
Annual report for 2019
Published 21 May 2020

© Crown copyright 2020
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/raib-annual-report-published-2020/annual-report-for-2019
Our Purpose:
We independently investigate accidents to improve railway safety, and inform the industry and the public.
1. Chief Inspector’s review of 2019
I am sorry to report that 2019 saw some major setbacks on the path to improved safety for railway employees. In July, all of us at RAIB were shocked to hear that two track workers had been killed by a train at Margam in South Wales. Three men were undertaking routine maintenance activities on a main line that was still open to traffic, and none saw the approach of the train until it was too late. We immediately deployed a team to site and launched our investigation.
Our role is clear, to provide an independent investigation of the factors that led to the accident and the underlying management issues. I am determined that RAIB recommendations will promote the changes that are needed to make track worker deaths a thing of the past.
The year 2019 ended on another sad note with the death of a train driver who was caught between two trains as he walked between them at Tyseley depot in Birmingham on 14 December 2019. On 8 April 2020, RAIB deployed to the site of another tragedy, a fatal accident involving a track worker who was struck by a train near Roade, in Northamptonshire. Our investigations are currently underway.
My thoughts are with all those affected by these terrible accidents.
1.1 Safety of track workers
One hot summer’s day some years ago I attended the site of a fatal accident involving a track worker. I had seen the aftermath of fatal accidents before, and was to see more in my career as an RAIB investigator. However, investigating the death of a fellow railway industry professional had a profound effect on me. The railway is like a family, with a distinct culture all its own, and we all feel deeply the loss of our colleagues. It’s especially traumatic for those who witness such accidents, including workmates and train drivers.
The need to better manage the continuing risk to those who work on the tracks has been reinforced by the tragic death of two track workers who were struck and killed by a train at Margam, near Port Talbot, on 3 July 2019. RAIB has started a detailed investigation into the causes of this dreadful event, and published its interim report on 5 December 2019 (IR01/2019).

There is no great mystery about the areas that need to be addressed to improve the safety of track workers. These have been repeatedly highlighted by 44 investigations carried out by RAIB over the last 14 years. The most obvious need is for smart and accurate planning to reduce the frequency with which trains and workers come into close proximity, while also meeting the need for access to assets on an increasingly busy railway system. Some railways, such as the London Underground and the Docklands Light Railway, already impose much stricter separation between people and trains. Consequently, neither has ever featured in an RAIB investigation in which track workers were at risk from moving trains. Other European railway systems, such as in France, timetable ‘white periods’ in the daytime off-peak hours during which no trains are scheduled to run, so enabling safe access for inspection and maintenance purposes. In other cases, reduced train services are directed over bi-directionally signalled lines, or diverted onto alternative routes, to enable access in daylight hours.
Daytime line blockages for routine inspection and maintenance are hard to come by on the heavily trafficked parts of our national network, and so it is often much easier to arrange safe access to the infrastructure at night, when fewer trains are operating. Despite this, many routine maintenance activities continue to be carried out during the day when opportunities to block the line are much reduced. Cyclical and pre-planned activities, like replenishment of lubricators, continue to be carried out in the middle of the day by a worker who is required to ‘nip in’ between high speed trains, while two or three colleagues are employed to look out. This is not only potentially unsafe, it can be inefficient because the work activity is constantly being interrupted.
The shift away from reliance on lookouts is starting to happen in parts of Network Rail, particularly in the Scotland and LNE Routes. However, there is still a long way to go, and there may well continue to be a need for workers to visit the infrastructure during traffic hours, however they are protected. Instances where this may be unavoidable include observing the track under load and responding to faults. I believe it is essential that Network Rail addresses the fundamental requirements that have been highlighted time and again by RAIB’s investigations.
These include:
- improving the quality of leadership on site, including the identification of site hazards and the local management of risk
- the provision of concise, accurate and relevant information to facilitate orientation and safe decision-making (be it on a sign at the access gate or on a decent line diagram)
- improving the clarity of voice communications
- reducing reliance on the vigilance of individual workers to warn of approaching trains
- greater use of technology to control access to the infrastructure, to provide warnings of approaching trains or protect possession limits
RAIB’s investigations show how important it is that leaders on site are equipped with the social and cognitive skills that are needed to set up and maintain a safe system of work. It is simply not possible for planners to anticipate every problem that the work groups will encounter, and for that reason team leaders need to make the right calls when confronted with the realities of a particular situation. This requires leaders who are equipped with the necessary skills and experience, and sufficient knowledge of the locality, to lead a team in complex and constantly changing circumstances. They also need the ability to communicate clearly, to exercise control and accept challenge from group members who spot that ‘something’s not right’.
So, the railway has a lot to do to cultivate and support a generation of leaders who are able to make a real difference to track safety. We had all hoped that many of these needs would be addressed by the introduction of specially selected ‘safe work leaders’, as part of Network Rail’s ‘Planning and Delivering Safe Work’ initiative. Assurances were given that the industry was moving towards a smaller number of specially selected individuals to consistently provide this quality of site leadership. This goal has yet to be achieved, and was not adequately addressed by the creation of the person-in-charge role in the latest revision of Network Rail’s 019 standard.
Eight months before the accident at Margam, RAIB attended another tragic accident, at Stoats Nest Junction in south London (report 07/2019). This accident was the first in more than four years involving the death of a track worker who was struck by a train. He was employed on a zero hours contract to lay protection at one end of an engineering possession.

For such workers there can be great pressure to try and juggle multiple jobs to make ends meet. The possible effects of such patterns of employment on fatigue and fitness for work are significant. We have therefore recommended that the railway industry reviews the way it manages the use of staff on zero hours contracts, to minimise the risk associated with this pattern of work.
The continuing requirement for people to go onto the track to place and remove red lamps and explosive detonators, as part of the arrangements for protecting engineering work on the railway, is something that RAIB has queried before. Following a fatality at Reading in 2007, and again after a near miss in north London in 2017, we recommended that the railway industry should find ways of eliminating the need for people to be exposed to the risk of being struck by trains in these circumstances. Modern technology means that there are many ways in which the position of trains can be established, and warnings given to drivers and to track workers, if a train movement goes beyond a safe limit. I encourage the industry to continue to try and eradicate the need for Victorian methods of protection on the twenty-first century railway. It is deeply saddening that another person has died while putting down protection for his fellow railway workers - there must be a better way.
Our investigation into a near miss involving a lookout at Peterborough (report 04/2019) revealed a catalogue of problems with on-site organisation and communication. Some of the people involved made incorrect assumptions about what was happening, and the lookout became distracted from the vital duty of warning of approaching trains. The investigation also highlighted the difficulty of managing effective communications between controllers of site safety and the lookouts that they have placed at locations remote from the site of work (this was also a factor in a narrowly avoided collision with a group of track workers at Kirtlebridge in Dumfries and Galloway). For this reason, we have recommended that Network Rail investigates the methods of communication that are actually being used in these circumstances, and implements practical measures that will make life safer for teams working on the track.
I remain hopeful that the rail industry will find a way to address these thorny and persistent issues. There is now a real sense that things must change. We’ve come a long way since the days when fatal accidents involving track workers were commonplace. However, it’s now time for some clear thinking on how best to further reduce the risk to our colleagues who inspect, maintain and renew the railway’s infrastructure. Underpinning all this, there needs to be a culture which absolutely rejects risk-taking as a means of getting the job done.
1.2 Management of stranded trains, and passenger self-detrainment
To be stuck on a train that is not moving can be an unpleasant experience. Add to this a crowded commuter service, limited information and no toilet facilities, and the result is a situation that none of us would want to be part of. Several of our recent investigations have focused on the circumstances which have led some passengers to get out of the trains and walk along the tracks which were still open to traffic, in proximity to a live conductor rail (report 16/2018, report 02/2019, and safety digest 09/2019). As part of these investigations, we considered what could have been done to prevent a relatively minor event involving one train escalating to involve numerous other trains and thousands of passengers. Our investigations highlight the importance of decisive action in the early stages of an incident involving a stranded train.
Our major cities are reliant on rail services to convey many millions of passengers every week, relieving pressure on road networks that are already congested. Achieving this task requires high frequency train services and rolling stock that can convey large numbers of people. Generally, the rail network meets this challenge. However, on such high-density routes, serious delays can themselves be a safety issue if on-board conditions deteriorate rapidly, and frustration and discomfort lead to people taking matters into their own hands, putting themselves at risk of electrocution or of being struck by a train.
Professionalism in railway operations includes the ability to anticipate how a situation may develop. Today, signallers and operations controllers oversee large areas of the rail network, which means that they have the role of front-line managers for incidents like this. It is important that the training they are given equips them for this role. When conditions outside are challenging, and things are not going entirely smoothly, thinking in a more precautionary manner about the possible consequences of a particular train movement may pay dividends.
We are recommending that the railway industry takes action that will minimise the risk of trains becoming stranded, for whatever reason. However, given the range of factors that can disrupt the operation of the railway system, we have also made recommendations which relate to the need for better management of the consequences of a stranded train, so that passengers are kept informed and the railway remains in control of events.
As the railway continues to create signalling centres covering huge geographical areas, and embraces more and more digital technology, its ability to manage operating incidents in an efficient manner should be significantly enhanced. However, I fear that this opportunity will be lost unless the railway develops an overarching ‘control and command’ strategy. Such a strategy could define the ways in which system designers and railway operators jointly address the need for efficient incident management on the modern railway. It should include good practice and high-level principles governing the design and subsequent operation of large control and command facilities, such as signalling centres and operational control rooms.
1.3 Safety at the interface between platforms and trains/trams
Since it was set up in 2005, RAIB has investigated 16 events in which systems have not detected objects trapped in the closed and locked doors of a departing train or tram. In some cases, a limb or item of clothing has been caught in the doors and the people involved have been seriously injured.
A recurrent theme in so many of our investigations is the mistaken assumption that door control systems will always detect the presence of an object. It is therefore disappointing that we continue to encounter train dispatchers (who can be drivers, guards or station staff) who believed that door safety systems would always prevent the train from moving if an object became trapped in the closed doors. Worryingly, this misconception is sometimes shared by more senior members of staff.

These findings reinforce the importance of the final safety check after the doors are detected as closed and before a train or tram continues with its journey. However, they also suggest that it can be very difficult for human operators to effectively monitor repetitive automatic functions such as the operation of train doors, and to reliably spot a dangerous situation that may only occur very occasionally. For this reason, it is important to continue to strive for technology that can detect that people are trapped, or to help the dispatcher to identify that something is going dangerously wrong during dispatch (Notting Hill Gate, report 14/2018 and Elstree & Borehamwood, report 03/2019).
1.4 Safe design operation and maintenance of on-track plant
Getting road-rail plant safely on and off the track ought to be a straightforward business. Unfortunately, over the years RAIB has had to investigate too many incidents in which this operation has gone wrong, and the machine involved has run away downhill, often for quite long distances. Our investigation into a runaway at Bradford (report 01/2019) found that the machine operator’s actions were not in line with what he had been trained to do, and no-one had checked on him. Of greater concern, however, is that the machine’s brakes did not hold it stationary on the 1 in 46 gradient. This was because they were badly maintained, a state of affairs that can be traced back to poor instructions and inadequate supervision of the plant hire company’s maintenance staff.
The management of safety in the rail plant industry is something that RAIB has expressed concern about before. In the past, one of the important issues has been the competence of machine operators and maintainers. In this case, the problems were not only at the plant hire company. The project to convert many road-rail vehicles to direct rail wheel braking also lacked important elements of safety assurance, such as provision for proper information about the machines being converted, and adequate arrangements for training the people who would have to maintain the new braking systems.
Our concern about the operation and design of on-track machines was reinforced by a dreadful accident that occurred at Cholmondeston in Cheshire (report 08/2019), in which a member of railway staff suffered life-changing injuries. The investigation has revealed some alarming weaknesses in the design of railway equipment and the railway’s working processes.

This accident involved a road-rail vehicle that ran into a stationary personnel carrier. The machine was a road lorry that had been converted so that it could be used on both road and rail. Turning the vehicle round while it was on the railway required it to be taken off the track at a suitable location, which was not always easy to arrange. For this reason, the machine was often, as on this occasion, expected to travel a significant distance in reverse. However, the driver’s seating and controls had not been altered, so when the machine was going backwards, the driver had to turn around in their seat to see where they were going (the load of ballast carried by the lorry obstructed any view directly along the track), or rely on signals from a person walking alongside the machine.
Our investigation found that there had been inadequate consideration of the practical aspects of using such a machine on the railway. The Office of Rail and Road (ORR) has promoted the concept of ‘Health and Safety by Design’ to encourage duty holders to choose equipment with intrinsic safety features, and consider the operating conditions at the earliest stages when planning the procurement of equipment. This clearly did not happen in the case of the ballast distributor that was being used at Cholmondeston. We recommended that the industry takes effective action to ensure that its road-rail vehicles can be driven safely to and from the site of work, now and in the future.
Both investigations highlighted the need for the people who operate these potentially dangerous machines to be suitably trained and assessed as competent. It is also important that their compliance with safe methods of operation is monitored from time to time, rather than simply assumed to be correct. However, reliance on the correct implementation of procedures can never be sufficient when the consequences of an error can be so severe. It is for this reason that the design of on-track machines must take into account the reality of operations in a harsh and potentially dangerous environment.
1.5 Safety critical software design
December 2019 saw the publication of our investigation into an incident in which the temporary speed restrictions stored in the signalling system on the Cambrian lines disappeared (report 17/2019). We only decided to investigate this event once it became clear to us that the absence of the temporary speed restrictions had been unknown to the signallers. It quickly became apparent that neither Network Rail nor the supplier of the equipment could explain why a safety critical function of this type had failed in such a potentially dangerous manner.
The lessons from this investigation are important ones for the railway industry. It is fundamental that the process of digital design is robust enough to ensure that software-based systems operate correctly in all reasonably foreseeable circumstances. In this case, the people operating the railway did not know that there was anything amiss. Digital railways need to detect when they have failed and report this to those who need to know: in this case, the signallers.
A software-based system is often made up of a number of ‘black boxes’ which perform particular tasks. It can be hard to know how each of these boxes really works or to fully understand their potential failure modes, particularly when the box has been bought ‘off-the-shelf’ or imported from another application entirely. Once our black boxes have been plugged together, do we really know how they will interact with each other, and with the human operator? Safety critical digital systems don’t often break down – safety critical failures tend to be related to the way they are designed or the way that design has been translated into a working system.
Demonstrating digital system safety can be difficult, but that doesn’t mean that we shouldn’t try to master the problem. Existing industry guidance helps us by breaking the problem down into distinct steps: specification; definition of requirements; design, checking and testing; and validation against the originally specified requirements.
The need for the industry to find ways of improving the way that it manages the implementation of modern software-based systems was reinforced by a major incident that occurred on the national network on 9 August 2019. On this day the National Grid suffered an event leading to the supply frequency of the Overhead Line Equipment (OLE) supply dropping below 49 Hz for approximately 16 seconds. Fifty-seven class 700 trains operating on the AC network north of London responded to the frequency drop by locking out their traction power systems so they became stranded with no air conditioning and reduced lighting.
Twenty-seven of the affected units were recovered using a simple reset process, but this did not work for the other thirty trains which had been ‘updated’ with a software patch. For those trains with this patch, recovery required the attendance of a technician to connect a laptop into the train network and manually restore the traction power system. This unintended consequence of a relatively minor change to the design of the software resulted in massive disruption to the East Coast and Midland main lines for more than seven hours and closed King’s Cross station and part of St. Pancras.
The trains reacted to a reduced traction supply frequency, as intended by the designer (although not as specified by the client). The incident highlights the need for clearer definition of requirements and careful analysis of the consequence of any software changes.
As we move into the digital age it’s vital that the railway industry reviews its role as the client for safety critical software-based systems. Such a review needs to think through the ways in which clients can satisfy themselves that safety requirements for software-based systems are unambiguously defined and take into account the real world needs of the end users. It also needs to consider the best ways in which the clients can assure themselves that the suppliers have properly validated the design against the safety requirements, and the adequacy of current approval processes. This applies equally to the design of new systems and subsequent software modifications.
Improvements to the ways in which the railway industry manages digital risk will involve learning from other industries and co-operation between many different bodies. The railway industry must not shrink from the challenges that this will present, as it will be vital for establishing and maintaining public confidence in the future use of digital systems on the railway.
1.6 The overturning of a tram at Sandilands Junction, Croydon, 9 November 2016
November 2019 was the third anniversary of the tragic accident at Sandilands Junction on the Croydon tramway that led to the death of seven passengers and serious injuries to many more. Our investigation report contained 15 recommendations for the improvement of safety on the Croydon tramway and tram systems elsewhere in the UK.
The UK’s safety regulator for railways and tramways, the Office of Rail and Road, has been monitoring how tram owners and operators have considered and progressed RAIB’s recommendations. ORR has recognised that the far-reaching and cross-sector nature of the recommendations mean that the entire sector needs to work together to develop its understanding of tramway risk and effectiveness of existing control measures. I agree that a collaborative approach is essential, and I am pleased to see that our first recommendation has led to the establishment of a Light Rail Safety and Standards Board (LRSSB). It is important that this body is maintained in existence for the foreseeable future if the benefits of data sharing and closer collaboration are to continue.
With regard to the Croydon system, I am pleased to note the many substantive changes since the Sandilands accident. These include:
- completion of a detailed risk model, a full update of the operator’s route risk assessment and a review of processes for undertaking risk assessments
- installation of a system (PPOS) to prevent overspeeding at high risk locations by automatic application of the brakes, and continual GPS based speed monitoring
- installation of a facial monitoring system to automatically alert drivers when a low level of alertness is detected (which is also being used for the proactive management of fatigue risk)
- improvements to signage, notably on the approach to Sandilands Junction
- improved emergency lighting
- a review of safety management arrangements, including the management of fatigue and steps to encourage the development of an open reporting culture
It’s good to learn from ORR that very real progress is also being made with developing and implementing RAIB’s recommendations on other tramways, including enhanced driver vigilance and automatic braking systems. However, we note that extensive research (by London Trams) has not identified a reasonably practicable way of significantly improving the containment provided by windows on existing fleets of trams - it has been concluded that the level of containment required to mitigate the risk when overturning can only be provided by laminated glass, which would be very difficult to fit to existing trams. While noting the difficulty of retrofitting laminated glass to existing vehicles, RAIB agrees with ORR that more work us needed to evaluate the potential improvements to containment in future builds of trams.
Taken together, the programme of work addressed by UK tramways, both individually and collaboratively through UKTram and the LRRSB, represents a step change in the understanding and control of risk on modern tramway systems. Tram travel remains extremely safe. However, our investigation into an overspeeding event at Middlewood, Sheffield (July 2018, safety digest 10/2018) and a recent event near Bonn in Germany, when a tram ran away for 7 km after a driver collapsed, both serve as reminders of the need to actively manage tramway risk.
See Appendix D for a full update of the status of RAIB’s recommendations following its investigation into this accident.
1.7 To conclude
Sadly, 2019 saw a significant number of investigations involving one or more fatalities. During the year we published four reports relating to fatal accidents (three members of the public and one member of staff) and we are currently investigating three staff fatalities. Our thoughts are with those who have lost their loved ones. As investigators, we are only too aware of the terrible harm caused to families and friends by each of these sudden and unexpected deaths. Our job is to do all we can to explain the sequence of events that led to this loss, to analyse the causes and to make recommendations to prevent a recurrence.
Although our work is often sad and difficult, I continue to be impressed by the dedication and professionalism of our team of inspectors and the vital support teams at RAIB. I am also grateful for the valuable help and support we receive from people and organisations across the railway industry, and the continued positive relationship with the British Transport Police and the independent safety regulator, the Office of Rail and Road.
Simon French
Chief Inspector of Rail Accidents
May 2020
2. Operational activity
The railway industry is required to report certain accidents and incidents to us as set out in the Regulations. We received 381 notifications between 1 January and 31 December 2019, and 51 led us to carry out a preliminary examination of the evidence to determine the most appropriate response.
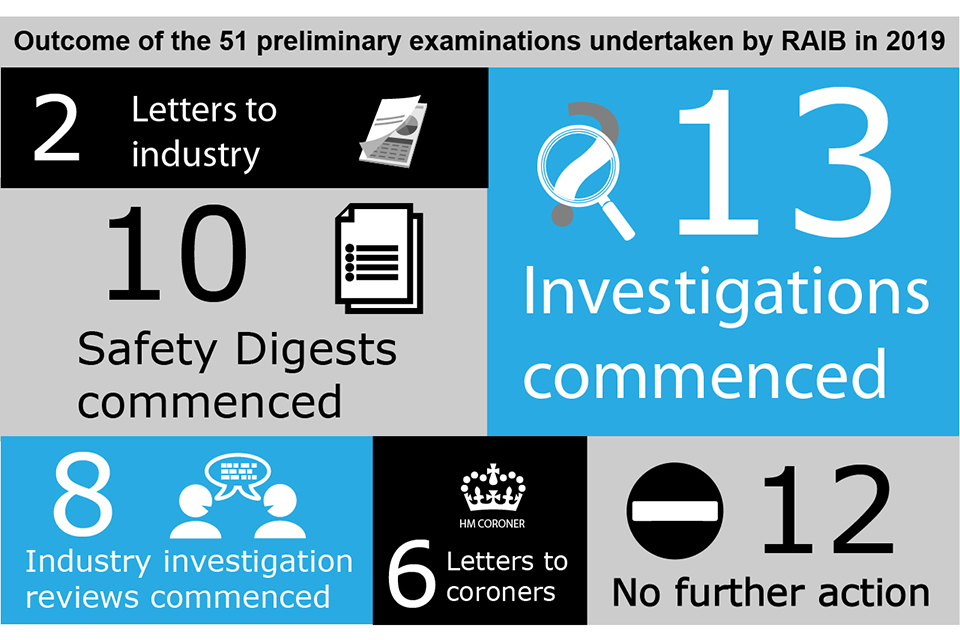
Letters to industry are sent in cases where, following our preliminary examination, we do not believe that there is sufficient potential safety learning to justify either further investigation or the production of a digest. We may then share the evidence that we have collected with the industry parties involved, to assist them with their own investigations into the event. We may also review industry investigations to inform ourselves about the quality of the investigation or technical aspects of the event that it relates to.
More information about safety digests and urgent safety advice can be found at Appendices B and C of this report.
2.1 Northern Ireland and the Channel Tunnel
No investigations in Northern Ireland or the UK part of the Channel Tunnel were carried out during 2019. We continue to maintain contact with the infrastructure managers and railway undertakings as well as with the:
- Department for Infrastructure (Northern Ireland)
- Intergovernmental Commission (Channel Tunnel)
as the respective safety authorities.
2.2 Types of accident investigated by RAIB
We have a duty to investigate all railway accidents in the UK classified as ‘serious’ in the Railways (Accident Investigation and Reporting) Regulations 2005 (the 2005 Regulations). This definition covers all derailments and collisions of rolling stock resulting in the death of one person, serious injuries to five or more persons, or extensive damage to the rolling stock, infrastructure or environment.
We have a similar duty for incidents and accidents which, under slightly different circumstances, could have resulted in serious accidents, and which have an obvious impact on railway safety regulation or the management of safety.
The 2005 Regulations were introduced in response to a recommendation made by Lord Cullen following the Public Inquiry into the collision at Ladbroke Grove in October 1999. However, the regulations also transpose the requirements of the EU Directive 2004/49/EC into UK law.
The European Agency for Railways (ERA) has published guidance to promote consistent categorisation of investigations in accordance with the Directive. We use this to classify our investigations according to Articles 19(1) and 19(2) of the Directive.
- Article 19(1) - a ‘serious’ accident where the investigation is mandatory
- Article 19(2) - an accident or incident, which under slightly different conditions might have led to a serious accident, such as a narrowly avoided serious accident
Table 1 shows the breakdown of accidents and incidents that we have investigated between 2015 and 2019. These are classified as per Articles 19(1) and 19(2). The figures have been collated according to the date of occurrence and not publication of the report.
Table 1: Investigations by category sorted by Articles 19(1) and 19(2)[footnote 1]
| Basis for investigations by the European Railway Safety Directive category | 2015 | 2016 | 2017 | 2018 | 2019 | Total |
|---|---|---|---|---|---|---|
| Article 19(1) | 1 | 5 | 4 | 3 | 4 | 17 |
| Article 19(2) | 20 | 14 | 14 | 16 | 13 | 77 |
| Total | 21 | 19 | 18 | 19 | 17 | 94 |
Appendix A includes details of the investigations commenced and completed in 2019 and the legal basis for the investigation.
The graphic below shows the total number of investigations and bulletins/safety digests started, by type of accident, for the five year period 2015 - 2019.
| Categories | Full investigations | Bulletins / Safety digests |
|---|---|---|
| Events involving moving trains (staff) (21) | 10 | 11 |
| Events involving moving trains (passengers and members of the public) (18) | 15 | 3 |
| Level crossing accidents and near misses (18) | 10 | 8 |
| Collision with an obstacle (14) | 7 | 7 |
| Passenger train derailments (10) | 4 | 6 |
| Infrastructure failures (8) | 8 | 0 |
| Runaway incidents (8) | 5 | 3 |
| Train defects (8) | 6 | 2 |
| Freight train derailments (7) | 5 | 2 |
| Unauthorised train movements (7) | 5 | 2 |
| Collisions with other trains (6) | 5 | 1 |
| Other (5)* | 5 | 0 |
| Near misses (4) | 1 | 3 |
| Signals passed at danger (3) | 2 | 1 |
| Fires on rolling stock (2) | 1 | 1 |
| Class investigations (1) | 1 | 0 |
*Electric shock (near miss); failure of signalling system; unsafe loads
3. Recommendations
We make recommendations with the objective of improving railway safety. Recommendations aim to reduce the chance of a similar accident recurring or to manage the consequences if such an event happened again. We occasionally make recommendations related to the way incidents and accidents are managed.
Recommendations are directed to the organisation we consider is best placed to implement the changes required. These organisations are referred to as the ‘end implementer’ and include railway, non-railway, and private and public sector bodies.
Each recommendation is also addressed to the appropriate safety authority[footnote 2]. If a recommendation relates to an organisation that is not regulated by the railway industry’s safety authority it can be addressed to any other public body (for example the Health and Safety Executive).
On receipt of our recommendations, the safety authority is legally required to ensure that the ‘end implementers’ consider the recommendations, and where appropriate, act on them, as required by the Regulations. The Regulations give the safety authority the power to require end implementers to provide full details of the measures they intend to take, or have taken, to implement the recommendation.
The safety authority is required to inform us, within a period of not more than 12 months, of the measures taken in response to the recommendation, or the reasons why no implementation measures are being taken.
Although we have no statutory powers to enforce the implementation of recommendations, we may consider the actions taken as part of any subsequent investigation.
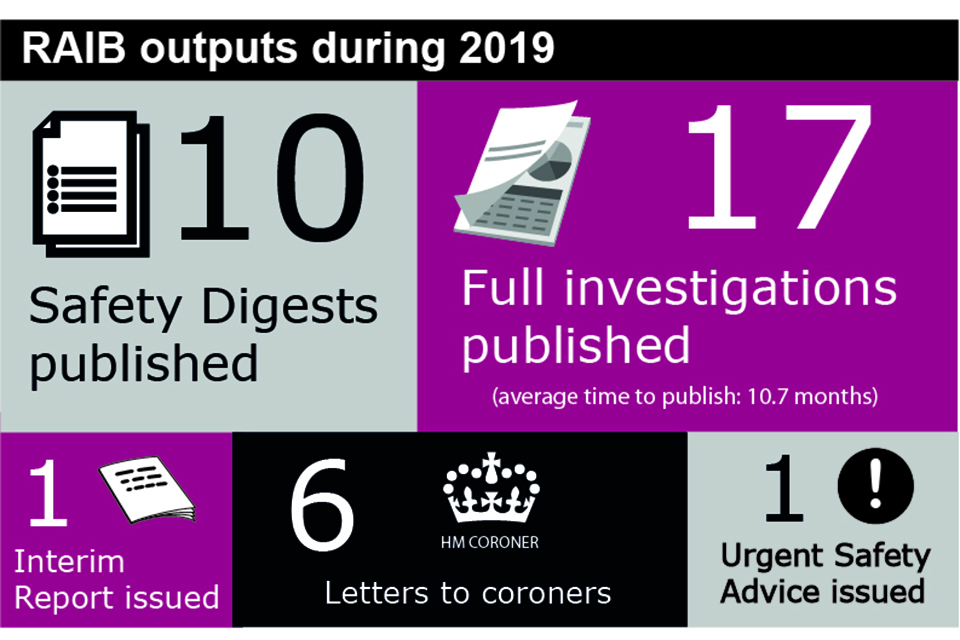
In the 17 reports published in 2019 we made a total of 51 recommendations.
Our Index of RAIB recommendations shows the most up to date status for each recommendation. This information is provided to us by the relevant safety authority or public body. Each entry is linked to a recommendation status report that provides the full text of each recommendation.
The responses are categorised as:
i. Implemented - all actions to deliver the recommendation have been completed
ii. Implemented by alternative means – the intent of the recommendation has been satisfied in a way we did not identify during the investigation
iii. Implementation ongoing - work to deliver the intent of the recommendation has been agreed and is in the process of being delivered
iv. Progressing – the relevant safety authority has yet to be satisfied that an appropriate plan, with timescales, is in place to implement the recommendation; and work is in progress to provide this
v. Non-implementation – recommendation considered, and no implementation action is to be taken
If we are still awaiting an initial report from the relevant safety authority or public body on the status of the recommendation, we categorise it as ‘Awaiting Response’.
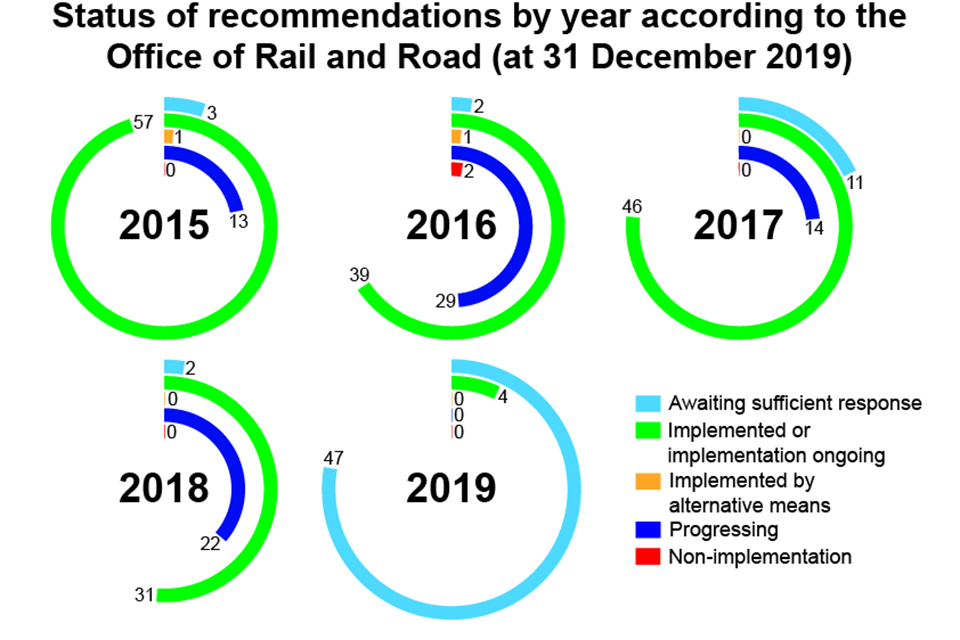
A summary of the status of the recommendations made between 1 January 2015 and 31 December 2019 is shown below.
From now on RAIB’s annual reports will only contain information relating to recommendations that were made during the preceding 10 years. By doing so we hope to focus on what is most relevant at the time. Details of all other recommendations will still be provided in the ‘Index of Recommendations’ which is published on our website.
Reports from ORR show that 77.7% of all RAIB recommendations made since 2009 have either been implemented, or were in the process of being implemented (as of 31 December 2019). A further 2.5% have been recorded as being implemented by alternative means.
In the case of 1.6% of our recommendations the duty holder proposed no action and ORR considers them to be closed, which is classed as non-implementation.
The remaining 18.2% of recommendations remain open because ORR has yet to receive a sufficient response, or because ORR is still considering the duty holders’ response (classed as progressing). However, it is recognised that there is an inevitable time lag between a duty holder reporting the actions taken or planned in response to a recommendation, and ORR reporting to RAIB the outcome. This period of time is required for ORR to consider the appropriateness of the actions, and can sometimes be prolonged if ORR needs further information from the duty holder.
Based on our understanding of the risk, we may have concerns over the way an organisation has responded to a recommendation, or because of information provided to us by the safety authority. When this happens we will raise these concerns with the relevant safety authority. The responses are highlighted with a coloured triangle in the Index.
The classification represented by the triangles is:
Red - We have particular concerns that no actions have been taken in response to a recommendation.
Blue - We are concerned that the actions taken are inappropriate or insufficient to address the risk identified during the investigation.
White - We note that substantive actions have been reported but we still have concerns.
We may also add our own comments and observations which will appear in the recommendation status report.
Those recommendations where the status has changed during 2019, but we have concerns about the response are listed below:
Report no. 20/2018 – Near miss with track workers and trolleys at South Hampstead, London
Recommendation 5 - White
Intent of recommendation – that Network Rail reviews how standard NR/L2/OHS/019 Issue 9 is being applied across its network and takes appropriate actions based on what it finds.
ORR status – Network Rail has not completed the detailed audit required by the recommendation. Nevertheless, ORR has classified the recommendation as ‘implemented by alternative means’ on the basis that two recent Improvement Notices issued to Network Rail by ORR have superseded the need to implement the actions identified by this recommendation.
RAIB concern – RAIB is aware that Network Rail is conducting audits as part of its response to this recommendation. RAIB considers that these audits are still important because:
-
the actions required by the Improvement Notices will take some time to come into effect, leaving a considerable intervening period
-
improvements to track safety arrangements need to be informed by a proper and detailed understanding of how standard NR/L2/OHS/019 Issue 9 is being applied and the reasons for non-compliance
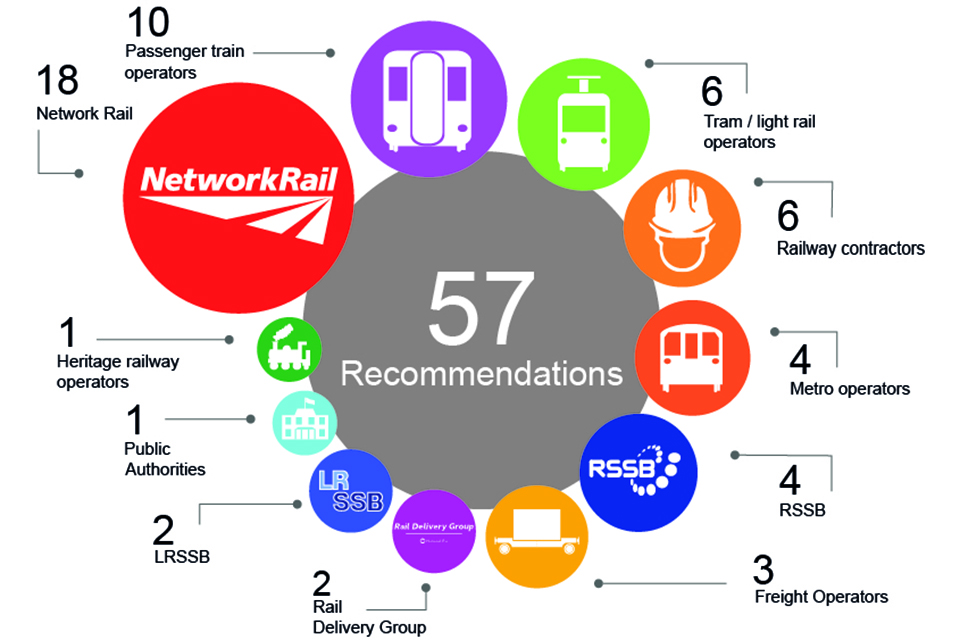
3.1 Recommendations in reports published in 2019
Recommendations in 2019 were made to the following organisations (in some cases they were made to more than one implementer):
3.2 Learning from RAIB investigations
Since becoming operational in 2005, RAIB has published details of 447 investigations (352 full reports and 95 bulletins/safety digests). These describe accidents and incidents of many different types, which have occurred across the whole spectrum of the railway and tramway industry, and throughout the UK. However, there are six categories of event which together make up around 40% of our investigations. We believe the industry still needs to do more work to address the factors which give rise to these accidents and incidents. Summaries of some of the learning which we have identified in these areas are available on our website.
The first involves the design and operation of user worked level crossings and is concerned with managing the interface between road vehicle users and the railway.
Secondly, the protection of track workers from moving trains continues to be of great concern to us, particularly in the light of the deaths of two workers at Margam during 2019.
The third category is about managing risk at the platform-train interface, where we continue to see incidents in which people are trapped in train or tram doors and dragged along the platform.
Category four highlights the fact that recent years have seen incidents which have highlighted the need for the safe management of abnormal train-operating events which put passengers and crews at risk. These happen when trains become stranded between stations because of operational incidents or equipment failures, and passengers are exposed to unacceptable risk in the aftermath.
The fifth area is freight train derailments, which is a problem that has existed for as long as the railways themselves, but where there is still work to be done by the industry to understand and fully address the way in which deficiencies in track and vehicle design, loading and maintenance come together to produce the conditions that lead to accidents.
Finally, the safe design, operation and maintenance of on-track plant and trolleys is an area in which more needs to be done to reduce the possibility that vehicle movements may not be properly controlled, with the risk that this creates of collisions with people and equipment working on the track.
3.3 Other issues of note
Our work covers a wide variety of issues dealing with railway safety. The following investigations published during 2019 have been of particular concern:
Audibility of tram horns (warnings to pedestrians)
- Fatal accident at Saughton foot crossing on the Edinburgh tramway (report 09/2019)
Managing the risk of fog at footpath and user worked crossings
- Fatal accident at Tibberton level crossing (report 13/2019)
Managing the risk to passengers who lean out of train windows
- Fatal accident to a passenger at Twerton, near Bath (report 14/2019)
Managing the risk of excess speed at emergency speed restrictions
- Overspeeding incident at Sandy, on the East Coast main line (report 10/2019)
Protection of trains from large, low and slow-moving vehicles at user worked crossings
- Dangerous occurrence at Bagillt level crossing (report 11/2019)
4. Other activities and information
4.1 International issues
Throughout 2019, RAIB has continued to work with global organisations, sharing our knowledge and experience including:
- attending the International Transportation Safety Association’s (ITSA) annual meeting in Quebec City
- continuing to build working relationships with colleagues at the National Transportation Safety Board (NTSB) in the United States
- providing training and mentoring to the Transport Safety Investigation Bureau (TSIB) in Singapore, which has expanded to include rail within its remit
- supporting colleagues at the Danish Havarikommissionen during its Great Belt (Storebælt) investigation
- the development and evaluation of a pilot trial of human factors training for EU National Investigating Bodies
- co-operating with the Accident Investigation Board Norway following the runaway of a GB designed, manufactured and certified road-rail vehicle (which happened the day before a similar runaway on the GB network which was investigated by RAIB)
Having invested considerable time in building relationships with our European investigation colleagues it is intended to preserve these positive and productive working relationships so far as is possible now the UK has left the European Union.
4.2 Rail accident investigators’ good practice seminar
In November, we hosted our third accident investigators’ good practice seminar which grows year on year. The seminar aims to encourage professionals responsible for rail accident investigation to share and discuss issues and experiences. This year, our own inspectors shared what they had learned during investigations, with the morning session focused on investigating organisational factors.

We were also pleased to have presentations from Network Rail, RSSB, Alstom, East Midlands Trains as well as the Havarikommissionen who shared their own experiences following the Great Belt investigation during the afternoon session.
Planning is already underway for the next seminar.
4.3 Road accident investigation project
We continue to provide support to the RAC Foundation as it progresses its Road Collision Investigation Project (RCIP). The project seeks to establish whether there is a business case for putting more resource into the investigation of road crashes, based on a comparison with the approach to accident investigations used for other modes (rail, air and sea) and safety-critical industries (oil and gas). The project is now at a critical stage and RAIB has been able to assist by releasing an experienced investigator to work with the RCIP team.
4.4 Working with the other Accident Investigation Branches
The Air, Marine and Rail Accident Investigation Branches (AIB) continue to share and develop expertise through working closely in fields of common interest. This covers areas such as electronic data analysis and sharing of equipment to allow rapid and effective investigation of serious accidents, and administrative efficiencies.
The Accident Investigations Chiefs’ Council (AICC) is now fully operational. Comprising a non-executive chair and the three Chief Inspectors, its aim is to promote improvements in effectiveness, efficiency and resilience, and to safeguard the AIBs’ functional independence with their selection and conduct of investigations.
4.5 RAIB’s own safety record
The nature of our work when responding to railway accidents and incidents, can vary in scale, risk and environment. This means our staff can face significant health and safety hazards. We have developed, and continue to update, our own Safety Management System. This includes our health and safety policy and arrangements for how we manage risk. It also sets out a system for the real-time assessment of risk by means of a process known as ‘Dynamic Risk Assessment’.
We monitor our own health and safety performance as an integral part of our management and governance process. We have a Health, Safety and Welfare committee, chaired by the Chief Inspector, which meets periodically to consider any issues raised.
One minor injury to a member of our team and one to a contractor working on site were reported during 2019. One member of the team and one contractor also experienced a near miss. Each of these were recorded and investigated.
4.6 Funding
Our operating budget for the 2019-20 financial year was £5.2m.
4.7 Our ambitions
We aim to be:
- world-class accident investigators, respected and trusted by the industry
- positive, sensitive and efficient in dealing with others, both inside and outside of the organisation
- adaptive to changes in industry, technology and society
We will:
- publish safety learning as quickly as possible to help industry manage any risk
- have a culture of integrity, honesty, objectivity and impartiality
- encourage and help our staff to develop
- act in accordance with the highest professional standards
- deliver good value for money
You can find out more about our role and the legislation which governs our operations at: www.gov.uk/raib.
5. Appendices
5.1 Appendix A - Investigations completed and commenced in 2019
Table A1 lists all RAIB investigations published during 2019. Details of all investigations started by RAIB during 2019 are provided in table A2.
During 2019 we classified our investigations according to Article 19 of guidance published by ERA. This guidance promotes consistent categorisation of investigations in accordance with the Directive. The classifications are:
- Article 19(1) - a serious accident where the investigation is mandatory
- Article 19(2) - an accident or incident, which under slightly different conditions might have led to a serious accident, such as a narrowly avoided serious accident
In both tables, all investigations started under article 19(2) were undertaken on the basis of the potential or actual seriousness of the accident or incident; the schedule 19(1) threshold was not reached.
You can read summaries of all of our current investigations.
Table A1 – Full investigations completed in 2019
| Report Number | Event date | Publication date | Title of the investigation (location) | Occurrence type | Basis for investigation |
|---|---|---|---|---|---|
| 01/2019 | 08/06/2018 | 14/03/2019 | RRV runaway at Bradford Interchange | Runaway incident | 19(2) |
| 02/2019 | 02/03/2018 | 25/03/2019 | Stranding of trains and self-detrainments at Lewisham | Train movement accidents inv pax/pedestrians | 19(2) |
| 03/2019 | 07/09/2018 | 01/05/2019 | Train door accident at Elstree & Borehamwood station | Train movement accidents inv pax/pedestrians | 19(2) |
| 04/2019 | 20/07/2018 | 05/06/2019 | Near miss between a train and a track worker at Peterborough | Staff hit by train (near miss) | 19(2) |
| 05/2019 | 04/09/2018 | 26/06/2019 | Collision between a train and utility vehicle at Dollands Moor yard | Staff hit by train (Injury) | 19(2) |
| 06/2019 | 01/09/2018 | 10/07/2019 | Train travelling with doors open on the Jubilee line | Train defects | 19(2) |
| 07/2019 | 06/11/2018 | 11/07/2019 | Track worker struck by a train at Stoats Nest Junction, near Purley | Staff hit by train (Fatality) | 19(1) |
| 08/2019 | 19/09/2018 | 16/07/2019 | Collision between road-rail vehicles at Cholmondeston | Collision with other train | 19(2) |
| 09/2019 | 11/09/2018 | 25/07/2019 | Fatal collision between a tram and a pedestrian nr Saughton tram stop | Train movement accidents inv pax/pedestrians | 19(1) |
| 10/2019 | 19/10/2018 | 01/08/2019 | Overspeed at Sandy South Junction, Bedfordshire | Unauthorised train movement | 19(2) |
| 11/2019 | 17/08/2018 | 15/08/2019 | Serious operational irregularity at Bagillt user worked crossing | Level crossing near miss | 19(2) |
| 12/2019 | 02/12/2018 | 26/09/2019 | Near miss with a track worker near Gatwick Airport station | Staff hit by train (near miss) | 19(2) |
| 13/2019 | 06/02/2019 | 10/10/2019 | Fatal accident at Tibberton No. 8 footpath crossing | Level crossing accident | 19(1) |
| 14/2019 | 01/12/2018 | 16/10/2019 | Fatal accident involving a train passenger at Twerton | Train movement accidents inv pax/pedestrians | 19(1) |
| 15/2019 | 12/03/2019 | 28/11/2019 | Passenger injury at Ashton-under-Lyne tram stop | Train movement accidents inv pax/pedestrians | 19(2) |
| 16/2019 | 13/03/2019 | 09/12/2019 | Near miss between a passenger train and lorry at Mucking AHB level crossing, Essex | Level crossing near miss | 19(2) |
| 17/2019 | 20/10/2017 | 19/12/2019 | Loss of safety critical signalling data on the Cambrian Coast line | Failure of signalling system | 19(2) |
Table A2 – Full investigations commenced in 2019
| Event date | Title of the investigation (location) | Occurrence type | Basis for investigation | |
|---|---|---|---|---|
| 24/01/2019 | Factors affecting safety-critical human performance | Class investigation | - | - |
| 06/02/2019 | Person struck and fatally injured at Tibberton No: 8 FPC | Level crossing fatality | 19(1) | |
| 12/03/2019 | Person fell on track following tram departure at Ashton-under-Lyne | Train movement accidents inv pax/pedestrians | 19(2) | |
| 13/03/2019 | Near miss at Mucking (AHBC) LC | Level crossing near miss | 19(2) | |
| 16/04/2019 | Brake failure leading to runaway at Beddgelert | Runaway incident | 19(2) | |
| 20/04/2019 | Operational irregularity at Balham | Unauthorised train movement | 19(2) | |
| 06/05/2019 | Freight train derailment, Willesden High Level Junction | Freight train derailment | 19(2) | |
| 17/05/2019 | Near miss between two trams, Manchester | Unauthorised train movement | 19(2) | |
| 13/06/2019 | Train collision with washed-out aggregate, Corby | Infrastructure failure | 19(2) | |
| 03/07/2019 | Fatal accident at Margam | Staff hit by train (Fatality) | 19(1) | |
| 01/08/2019 | Loss of brake control on a passenger train, Edinburgh Waverley | Train defects | 19(2) | |
| 13/11/2019 | Train collision at Neville Hill | Collision with other train | 19(2) | |
| 24/11/2019 | Near miss at Norwich Road level crossing | Level crossing near miss | 19(2) | |
| 14/12/2019 | Fatal accident at Tyseley depot | Staff hit by train (Fatality) | 19(1) |
5.2 Appendix B – Safety digests commenced in 2019
Table B1 – Safety digests commenced or completed in 2019
5.3 Appendix C – Urgent safety advice issued in 2019
We can issue urgent safety advice at any stage during an investigation when we believe there is a need to provide immediate information to the relevant industry bodies about the wider safety issues we have identified.
If the issue affects other European member states, we report the safety advice to ERA via their safety information system (SIS); this action alerts all member states to the advice.
During 2019 we issued one item of urgent safety advice.
| Event date | Event | Urgent safety advice | Date of USA |
|---|---|---|---|
| 11/09/2018 | Fatal collision between a tram and a pedestrian, near Saughton tram stop, Edinburgh | Warning horns on Edinburgh trams | 14/02/2019 |
5.4 Appendix D – Response to RAIB recommendations made in the Sandilands Junction (Croydon tram) investigation
Since the end of 2019, further progress has been reported by the industry and the ORR has updated its assessment of the status of actions taken in response to RAIB’s recommendations. Shown below is an updated summary table based on information provided by ORR to RAIB on 3 March 2020.
| Status | Explanation |
|---|---|
| I - Implemented | All actions to deliver a recommendation have been completed. |
| IG – Implementation ongoing | ORR is content with the proposed action plan to implement the recommendation and the timescale for delivery that has been presented by the end implementer. |
| P - Progressing | ORR is satisfied that the end implementer is taking suitable action to consider and address a recommendation, but a formal completion date has not yet been provided. |
| REC | Subject | Croydon Tram | Other Tramways | ORR |
|---|---|---|---|---|
| 1 | Industry safety body | I | ||
| 2 | Industry review of risk | IG | IG | |
| 3 | Automatic speed control | I | P / I / IG[footnote 3] | |
| 4 | Vigilance devices | IG | IG | |
| 5 | Visual cues | I | IG | |
| 6 | Passenger containment | IG | P | |
| 7 | Emergency lighting | I | P / I / IG[footnote 4] | |
| 8 | Evacuation | I | I | |
| 9 | Regulatory framework | I | ||
| 10 | Independent risk review | I | ||
| 11 | Driver fatigue | I | ||
| 12 | Organisational culture | I | ||
| 13 | Response to safety related reports | I | ||
| 14 | On-tram CCTV | I | ||
| 15 | Maintenance and testing documentation | I |
Summary of the status of actions taken in response to the RAIB’s recommendations (as reported by ORR on 3 March 2020).
-
Figures do not include class investigations (which address more general safety issues). ↩
-
The safety authority is a body responsible for regulating railway safety; for Great Britain this is the Office of Rail and Road (ORR); for the Channel Tunnel it is the Intergovernmental Commission and for Northern Ireland it is the Department for Infrastructure. ↩
-
Progressing at Blackpool and Sheffield. Implementation ongoing at Edinburgh, Manchester and Nottingham. Implemented at Midland Metro. ↩
-
Progressing at Midland Metro. Implementation ongoing at Edinburgh and Nottingham. Implemented at Blackpool, Manchester and Sheffield. ↩