes sur les Accidents de Transport Terreste; BEA-TT), and with the relevant infrastructure managers, railway undertakings, and safety authorities.
Memoranda of Co-operation (MoC) with RAIU and BEA-TT remain in place covering joint working in the event of a cross-border accident.
The regulatory regime in the Channel Tunnel is currently in transition. Regulatory supervision of the Channel Tunnel is undertaken by the Intergovernmental Commission (IGC) (for the UK part) and the l’établissement public de sécurité ferroviaire (for the French part).
The UK and French governments are working together to agree a Technical Framework Agreement governing the safety and interoperability requirements for railway operations and rail accident investigation in the tunnel, as well as overall governance arrangements.
RAIB and BEA-TT have been party to these discussions and have agreed text for inclusion in the agreement, which will reflect the intent of both bodies to co-operate in the event of an accident or incident. Once this agreement takes effect, ORR will assume the role of safety authority for the UK half of the tunnel. The IGC will continue to carry out its functions under the Treaty of Canterbury and the Fixed Link Concession Agreement.
4. Recommendations
RAIB makes recommendations to industry and other bodies with the aim of improving railway safety. Our recommendations aim to reduce the chance of a similar accident occurring, or to reduce the consequences if such an event were to happen again.
When making recommendations, we identify organisations we consider best placed to implement the changes required. These organisations are referred to as the ‘end implementers’ and include railway, non-railway, private, and public sector bodies.
Most of our recommendations are addressed to the relevant safety authority. For the UK’s railways this is ORR. In Northern Ireland it is the NI Department for Infrastructure (who are advised by HSENI). The safety authority for the UK part of the Channel Tunnel system is the Intergovernmental Commission until ORR takes on this role under the new Channel Tunnel Technical Framework agreement.
If a recommendation relates to an organisation not regulated by the railway industry’s safety authority it can be addressed to any other public body as required.
The law requires that the safety authority ensure that end implementers consider our recommendations and act on them where required. The Regulations require end implementers to provide full details to the safety authority of the measures they intend to take, or have taken, to implement the recommendation.
The safety authority is required to consider each recommendation and action as appropriate. It should also inform us of any measures taken in response to the recommendation, or the reasons why no measures have been taken.
We collect information on actions taken in response to our recommendations. This information is generally based on reports we receive from the safety authority (usually ORR). Any public bodies who are the recipients of our recommendations are required to respond directly to us.
4.1 Current status of RAIB recommendations
The latest status for each recommendation is available in our index of RAIB recommendations. The index provides information as supplied by the relevant safety authority or public body. Each entry is linked to a recommendation status response that provides the full text of each recommendation.
Effective from 1 January 2023, ORR introduced new status definitions to replace those previously used. Responses to recommendations are now categorised as:
Open: Actions to address the recommendation are ongoing.
Closed: ORR considers the recommendation to have been taken into consideration by an end implementer and evidence provided to show action taken or justification for no action taken.
Insufficient response: The end implementer has not provided sufficient evidence that the recommendation has been taken into consideration, or if it has, the action proposed does not address the recommendation, or there is insufficient evidence to support no action being taken.
Superseded: The recommendation has been superseded either by a newer recommendation or actions have subsequently been taken by the end implementer that have superseded the recommendation.
Other recommendations not yet reported on are categorised as ‘Awaiting response’.
4.2 2023 recommendation distribution
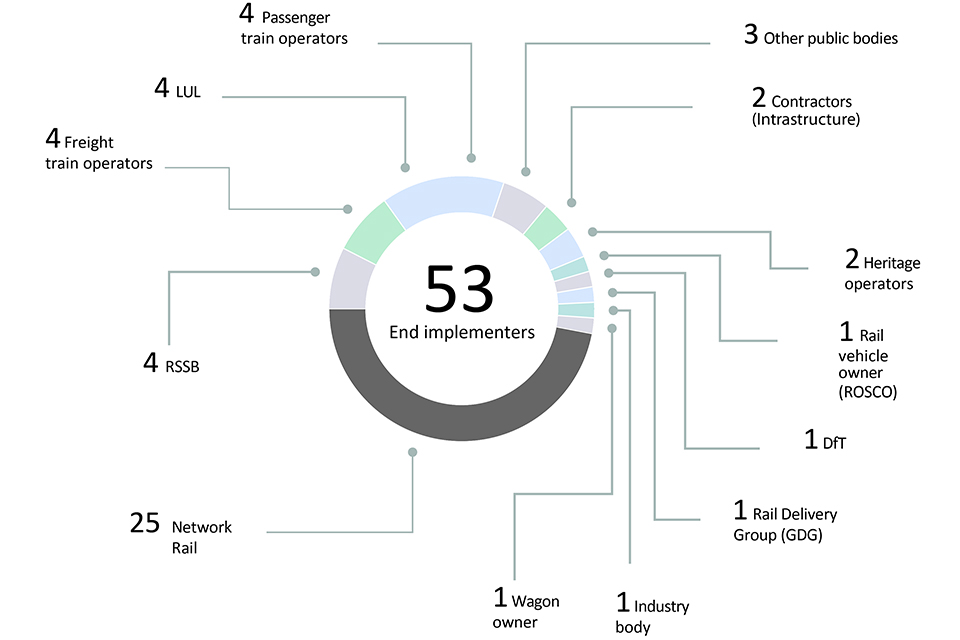
In 2023, we made 49 recommendations directed to 53 end implementers. These included infrastructure owners, train operators, vehicle owners, and other authorities.
In some cases, recommendations were made to more than one end implementer.
4.3 Recommendations
Between 2019 and 2023, we made a total of 259 recommendations. The status of these recommendations was:
- For 20.8 % of recommendations, the safety authority is yet to receive a response from the end implementer (‘awaiting response’)
- For 34.4 % of recommendations, actions to address the recommendation are ongoing (‘open’)
- For 43.6 % of recommendations, ORR considers the recommendation to have been taken into consideration by an end implementer and evidence provided to show action taken or justification for no action taken (‘closed’)
- For 1.2 % of recommendations, the relevant safety authority considers that the response received from an end implementer is insufficient (‘insufficient response’)
No recommendations have been reported as being superseded.
Status of recommendations by the year that they were made (as reported to RAIB by 31 December 2023):
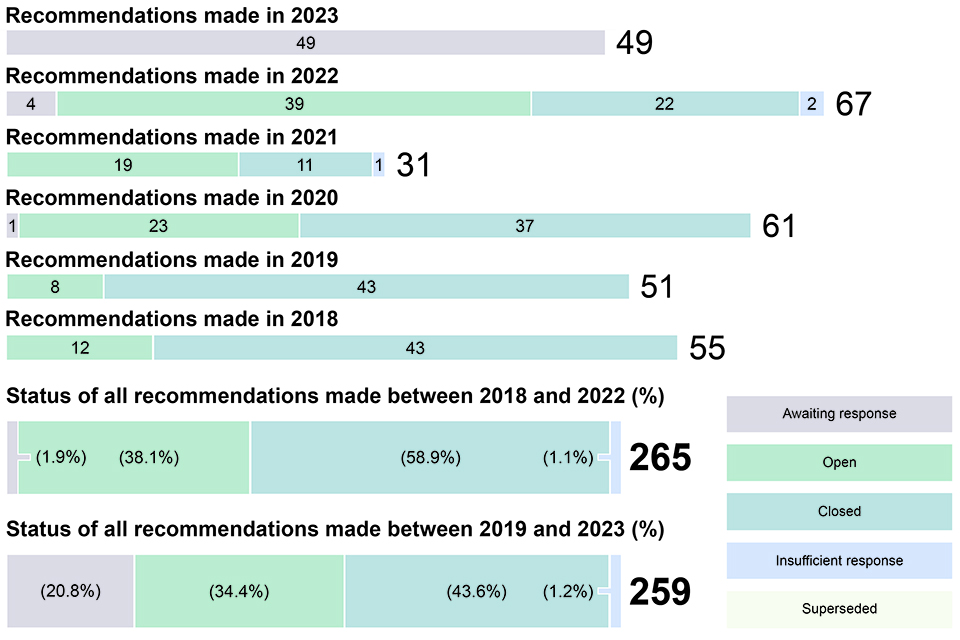
In the five-year period from 2018 to 2022 (that is, those recommendations more than one year old on 31 December 2023) 58.9 % of them have been reported as closed.
4.4 Areas of concern to RAIB
The safety authority, or public body to whom our recommendations are addressed, provides us with updates as to the status of the recommendation. Sometimes, after receiving this response, we may have concerns either about how the organisation has responded to the recommendation, or because of the information we receive from the safety authority.
When this happens, we will discuss our concerns with the safety authority or public body before recording any remaining concerns in the following year’s Annual Report.
When we record concerns regarding the actions taken in response to recommendations, we highlight them according to the following categorisation:
Red – we have concerns that no actions have been taken in response to a recommendation.
Blue – we are concerned that the actions taken are inappropriate or insufficient to address the risk identified during the investigation.
White – we note that substantive actions have been reported but we still have concerns about the underlying risk.
Report 04/2018 – Freight train derailment at Lewisham south-east London
Recommendation 2 – White
Intent of recommendation – The intent of this recommendation is to ensure suitable confirmation that the track is adequately supported, or where this is not possible, that suitable mitigation measures are put in place, in particular following renewal and heavy maintenance, where there has been significant disturbance to the track and ballast.
ORR status – Closed
RAIB concern – ORR reported that Network Rail had undertaken a thorough and detailed review of their control standards and guidance regarding criteria for confirmation of vertical track geometry following track bed disturbance, and mitigation arrangements required when this confirmation is not possible.
RAIB is concerned that this review was limited to Network Rail’s existing standards and that the review concluded that they already require that the vertical track geometry be confirmed under load following all renewal work. The response also appears to still allow a controlled, documented assessment by a suitably certified and competent person as an alternative to measuring/monitoring track under load.
Report 03/2022 – Near miss at Coltishall Lane User Worked Level Crossing
Recommendation 1 – Red
Intent of recommendation – That Network Rail reduces the risk of accidents at vehicular user worked crossings which may see significant use by road vehicle users who are unfamiliar with the crossing.
ORR status – Closed
RAIB concern – ORR reported that Network Rail is satisfied with the robustness of its level crossing risk assessment process and concluded that it is not reasonably practicable to manage safety risk and target safety expenditure based on emergencies/unplanned events such as that which occurred at Coltishall level crossing on 21 January 2021.
To manage the risk of a similar occurrence, Network Rail is engaging with highways agencies to make clear that routes over level crossings of this type should never form part of contingency arrangements for planned diversions.
RAIB is concerned that the intent of the recommendation has been misunderstood by Network Rail, which has solely focused on unplanned events. The recommendation seeks to address the way risks are assessed at user worked crossings which may see significant usage by unfamiliar users due to their location, as well as during unplanned events. None of Network Rail’s current risk assessment mechanisms (such as ALCRM or NRA) currently differentiate between the risks present at crossings used by those who are familiar and/or briefed on the correct way to use them and those which may see significant numbers of unfamiliar users due to their location, such as user worked crossings situated on a public road or a private through road.
Report 18/2017 – Overturning of a tram at Sandilands Junction, Croydon
Recommendation 6 – White
Intent of recommendation – To reduce the likelihood of people being seriously injured or killed by being ejected through tram doors and windows.
ORR status – Closed
RAIB concern – ORR reported that while some tram manufacturers concluded it would be possible to fit laminated glazing to existing trams, it could import risk and engineering challenges associated with significantly increasing the mass of vehicles. A number of operators have chosen to fit a film to the external side of windows. Although this does not offer any improvements in containment, it does offer other safety benefits, such as mitigating the effect of projectiles being thrown at the tram windowpane. ORR stated that the tramway sector has recognised the benefits of improved containment on new vehicles and Light Rail Safety and Standards Board will include enhanced performance requirements for window and door system integrity in new guidance currently under development.
All UK tramway systems have signed up to the new specification when procuring new vehicles. London Trams, the operator of the Croydon tramway, is currently tendering for new trams and has included mandatory requirements for laminated glazing and door retention in its contract specification. It has also fitted thicker film to the doors and windows on its existing tram fleet.
ORR stated that analysis of safety data by the Light Rail Safety and Standards Board showed no incidents that led to an ejection of passengers from a tram following a collision between a tram and a road vehicle. London Trams has also taken action to reduce the risk of trams being struck side on by road vehicles by installing additional road markings, signage and other mitigation measures.
The impracticability and potential negative consequences associated with fitting laminated glazing to existing vehicles, together with more robust risk controls introduced by the tram industry on speed control and driver vigilance aimed at preventing an overturning incident (as a result of recommendations 3 and 4 of the Sandilands report), led ORR to conclude that no further action should be taken in response to this recommendation.
RAIB acknowledges that significant progress has been made in addressing the risks of trams overturning due to overspeed or loss of driver awareness. However, RAIB is concerned that the lack of change in the existing window systems of some tramways means that there remains a risk of people being seriously injured or killed by being ejected through tram doors and windows during other types of accident, such as side impact collisions into trams by road vehicles.
Report 04/2011 – Fatal accident at Moreton-on-Lugg
Recommendation 4 – Blue
Intent of recommendation – To understand the risk posed by the use of non-critical information systems in signal boxes and implement practical mitigation measures.
ORR status – Closed
RAIB concern – ORR reported that Network Rail has identified three measures to address this recommendation. These are: to develop guidelines to help inform decisions about the location of Train Running System on TOPS (TRUST); training on the use of TRUST; training on coping with distraction and interruptions; and implementation of auto-refresh on TRUST.
ORR reported that Network Rail has issued several updated standards. These provide guidelines to inform decisions about the location of TRUST when it is being installed in new locations, as well as revised training on the use of TRUST. The appropriate use of information systems, such as TRUST, is addressed by the workload management and information systems competencies, while coping with distractions and interruptions is further addressed by the attention management competency. These competencies form part of the three-year training cycle for signallers.
RAIB’s concern is that the response is focused on TRUST and that it is not obvious whether the actions would address other similar systems. In addition, the guidelines referred to present a process for managing the ergonomic aspects of a new design and not guidance on the location of TRUST. It is also only applicable to new installations with there being no discussion of existing installations.
RAIB also notes that NR/L3/OPS/045/2.06 does not include any reference on training in the use of TRUST, as stated in Network Rail’s response.
Although the risk assessment produced as part of this work raises the technical integrity of TRUST as a risk, it is not obvious how this risk has been closed out. It also does not appear that the use of non-safety-critical systems to support safety-critical decisions has been recognised in the risk assessment.
It is in addition not obvious whether the issue of signallers being misled by, for instance, out-of-date information has been addressed. Information can be misleading due to delay because of its manual input, as well as the need to refresh the TRUST screen. It appears that the latter has been addressed, but not the former.
Report 09/2022 – Collision between road-rail vehicles near Ramsden Bellhouse
Recommendation 3 – White
Intent of recommendation – To ensure that the provision of obstacle detection technology for on‑track plant is subject to ongoing review as new technology becomes available and/or more cost-effective.
ORR status – Closed
RAIB concern – ORR reported that Network Rail has provided evidence that its plant team regularly review and discuss new systems that have the potential to detect obstacles reliably and consistently, as well as being given demonstrations of new systems by suppliers. Network Rail is also involved in a research project related to autonomous vehicular movement on the rail network and the progress of this research is regularly reviewed for transferable technology and learnings.
RAIB is concerned that Network Rail will continue to review obstacle detection technology for on‑track plant on the ad hoc basis that existed before the accident. This is contrary to the intent of the recommendation, which was that Network Rail adopt a formalised mechanism to require a periodic review of technological solutions.
5. Summaries of learning
Over the years, our investigations have allowed us to gather detailed insights into a range of accidents and their associated causal factors. From this information, we have been able to identify recurring themes and have shared this information with the industry in the form of summaries of learning documents since launching them in 2019.
The current themes we have identified are:
1 - Design and operation of user worked level crossings
2 - Protection of track workers from moving trains
3 - Managing risk at the platform-train interface
4 - Safe management of abnormal train-operating events
6 - Safe design, operation and maintenance of on-track plant and trolleys
7 - The safe management of weather-related events which affect train operation
8 - The integrity of train braking systems
9 - Wrong side failures of signalling
Where appropriate, these have been updated to incorporate learning from 2023.
For 2023, we have added a further topic:
10 - Management assurance
Find out more about each of these topics at: https://www.gov.uk/government/collections/summaries-of-learning
6. Safety and funding
6.1 RAIB’s own safety record
RAIB works hard to ensure we have the highest standards for health, safety, and wellbeing in all aspects of our operations. We review our work and apply any lessons learned from attending site to improve our safety management. We regularly review our office practice and update our health and safety governance arrangements, incorporating learning from accidents and incidents. We did not record any incidents involving our staff in 2023.
As part of this aim to improve, we work closely with external partners, particularly the Air and Marine Accident Investigation Branches. Sharing common lessons learnt and best practice across work areas such as health, safety and wellbeing helps keep both our own team, as well as those we work with, as safe as possible.
6.2 Funding
Our operating budget for the 2022-23 financial year was around £5.1 million.
7. Other activities
7.1 External events
Throughout 2023, we were able to participate in a variety of external events, either in person or virtually. Such participation permits us to reach other areas of the industry and allows us to fulfil our aim of informing the industry and public.
We spoke at Track Engineering, and Earthworks and Drainage events hosted by the Permanent Way Institute (PWI), the IMechE (Scotland), University of Birmingham and University of Cranfield among others.
You can find out more about previous presentations we’ve made at: https://www.gov.uk/government/publications/raib-papers-and-presentations.
7.2 Working with academia
Building relationships with universities specialising in subjects relevant to our investigations helps ensure we keep up to date with the latest scientific developments in fields such as mechanical engineering and human factors.
These relationships have a two-way benefit: as well as offering universities sources for ideas and assistance for student projects in areas that benefit RAIB, our inspectors can provide feedback as well as deliver guest lectures. Some examples include working with University of Cranfield delivering lectures on investigating on-train data recorders.
7.3 Rail accident investigators’ good practice seminar
Following an enforced hiatus in 2022, we were able to host our 5th Railway Accident Investigators’ Seminar in November 2023.
At this year’s event, we hosted guest speakers from Network Rail and The Royal Holloway University of London, along with several of our own colleagues. Topics included investigating the accident at Carmont and the different investigative strands, investigating organisational factors and the effects of weather on railway operations.
Looking forward, we are already planning a seminar for 2024, bringing together guest speakers and investigators from across the industry to both share and learn from collective knowledge and experience.
7.4 The Accident Investigation Chiefs’ Council
The aim of the Accident Investigation Chiefs’ Council (AICC) is to enhance co-operation between the Air, Marine and Rail Accident Investigation Branches. By developing collaborative working practices and joint memoranda of understanding, as well as promoting effective working arrangements with external bodies, AICC works to improve the branch’s effectiveness and efficiency.
AICC comprises a non-executive chair and the Chief Inspectors from the Air, Marine and Rail Accident Investigation Branches.
Find out more about the role of AICC, its terms of reference and its Memorandum of Understanding.
7.5 International relations
RAIB has been a longstanding member of the International Transportation Safety Association (ITSA). ITSA is an international network of heads of independent safety investigation bodies, covering all modes of transport, including aviation, marine, railways, road transport, pipelines, and underground infrastructure.
The membership includes major investigation bodies across five continents, such as the NTSB in the USA and the ATSB in Australia.
Although the UK has left the European Union, we maintain mutually beneficial relationships with the EU National Investigation Bodies and attend their plenary meetings and some subject specific task groups in an advisory capacity.
As in other years, RAIB received a number of requests for advice or assistance from investigation bodies around the world and, if resource allowed, provided it.
8. Table of investigations started, ongoing and published 2023
(Items prefixed with the letter ‘SD’ are safety digests, the remainder are full investigations)
| Event (National Network unless stated otherwise) | Event date | Published | Occurrence type |
|---|---|---|---|
| Collison with a tree at Broughty Ferry | 27/12/2023 | n/a | Collision with an obstacle |
| Fatal accident at Stratford station | 26/12/2023 | n/a | Train movement event involving passengers / pedestrians |
| SD – Train damaged by collision with an object at Highdyke | 19/12/2023 | 17/04/2024 | Collision with an obstacle |
| RRV collision with track trolley at Brading | 22/11/2023 | n/a | Collision with an obstacle |
| Collision between on-track machines near Strood | 16/11/2023 | n/a | Collision between trains |
| Collision at Aviemore station | 29/09/2023 | n/a | Collision between trains |
| Member of staff struck by train at St Philips Marsh depot | 26/09/2023 | n/a | Train movement event involving staff |
| Signal passed at danger at Stafford Trent Valley No.1 Junction | 22/08/2023 | n/a | SPAD or unauthorised train movement |
| SD – Overspeed incidents at blanket emergency speed restrictions between Blackford and Gleneagles | 15/07/2023 | 06/12/2023 | SPAD or unauthorised train movement |
| Tram derailment at Bulwell (Nottingham trams) | 12/06/2023 | 27/03/2024 | Passenger train derailment |
| SD – Overspeed incidents at emergency speed restrictions at Wood Green and Melton Lane level crossing | 11/06 & 12/06/2023 | 05/12/2023 | SPAD or unauthorised train movement |
| Runaway wagon at Kineton | 25/05/2023 | 16/05/2024 | SPAD or unauthorised train movement |
| Uncontrolled evacuation of a train at Clapham Common Underground station | 05/05/2023 | 08/05/2024 | Train movement event involving passengers / pedestrians |
| Train overspeeding incident at Spital Junction | 04/05/2023 | n/a | SPAD or unauthorised train movement |
| Unsafe movement of train at Styal station | 03/05/2023 | n/a | Train defects |
| SD – Passenger dragged at Beeston Centre tram stop (Nottingham trams) | 22/02/2023 | 15/06/2023 | Train movement event involving passengers / pedestrians |
| Trap and drag accidents at Archway and Chalk Farm London Underground stations | 18/02 & 20/04/2023 | n/a | [Train movement event involving passengers / pedestrians |
| SD – Near miss with a track worker at Teignmouth Boat Yard | 14/02/2023 | 24/05/2023 | Train movement event involving staff |
| Train striking debris at Yarnton | 10/02/2023 | 01/02/2024 | Infrastructure failure |
| Serious injury to a passenger alighting from a train at Loughborough Central station (Great Central Railway) | 14/01/2023 | 31/10/2023 | Train movement event involving passengers / pedestrians |
| SD – Near miss with a track worker near Orton Sewer works, Bulkington | 15/11/2022 | 16/03/2023 | Train movement event involving staff |
| Two trains in the same signal section at South Wingfield | 26/10/2022 | 23/10/2023 | SPAD or unauthorised train movement |
| Freight train derailment at Petteril Bridge Junction | 19/10/2022 | 10/10/2023 | Freight train derailment |
| SD – Derailment of a tram near Highbury Vale tram stop (Nottingham trams) | 30/09/2022 | 13/02/2023 | Passenger train derailment |
| Near miss with two track workers at Penkridge | 10/07/2022 | 08/08/2023 | Train movement event involving staff |
| Collision between two freight trains at Loversall Carr Junction | 05/07/2022 | 03/08/2023 | Collision between trains |
| Near miss at Farnborough North footpath level crossing | 19/05/2022 | 24/04/2023 | Near miss – level crossing |
| Pedestrian struck by a train at Lady Howard footpath and bridleway crossing | 21/04/2022 | 06/02/2024* | Level crossing event |
| Train overspeeding at Spital Junction | 17/04/2022 | 10/07/2023 | SPAD or unauthorised train movement |
| Track worker struck by train near Chalfont & Latimer station | 15/04/2022 | 15/05/2023 | Staff accident |
| Embankment washout under a passenger train at Haddiscoe | 30/01/2022 | 27/07/2023 | Infrastructure failure |
| Train driver struck by a train near West Worthing Middle Siding | 01/02/2022 | 16/02/2023 | Train movement event involving staff |
| Freight train derailment at London Gateway | 24/12/2021 | 19/12/2023 | Freight train derailment |
| Collision between passenger trains at Salisbury Tunnel Junction | 31/10/2021 | 24/10/2023 | Collision between trains |
| Buffer stop collision at Enfield Town station | 12/10/2021 | 09/11/2022** | Collision with an obstacle |
| Track damage between Pencoed and Llanharan | 06/03/2021 | 22/02/2023 | Train defects |
*Originally published 14/02/2023. Investigation reopened due to emergence of new information. Updated report published 06/02/2024.
**Report publication delayed due to court proceedings. Report sent to industry 09/11/2022 and published on RAIB website 06/07/2023.
9. Response to RAIB recommendations made in the Carmont investigation
Since the end of 2023, progress has been reported by the industry and ORR has updated its assessment of the status of actions taken in response to RAIB’s recommendations from the Carmont investigation. Below is a summary table showing the status of recommendations based on information provided by ORR up to 31 March 2024.
| Status [footnote 1] | Explanation |
|---|---|
| Open (O) | ORR reports that the end implementer(s) has/have taken the recommendation into consideration and is/are taking action to implement it. |
| Closed (C) | ORR reports that the end implementer(s) has/have taken the recommendation into consideration and has/have taken action to implement it. |
| Rec. | Subject | End implementer(s) |
|---|---|---|
| 1 | Contract and project management | Network Rail (O) |
| 2 | New works and maintenance processes | Network Rail (O) |
| 3 | Drainage design | Network Rail (O) |
| 4 | Mixed cutting examinations | Network Rail / Amey (C) [footnote 2] |
| 5 | Reporting incomplete examinations | Network Rail (C) |
| 6 | Mitigating rainfall-related threats | Network Rail (O) |
| 7 | Control room capability | Network Rail (O) |
| 8 | Management assurance of control room functions | Network Rail (O) |
| 9 | Learning from previous events | Network Rail (O) |
| 10 | Risk assessment of mitigating controls | Network Rail (O) |
| 11 | Route proving trains | Network Rail (C) |
| 12 | Derailment mitigation | Network Rail / RDG (O) |
| 13 | Infrastructure-mounted derailment containment | Network Rail (O) |
| 14 | Lifeguards | HST owners (O) [footnote 3] |
| 15 | Glazing | RSSB (C) |
| 16 | Folding tables | Angel Trains (O) [footnote 3] |
| 17 | Secondary impact protection for drivers | RSSB (C) |
| 18 | Corrosion limits | Owners of MkIII stock (O) [footnote 3] |
| 19 | Pre-1994 crashworthiness | Operators of HSTs (O) [footnote 3] |
| 20 | Fire properties of batteries | RSSB (C) |
-
Effective from 1 January 2023, ORR introduced four new statuses to replace the eight previously used. These are: ‘Open’, ‘Closed’, ‘Insufficient response’ and ‘Superseded’See section 4.1. ↩
-
ORR has accepted Network Rail’s justification for not involving Amey in this recommendation. ↩
-
Recommendations 14, 16, 18 and 19 are being taken forward by RSSB on behalf of industry. ↩ ↩2 ↩3 ↩4