Safe care at home review (accessible version)
Updated 4 July 2023

© Crown copyright 2023
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/safe-care-at-home-review/safe-care-at-home-review-accessible-version
June 2023
Ministerial foreword
Sarah Dines MP, Minister for Safeguarding
‘Home’ should always be a place where people feel safe, and this government is dedicated to ensuring people with care and support needs, who rely on others to help them with their daily activities in their homes, are free from abuse and neglect.
We know that in the vast majority of cases, care and support in the community is provided in wonderful and kind ways that demonstrate the best qualities of our country. However, the passage of the Domestic Abuse Act in 2021 highlighted the need for a more considered review into the protections and support available for victims of abuse in care contexts. This government committed to address this by completing the Safe Care at Home Review to consider how we can continue to protect people from harm.
The Safe Care at Home Review is an important reminder that people with care and support needs may experience abuse and neglect, sometimes under the guise of ‘care’. Older people, or people with disabilities, may be particularly vulnerable to harm because of their dependence on others and the complexity of their care needs. They might rely on other people for physical, mental or financial support, and may face difficulties recognising or reporting harm.
The review draws on a range of evidence, including the Home Office funded Vulnerability Knowledge and Practice Programme, which in recent work has highlighted that one in six domestic homicides involved people who were cared for by, or caring for, the suspect[footnote 1].
We have to work harder together to protect people with care and support needs who are at risk of abuse in their own homes, and to learn lessons to protect society’s most vulnerable. Effective safeguarding requires a whole system, trauma-informed, and person-centred model of care.
Evidence from the review reinforces the importance of this government’s ongoing work to tackle violence against women and girls more broadly. We have already taken steps to address change, including introducing coercive and controlling behaviour as an offence in 2015; passing our landmark Domestic Abuse Act 2021; strengthening guidance on domestic abuse and publishing the ambitious Tackling VAWG Strategy and Tackling Domestic Abuse Plan to help to prevent these crimes, pursue perpetrators and improve the quality of support and range of protections available for victims. In the Tackling Domestic Abuse Plan, we committed to invest £140 million, over three years, to support victims and survivors of domestic abuse and sexual violence.
As Safeguarding Minister, protecting our most vulnerable members of society, improving our understanding of this form of abuse, and delivering a robust response, remain strategic priorities of mine.
This review sets out clear actions requiring cross-government working, to take forward as we continue to build on our existing efforts to improve the system at large, in protecting and delivering quality services to victims and survivors and improving our understanding of this horrific form of hidden abuse.
Helen Whately MP, Minister for Social Care
Any type of abuse or neglect is unacceptable, and this government is committed to delivering an effective safeguarding system so people with care and support needs receiving care in their own homes do so safely, free from abuse and neglect. That is why when this government heard about reports of abuse by people providing care during the passage of the Domestic Abuse Act 2021, we committed to reviewing the protections and support in place for survivors and victims of this abuse.
Following engagement with key safeguarding stakeholders and those with lived experience, I am pleased that we are publishing the Safe Care at Home Review which sets out what we heard and what we plan to do about it.
Ensuring people with care and support needs receive tailored and empathetic care from the comfort of their own home is imperative to maintain their independence.
However, spotting signs of and putting an end to abusive or neglectful behaviours occurring in people’s own homes can be a challenge.
The actions set out in this report show this government’s commitment to protect and empower those who draw on care and support in their own homes, and to those who provide it. As Minister of State for Social Care I am proud to champion the importance of safeguarding people with care and support needs so they can live their lives safely and independently in the place they call home.
We know that the issues highlighted in the report will not be fixed quickly or easily; this report is the start of a journey to highlight and tackle these issues. I am pleased that evidence in the review came from a range of stakeholders, including representatives of deaf and disabled people and carers to begin to understand how abusive environments can be fostered in some care relationships in the home, and protections available to those who experience, or are at risk of experiencing it.
Despite the challenges people working in the social care sector face each day, I continue to be inspired by their commitment to deliver high quality, dedicated care so people with care and support needs have choice, control, and support to live independent lives safely. I would like to thank all the paid and unpaid carers for everything that you do. Where the care provided falls below what we expect, like in the cases we heard about during this review, this report aims to shine a spotlight on it and sets out a plan for improving the system that exists to safeguard against it.
This review goes hand in hand with the government’s wider work to improve adult social care. We have already shown our commitment to adult social care with a historic increase in funding announced by the Chancellor last autumn. We are making available up to £7.5 billion extra investment over two years to support adult social care and hospital discharge. That is the biggest increase ever in social care in England. In addition, we are making major progress on our reform journey, as set out in ‘Next steps to put People at the Heart of Care’.[footnote 2] This includes investing in the workforce, better data and technology, and increasing oversight of the social care system.
Acknowledgments
We are grateful to all the contributors of this review. We would like to thank stakeholders from across the health, housing, social care, academic, criminal justice, and domestic abuse sectors for their involved and honest engagement with the review. In particular, we also express our gratitude to victims, survivors and those with personal experience of abuse in care contexts who participated both directly and indirectly in informing the review.
Executive summary
1. During the passage of the Domestic Abuse Act 2021, concerning evidence was presented by peers and the deaf and disability sector on abuse against people receiving care in their own homes. In response, the government decided to review the existing protections and support for adults with care and support needs who are at risk of, or experiencing, abuse in their own homes by people providing their care. The Safe Care at Home Review (‘the review’) was jointly led by the Home Office and Department of Health and Social Care (DHSC). The review applies only to England, as health and social care is a devolved matter.
2. Abuse or neglect is unacceptable in any context. This review has helped to highlight the issue of identifying abuse or neglect that occurs in people’s own homes and the action that can be taken to prevent this type of abuse from occurring.
3. Millions of adults receive excellent support in their own homes from paid, unpaid and voluntary carers. We know this is greatly valued, helping people with practical day-to-day tasks to live more independent and fulfilling lives. As a government, we want to ensure everyone who is cared for in their own home is treated with dignity and respect. Having heard this is not always the case, we are determined to understand the gaps in the system and address them to ensure everyone receives the quality of care they would want for their own loved ones in their own homes.
4. To gain this understanding the review team engaged with a wide range of stakeholders. Representatives from the Deaf community, older people’s and disabled organisations, people providing care, health and housing professionals, local authorities, social work professionals, Safeguarding Adults Boards, the police, the Crown Prosecution Service and other government departments contributed to this review.
5. This review shows that our understanding of the prevalence and nature of abuse in care relationships is limited. Research in this area can often focus on specific subsets of groups, such as those with disabilities or older people. This evidence may not be generally applicable to all adults receiving care in their own homes. For example, while NHS digital data on safeguarding adults collect data from local authorities on the scale of safeguarding activities, this data cannot be applied as a prevalence measure as not all cases of abuse will be reported.
6. The review heard about the challenges associated with detecting, reporting and investigating abuse in care relationships. These challenges could be explained in many ways: victims’ dependence on carers, the trust they place in carers, the manipulation they experience and the gradual and systematic grooming strategies which some perpetrators employ. In many cases, victims may feel unable to report the abuse as the abuser may be their only way of communicating with the community, or they may feel dependent on the perpetrator for care and support and feel uncertain as to how they would be supported and cared for without the perpetrator.[footnote 3],[footnote 4] Characteristics or conditions such as age, mental illness and disability or dementia or fluctuating mental capacity, may also exacerbate barriers to reporting harm and abuse.
7. The review team heard human stories that brought these challenges to life, such as Honor’s story (case study 1). Stories like Honor’s and others highlight the complexities of identifying and responding to harm that happens behind closed doors and the need for more work to improve our understanding and application of the Care Act 2014 and other relevant guidance and legislation.
8. The review team also heard that harm in care contexts can be far-reaching and in certain cases has grave consequences. For example, research from the Vulnerability Knowledge and Practice Programme Domestic Homicide Project, funded by the Home Office, has found that between 1 April 2020 and 31 March 2022, one in six domestic abuse-related deaths involved carers or people being cared for.[footnote 5]
9. During the course of this review and through extensive engagement, eight findings have emerged. They are divided into the following three themes:
- leadership and accountability
- effectiveness of the local response to abuse in the home
- research, evidence and learning
10. This review makes the case that a stronger response is needed to protect and support people with care and support needs who are at risk of, or experiencing, abuse in their own homes by people providing their care. To begin to address the concerns raised, a set of actions has been developed to address the review findings. These actions are set out throughout the report and summarised in Chapter 6.
Figure 1: Safe Care at Home stakeholder engagement
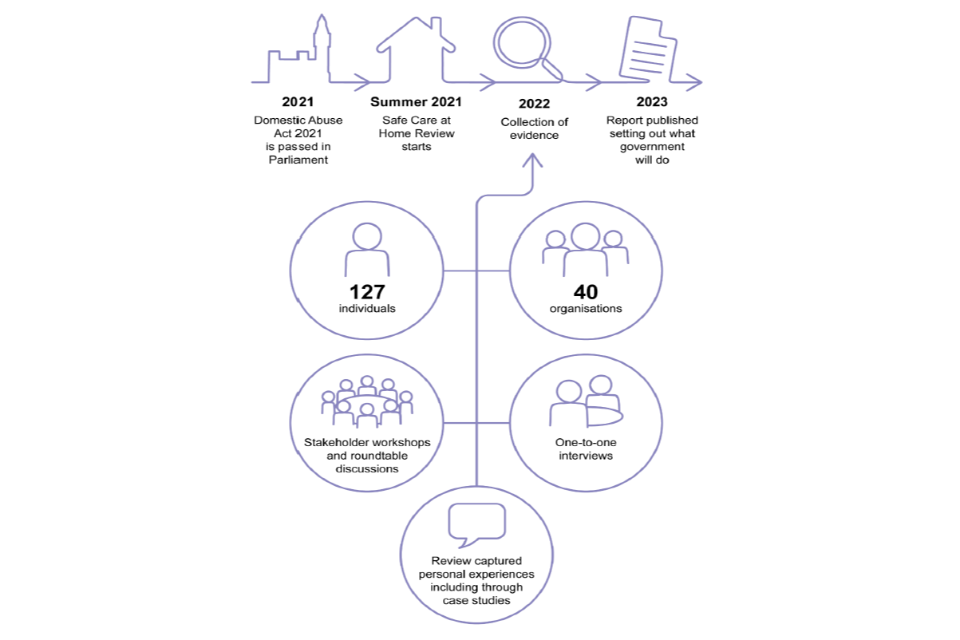
- 2021: Domestic Abuse Act 2021 is passed in Parliament
- Summer 2021: Safe Care at Home Review starts
- 2022: collection of evidence (127 individuals, 40 organisations, stakeholders workshops and routable discussions, one-to-one interviews, review captured personal experiences including through case studies)
- 2023: report published setting out what government will do
Chapter 1: introduction
This chapter sets out the context and the scope of the Safe Care at Home Review.
Context for the review
11. During the passage of the Domestic Abuse Act 2021, evidence was presented by peers and the deaf and disability sector on violence against people receiving care in their own homes, inviting the government to consider whether care relationships should be explicitly covered by the Domestic Abuse Act 2021.
12. The new statutory definition of domestic abuse introduced by the Domestic Abuse Act 2021 incorporates a range of abuse types beyond physical violence, any one of which can constitute domestic abuse if both the victim and perpetrator are “personally connected” (see Annex D). People with care and support needs who are abused by a partner, ex-partner or family member, who is also providing their care, are protected by the Domestic Abuse Act 2021 as they are covered by the “personally connected” definition within the Domestic Abuse Act 2021. However, victims of such abuse by a person providing their care who is not “personally connected” to them, would not be protected by the Domestic Abuse Act 2021.
13. Considering the evidence presented, the government decided that extending the definition of “personally connected” to incorporate all carers – formal or informal – would render the definition too broad, impacting the effectiveness of its implementation, and misaligning the UK with the approach taken to violence against women and girls in the Istanbul Convention, which does not include carers who are not “personally connected” to the victim within its definition.[footnote 6] The Istanbul Convention was later ratified in the UK in July 2022.
14. In response to the evidence presented during the passage of the Domestic Abuse Act 2021, the government committed to review existing protections and support for adults with care and support needs who are at risk of, or experiencing, abuse in their own homes by people providing their care. This is a joint review delivered by the Home Office and DHSC.
15. The review team engaged with a wide range of stakeholders to understand their views on the critical issues surrounding abuse in care contexts. The team spoke with representatives from:
- the Deaf community
- older people
- disabled people
- people who provide care
- health and housing professionals
- local authorities
- social work professionals
- the police
- other government departments
- the Crown Prosecution Service
- Safeguarding Adults Boards
- the Care Quality Commission
16. The review also considered publicly available research and evidence concerning care in the home and abuse within care relationships. Crucially, the review team engaged with and sought the perspectives of experts by experience, including victims and survivors and their representatives. The methodology undertaken for this review is set out in Annex A.
Scope of the review
17. The Terms of Reference for the review were published on 24 February 2022 and set out the aims and scope of the review.
18. The review applies only to England, as health and social care is a devolved matter. However, consideration was given to legislation covering other jurisdictions, such as the Domestic Abuse Act 2021 and other legislation affecting criminal justice which applies to England and Wales. Where relevant, the review points to good practice or lessons learned from examples across England and Wales.
19. The review does not limit the scope of what constitutes abuse or neglect in someone’s own home, as abuse takes many forms including: physical or sexual abuse; economic abuse/exploitation; discriminatory abuse; controlling or coercive behaviour; and psychological or emotional abuse. Abuse in care relationships of all forms is in scope for the review, including domestic abuse where two individuals are “personally connected”, and abuse in domestic settings where two individuals are not “personally connected” (for example, where the individual perpetrating the abuse and providing care is a volunteer or paid care worker). Abuse of carers themselves by cared-for individuals is also touched on but is not the focus of this review.
20. The review focuses on adults over the age of 18. Children and young people have different child safeguarding protections, which are out of the scope of the review. However, the review team noted the significance of leaving care services and the transition to adulthood for those receiving care, as well as applicable ages for key legislation and definitions, such as the Domestic Abuse Act 2021 definition covering victims aged 16 and over. The review team noted people can be cared for by young carers under the age of 18 and that there are issues to consider relating to child to parent abuse, although this was not the focus of this review.
21. Key definitions for the review, as set out in the Terms of Reference, are captured in Annex C.
What is not in scope of the review
22. The review does not include abuse perpetrated in care homes. Concerns raised during the passage of the Domestic Abuse Act 2021 focused on provision of care at home where abuse may be more ‘hidden’ and where there is differing oversight arrangements. Other settings such as prisons, homelessness services or hospitals are also out of scope of the review. Children and young people are out of the scope of the review. Although not in scope of this review, it is recognised there can be risks to people providing care, in particular if the individual they are caring for has complex needs, or in circumstances where the carer is also vulnerable.
Report structure
23. This review first sets out the current context, including the legislation and systems in place to prevent and protect against abuse in the home in the context of a care relationship at present. The report then presents its main findings. These have been organised into three themes:
- leadership and accountability
- effectiveness of the local response
- research, evidence and learning
24. These themes reflect the main findings that stakeholders communicated to the review team as the most pertinent issues requiring policy action.
25. The report also sets out actions that the government will take to address issues that stakeholders raised as part of the review.
26. Annexes A to H supplement the review and contain the following information:
| Annex A | Methodology |
|---|---|
| Annex B | Acronyms |
| Annex C | Definitions contained within the review’s Terms of Reference |
| Annex D | Definition of domestic abuse under the Domestic Abuse Act 2021 |
| Annex E | Eligibility to access care and support under the Care Act 2014 |
| Annex F | Types of abuse and neglect |
| Annex G | Agencies and organisations with safeguarding responsibilities |
| Annex H | Homecare settings |
27. This review includes findings from stakeholders, quotes from individuals with personal experience and case studies presenting real-life scenarios where abuse has occurred. Permission has been obtained from the individuals involved where quotes are included. Accounts have been redacted and pseudonyms have been used in all case studies to protect the anonymity and confidentiality of the individuals concerned. We are grateful to all those who contributed and shared their stories with the review.
Chapter 2: current context
This chapter first explores what care in the home looks like and outlines what we know about who provides care and the nature and prevalence of abuse in this context. A summary of legislation relevant to the review is also provided.
28. The review was carried out in the context of a health and social care system that is under strain and facing significant challenges, including the impact of COVID-19, demographic changes and workforce issues. The government has committed to reforming adult social care in England. In December 2021, the People at the Heart of Care: adult social care reform white paper was published, setting out a 10-year vision for reforming adult social care.[footnote 7]
29. The 10-year reform vision puts people at the centre of adult social care and aims to make sure that people:
- have the choice, control and support they need to live independent lives
- can access outstanding quality, as well as tailored care and support
- find adult social care fair and accessible
30. In spring 2023, the government published a plan for adult social care system reform called the Next Steps to put People at the Heart of Care. This sets out how we will build on the progress so far to implement the vision for adult social care, as set out in the People at the Heart of Care white paper.
Who receives care in their own home?
31. The demand for people needing care is vast and on the rise; almost two million requests for support with adult social care needs (from 1.4 million new clients) were made to local authorities in 2021/22, compared with just over 1.8 million requests in 2015/16.[footnote 8]
32. Anyone can require care and support in their own homes. How this is delivered can depend on an individual’s care needs, where they live and whom they live with. Someone who lives in a rural area may experience care very differently to someone who lives in an urban area. Factors such as the availability of public transport and accessibility to services can make it more difficult for victims in rural areas to report abuse and access support.[footnote 9]
33. The majority of those with care and support needs are older people, however requests for support with adult social care needs among under 65s have been rising steadily since at least 2015/16.[footnote 10] Among under 65s, the most common reason for seeking support in 2020/21 was related to their learning disability at 49%, physical support at 28% and mental health support at 18%.[footnote 11] For people over 65, the primary reason for seeking support was a physical disability (72%) followed by memory and cognition issues (13%).
34. Some people’s support is funded by local authorities under the Care Act 2014 where eligible (see Annex E for further information on Care Act 2014 eligibility). Others fund their own support, completely or combined with local authority support, or rely on support from family and friends. Future plans aim to introduce a lifetime cap on the amount an individual in England will need to spend on their personal care, alongside a more generous means-test for local authority financial support.[footnote 12] Once these reforms are implemented, adult social care will allow more people to receive support from their local authority.[footnote 13]
Who provides care?
35. The Care Act 2014 provides a statutory definition of a “carer”.[footnote 14] However, this review has used the term ‘people providing care’ as an overarching term to capture the following types of groups who may provide care at home:
- “Personally connected” individuals with caring roles. Defined by the Domestic Abuse Act 2021, and includes family members, intimate partners and people who were or are civil partners. Further detail on the definition of “personally connected” can be found in Annex D.
- Unpaid carers (e.g. neighbours or friends) who provide care for someone else.[footnote 15]
- Paid carers: employed care workers, personal assistants, and other paid individuals, in positions of trust, who provide care for an individual.
- Volunteers: individuals who provide care as part of a voluntary organisation.
36. These are not mutually exclusive definitions; different types of ‘care’ can intersect. Volunteers may include individuals who are unpaid to deliver care and might be associated with a voluntary community, and social enterprise sector organisation, local authority, or public service provider. A daughter who provides care for her mother is an unpaid carer who is also “personally connected”. A person may have care provided by family, personal assistants and care workers employed by an agency in the same day or week. In certain circumstances, personal assistants can also be family members that are paid. In some cases, a ‘care relationship’ may involve two individuals with care and support needs, for example, an ‘adult child’ with mental health difficulties being cared for by their elderly mother who may have her own care and support needs. This review considers all forms of care and support in a domestic context, including those who are “personally connected” to the individual with care and support needs, and those who are not.
37. In the context of this review, paid carers include ‘care workers’ employed by a regulated care agency. There is a legal requirement, under the Health and Social Care Act 2008, for service providers to register with the Care Quality Commission (CQC) if they provide or intend to provide an activity that is connected with health or adult social care in England. As part of their role in protecting and promoting the health, safety and welfare of people who use them, the CQC monitors, inspects and regulates health and adult social care services, which are regulated activities under the Health and Social Care Act 2008. This includes personal care that involves supporting people in their homes, including washing, bathing, getting dressed and going to the toilet.[footnote 16]
38. Paid carers may also include personal assistants, who are typically directly employed by individuals with care and support needs and therefore are not under CQC’s remit. Where health and social care activity is carried out by a family member, or by someone with a personal relationship to the person being cared for with no commercial consideration, they are exempt from CQC regulation.[footnote 17]
39. Unpaid carers include anyone who cares, on an unpaid basis, for a friend or family member who due to a condition, frailty, illness, disability, serious injury, mental health condition or addiction, cannot cope without their support to achieve their activities of daily living. Unpaid carers may not always live with the person they care for.
- 4.7 million people providing unpaid care
- 30% of these people provide 50+ hours a week
40. There are a range of estimates of the number of unpaid carers in England. The 2021 Census reported that 4.7 million people in England (8%) said that they provide unpaid care in England. This is 700,000 fewer than at the time of the 2011 Census, where 5.4 million people in England (10%) were found to provide unpaid care in England. This is measured by hours of care provided per week. Of the 4.7 million people providing unpaid care in England, 30% provide more than 50 hours of care per week. Compared to the 2011 Census, the 2021 Census found that there had been an increase in the proportion of unpaid carers providing more intensive levels of care, and a reduction in the proportion providing lower levels of care.[footnote 18] DHSC modelling estimates that there are 2.2 million older people (aged 65 and over) in England in receipt of unpaid care (no data is available on the number of people below 65 in receipt of unpaid care).[footnote 19]
- 2.2 million who are 65+ receive care
41. The Health Survey for England collects information about adults (aged 16 and over) who provide unpaid care. Figure 2 sets out the most common types of care recipients to whom unpaid carers provided care and support to in 2019. It shows that half of unpaid carers reported providing unpaid care to a parent. The second most common response was to provide unpaid care to a partner (18%), and then to a child (14%). Unpaid care can be provided to someone a person lives with, or it can be provided to someone who lives elsewhere. Data shows that 35% of unpaid carers live with the person they care for. Among unpaid carers providing more than 20 hours of care per week, 83% report living with the person they care for.[footnote 20]
Figure 2: Who are unpaid carers providing care and support to?
| Who receives unpaid care | Percentage of people who receive unpaid care |
|---|---|
| Parent | 50% |
| Partner | 18% |
| Child* | 14% |
| Friend | 10% |
| Grandparent | 7% |
| Sibling | 7% |
| Other | 7% |
| Neighbour | 4% |
Please note that groups are not mutually exclusive. The ‘Other’ group includes unpaid carers who responded with ‘Grandchild, including great grandchild’, ‘Other family member’ and/or ‘Someone else’. Source: Health Survey for England, 2019.
*Children are not in scope of the review.
42. People who provide care for more than 35 hours a week, where the person they are caring for gets certain disability benefits from the Department for Work and Pensions (DWP), may be eligible for a Carer’s Allowance. There are 1.3 million people currently entitled to this benefit.
What is defined as care in an individual’s ‘own home’?
43. This review has focused on settings where people are permanently residing in their own home (whether rented, provided by the local authority, or owned). It includes settings where an adult is supported to live independently in supported living accommodation or accommodation with care arrangements, paying either in part or full, towards the tenancy. As set out earlier, care homes, however, are out of scope of this review. For more information on different homecare settings, see Annex H.
What does abuse in a care relationship look like?
44. Both the Domestic Act 2021 statutory guidance and the Care Act 2014 statutory guidance describe a range of forms of abuse that victims may experience. Abuse can include physical, verbal, sexual, emotional, psychological or controlling and coercive behaviour, and economic abuse (for more details on the different types of abuse and neglect, please refer to Annex F). Victims of domestic abuse will often experience more than one form of abuse, particularly where harmful behaviour escalates. [footnote 21], [footnote 22] Multiple forms of abuse can take place all at once or consecutively, and abuse can take place over a prolonged period, often systematically escalating. Although not the focus of this review, there can be risks to people providing care. This is particularly if the individual they are caring for has complex needs, or where the carer is also vulnerable. See Chapter 5 for more information on abuse in the context of domestic homicide research.
45. In care relationships, deciding what is deliberate abuse, neglect or inadvertent harm may not be clear-cut. This makes it all the more challenging to detect, report and investigate. This may be the case not just for professionals but also for the people experiencing the harm, who may not recognise themselves as victims. This could be due to a number of factors, such as: the victims’ dependence on their carer; the trust they place in their carer, the manipulation they experience; and the gradual and systematic grooming strategies which some perpetrators employ. In many cases, victims may feel unable to report the abuse as the abuser may be their only way of communicating with the community. They may feel dependent on the perpetrator for care and support and feel uncertain as to how they would be supported and cared for without the perpetrator.[footnote 23] Characteristics or conditions such as age, mental illness, disability, dementia or fluctuating mental capacity may also exacerbate barriers to reporting harm and abuse.[footnote 24]
46. Financial and economic abuse is becoming increasingly reported on across society, with older people and people living with disability appearing to be most at risk.[footnote 25] A literature review by Age UK on financial abuse has suggested that the prevalence of financial abuse for those aged 65 or over is 1.2% of the population and that in 2015 there were roughly 130,000 people living at home who have suffered financial abuse at some point since turning 65.[footnote 26]
47. Perpetrators may exploit their position to keep the abuse hidden. They may use strategies such as appearing like someone who is simply ‘taking care of their loved one’ or acting in the victim’s ‘best interests’.[footnote 27] Perpetrators may abuse victims by specifically exploiting their care and support needs.[footnote 28]
Case study 1: ‘Honor’s story’– challenges in responding to reports of abuse, recognising abuse and barriers to making disclosures. [footnote 29], [footnote 30]
Honor was a 90-year old widow living with her middle-aged son in her own home. In June 2014, Honor’s daughter reported concerns about her mother’s welfare. She was worried that her mother may have been a victim of financial abuse by her brother, Honor’s son.
Honor’s daughter continued to raise concerns about her mother’s treatment by her brother. In response, the GP, Community Care and Safeguarding Team made repeated attempts to encourage Honor and her son to engage with social care services for support.
In 2015, Honor was seen by a mental health team and she disclosed that she felt intimidated by her son. The mental health worker reported this to the Enquiry Officer, but this did not lead to an alert being raised with safeguarding, as it should have been, because it was not regarded as new evidence of abuse.
Although Honor disclosed that she felt intimidated by her son, she did not allege psychological abuse or neglect by him and refused assistance from community care. Between June 2014 and December 2016, six safeguarding referrals were made by different people including Honor’s daughter, a friend, and voluntary organisations. However, Honor continued to deny the alleged abuse.
In December 2016, following a visit by the GP and a domestic abuse charity, Honor disclosed psychological abuse.
Therefore, despite the reports of abuse being flagged by her daughter in 2014, Honor felt unable to disclose that she was a victim of psychological abuse for a period of over two years. When Honor felt able to disclose the abuse she was experiencing, it was her GP she felt comfortable reporting to, rather than the police or another statutory safeguarding agency.
Scale and nature of abuse in care relationships
48. Our understanding of the prevalence and nature of abuse in care relationships is limited. Research studies in this area often focus on specific groups such as those with disabilities or older people, rendering the findings from such studies ill-suited to generalisation. The limitations of our understanding of both the scale and nature of abuse in care relationships is also covered in Chapter 5.
49. NHS Digital data on safeguarding adults brings together data collected by local authorities demonstrating the scale of safeguarding activities taking place at both regional and national levels in England.[footnote 31] The data cannot be considered as a measure of prevalence, as not all cases of abuse are reported. The data does however provide an indication of the scale and nature of abuse in care relationships. There were an estimated 541,535 concerns of abuse raised over the period from April 2021 to March 2022, an increase of 9% on the previous year. The data does not indicate the relationship between the perpetrators and victims beyond stating whether the source of risk was the service provider, ‘other – known to individual’, or ‘other – unknown to individual’.
- 541,535 safeguarding concerns year ending March 2022
- 161,925 safeguarding enquiries year ending March 2022
50. When a safeguarding concern has been raised about an adult in its area, the local authority has a duty, under section 42 of the Care Act 2014, to carry out a safeguarding enquiry if the adult has care and support needs, appears to be at risk of, or experiencing, abuse or neglect and as a result of those needs is unable to protect themselves.
51. In the year ending March 2022, there were 161,925 section 42 enquiries, an increase of 6% from the previous year. We do not know if this increase is the direct result of an increase in safeguarding concerns or a result of agencies and the public reporting more regularly. The majority of individuals involved in section 42 safeguarding enquiries were aged 85 and over (approximately 1 in 40 adults). The most common location of the risk was the person’s own home (48%).
Figure 3: Most common location of risk of Section 42 enquiries in England, year ending March 2022
| Location of risk | Count of concluded section 42 enquiries |
|---|---|
| Own home | 75,490 |
| Care home - residential | 36,010 |
| Care home - nursing | 15,015 |
| Other | 9,405 |
| In the community (excluding community services | 6,510 |
| Hospital - acute | 5,455 |
| Hospital - mental health | 5,120 |
| In a community service | 4,075 |
| Hospital - community | 1,610 |
Source: NHS Digital. 2022. Safeguarding adults, England.
52. The most common type of risk in section 42 enquiries that concluded in March 2022 was neglect and acts of omission, which accounted for (31%) of risks. Followed by physical abuse (19%) and psychological abuse (14%). Six percent of section 42 enquiries were classified as a domestic abuse risk. Most (51%) section 42 risks were raised by ‘other - known individuals’, such as a family member or a friend, while 34% were identified by service providers and 15% by ‘other - unknown individuals’.
Existing protections available to adults who are at risk of, or experiencing, abuse or neglect in their own home by the people providing their care.
The Care Act 2014, section 42 and related statutory guidance
53. Existing protections available to adults who are at risk of, or experiencing, abuse or neglect in their own home by the people providing their care are underpinned by the Care Act 2014 and the Care and Support statutory guidance, along with other legislation as set out in Figure 4.
54. Under section 42 of the Care Act 2014 (set out in the previous page), the local authority has a duty to carry out safeguarding enquiries where it has reasonable cause to suspect that an adult in its area:
- has needs for care and support (whether or not the authority is meeting any of those needs)
- is experiencing, or is at risk of, abuse or neglect
- as a result of those needs, is unable to protect himself or herself against the abuse or neglect or the risk of it
55. If the local authority has reasonable cause to suspect that an adult in its area meets the criteria set out under section 42 of the Care Act 2014, then the local authority must make (or cause to be made) whatever enquiries it deems necessary to decide whether action should be taken under Part 1 of the Care Act 2014 or otherwise. If action is required, the local authority must decide what action should be taken, and by whom. The Care and Support statutory guidance supplements the Care Act 2014 and explains the approach to safeguarding in depth, including endorsing the Making Safeguarding Personal which is a person-led and outcome-focused approach to safeguarding.[footnote 32]
56. The Care and Support statutory guidance also states that local authorities should have a qualified and registered social work professional practice lead, known as a Principal Social Worker (PSW), to lead and oversee social work practice, including ensuring the quality and consistency of social work practice in fulfilling its safeguarding responsibilities.[footnote 33] As part of their role, the PSW must advise the Director of Adult Social Services and/or wider council in complex or controversial cases. The PSW should have extensive knowledge base on safeguarding, Making Safeguarding Personal, and must be confident in its application in their own and others’ work.
57. A new duty on the Care Quality Commission (CQC) to assess local authorities’ delivery of their Care Act 2014 duties went live on 1 April 2023. This includes the CQC assessing how local authorities undertake and deliver their safeguarding duties. In making these assessments, the CQC will consider a range of evidence including people’s experiences, feedback from staff, leaders and partners, and the impact of safeguarding policies and processes.
Safeguarding Adults Boards and Safeguarding Adults Reviews
58. Section 43 of the Care Act 2014 requires each local authority to set up a Safeguarding Adults Board (SAB). A SAB includes three statutory core members: the local authority, the Integrated Care Board and the police.[footnote 34] The purpose of a SAB is to help and support adults in its area who fall within the criteria set out under section 42 of the Care Act 2014. The SAB must lead adult safeguarding arrangements across its locality and oversee and co- ordinate the effectiveness of the safeguarding work of its member and partner agencies. As part of this, a SAB must arrange for Safeguarding Adults Reviews to be carried out in cases involving adults with needs for care and support in circumstances where:
- (1) the SAB knows or suspects an adult has experienced, or is experiencing, serious abuse or neglect; or
- (2) where an adult has died, and the SAB knows or suspects the death resulted from abuse or neglect (whether or not they knew this at the time of death)
59. The aim of the Safeguarding Adults Review should be to identify the lessons to be learnt from these cases to prevent future abuse and deaths arising from abuse or neglect. This is similar to the aim of Domestic Homicide Reviews.[footnote 35]
Carer assessments
60. The Care Act 2014 also exists to support carers (as defined within the Act). Local authorities are required to undertake a carer’s assessment of any carer who appears to have a need for support. This is an opportunity to record the impact that caring has on a carer and to look at the carer’s specific needs, including assessing whether or not they are willing or able to continue caring. If a carer is assessed as having needs that are eligible for support, then the local authority is required to meet those needs and to draw up a support plan with the carer setting out how those needs will be met.
Key policy and legislative milestones in this area
61. Beyond the provisions set out in the Care Act 2014, there are other key legislative instruments which provide protections for people with care and support needs (see Figure 4).
Figure 4: Other key legislative milestones relevant to the Safe Care at Home Review
2005: Mental Capacity Act
Protects and empowers people who may lack the mental capacity to make their own decisions, including about their care and treatment.
2008: Health and Social Care Act
Established the CQC as an independent regulator for registration and inspection of health and adult social care services to ensure safety and quality of care.
2014: The Care Act
Places the safeguarding of adults with care and support needs from abuse and neglect on a statutory footing.
2015: Criminal Justice and Courts Act
Introduces criminal liability where a person has been placed under the care of a care worker such as in a hospital or care home and there has been ‘ill treatment’ or ‘wilful neglect’.
2021: Domestic Abuse Act
Introduces a statutory definition of domestic abuse, including economic abuse. Domestic abuse is defined in the context of “personally connected” individuals.
2022: Health and Care Act
Transforms how NHS England is organised, seeking to improve health and care service outcomes and to improve integration strategies.
62. As set out in the Terms of Reference, this review sought stakeholder views about how these protections differ for people with care and support needs at risk of, or experiencing, abuse, where the abuser falls within the scope of the Domestic Abuse Act 2021 and where they do not. The majority of stakeholders said that all adults with care and support needs should be protected by existing legislative provisions (either by the Domestic Abuse Act 2021, where the perpetrator is “personally connected” to the person receiving care, or by the Care Act 2014, where the perpetrator is not). Stakeholders made clear that a key issue leaving individuals at risk of abuse is the inconsistent application and cross-professional variation in understanding of the existing legislation, rather than specific legislative gaps, such as the scope of the Domestic Abuse Act 2021. Therefore, although the review considered legislative protections available, this has not been reflected as a key finding, as it was not identified by stakeholders as a key issue.
The role of the Disclosure and Barring Service (DBS)
63. Employers and other providers of regulated activity can make referrals to the DBS where there are concerns about individuals falling short of professional standards. Where the DBS determines that someone has met the ‘risk of harm’ threshold, the DBS may choose to add individuals to its children or vulnerable adults ‘barring lists’, which prevent individuals from working with children and vulnerable adults in regulated activity.[footnote 36] It is unlikely, however, that informal or unpaid carers would come to the attention of the DBS, by virtue of not being specifically employed by a care provider.
64. In a context where the person providing care is employed or contracted by an agency, carers would be eligible for the enhanced DBS and barred list checks. A local authority or Integrated Care Board may add conditions such as a DBS check as part of its risk assessment of safeguarding when they are engaging with organisations that oversee people working as personal assistants.
65. A person with care and support needs who directly employs a personal assistant cannot request enhanced DBS checks. Self-employed people are unable to apply directly to the DBS for a standard or enhanced criminal record check, regardless of the activity being undertaken. Self-employed individuals can, however, apply for a basic DBS check, which will reveal any unspent criminal convictions and adult cautions, which those using their services may ask to see. People who are cared for by family members or others who are “personally connected” are therefore not protected through DBS checks or referrals processes.
How are risks being assessed?
66. All care assessments and carer assessments should include a holistic and comprehensive overview of risk of harm that is live to changing circumstances. When the local authority is informed that someone living in their area with care and support needs may be at risk of abuse or neglect, then the safeguarding provisions of the Care Act 2014 will apply.
67. Although DWP has no legal duty to ‘safeguard’, the department does have a role in supporting people providing care and receiving care. DWP informed the review that when they become aware of a serious concern for the safety and wellbeing of someone in a care relationship, they can raise this with relevant local authorities to ensure that issues are addressed appropriately. For example, if a person receiving Universal Credit writes in their journal (an online messaging service used to communicate with DWP) that they are being harmed, this can be picked up by the system.
68. High-risk cases where the abuse is perpetrated by someone “personally connected” to the victim, and which are therefore considered cases of domestic abuse, may be referred locally to Multi-Agency Risk Assessment Conferences (MARAC).[footnote 37] Specialist domestic abuse support workers are highly trained to support families affected by domestic abuse and contribute to discussions and risk assessments involved in Multi-Agency Safeguarding Hubs (MASHs).[footnote 38] Police and other professionals may use risk assessment tools like the Domestic Abuse, Stalking and Harassment assessment tool or the Domestic Abuse Risk Assessment tool which has an increased focus on identifying signs of coercive control. [footnote 39], [footnote 40], [footnote 41]
69. In cases of abuse that do not involve a ‘personally connected’ relationship, where the perpetrator for example may be a care worker, personal assistant or friend, local authority safeguarding teams have a statutory duty to make enquiries about safeguarding concerns under the Care Act 2014. The decision as to which agency should lead and which tools to use may depend on the what the victims’ care and support needs are.
Chapter 3: leadership and accountability
This chapter explores the first of three main findings that emerged from the evidence collected during the course of this review, which centred around leadership and accountability. The findings set out in this chapter are:
- i. Oversight of safeguarding in England is fragmented and there is limited accountability.
- ii. Competing pressures and insufficient resources available have a negative impact on the safety of the people with care and support needs.
- iii. There is limited sharing of information and learning from best practice and failures.
Oversight of safeguarding in England is fragmented and there is limited accountability.
70. Although there are a number of agencies and frameworks in place to protect the safety of people with care and support needs (see Annex G), the review team noted that stakeholders from across the board perceived there to be a lack of national and local oversight and accountability of safeguarding functions in England.
71. Statutory responsibility for adult safeguarding sits with local authorities, as set out in the Care Act 2014, while at a national level, there is shared oversight responsibility. DHSC is responsible for setting national policy and the legal framework for adult social care. The Department for Levelling Up and Housing and Communities oversees the distribution of funding to local government, as well as the financial framework in which local government operates. The Care Act 2014 sets out the law on how adult social care in England should be provided and provides the legal basis for local authorities to arrange social care for individuals; to manage supply and demand in their local market; and to interact with sector partners. Policing and health have their own oversight bodies and other arm’s length or regulatory bodies, such as the CQC and NHS England, which are operationally independent but accountable to Ministers and to Parliament. A full list of government bodies and regulators that have a role in safeguarding can be found in Annex G. It is worth noting that community safety, children’s safeguarding and Safeguarding Adults Boards (SAB), together with other local partnerships, play an important role in local safeguarding arrangements.
72. Stakeholders such as academics, charities, and representatives from the police and social care professions felt that it was unclear who holds strategic oversight of the safeguarding of adults with care and support needs, at both local and national levels. The review heard that more needs to be done to hold organisations and agencies to account at a national level to ensure that lessons are being learned from safeguarding failures.
73. A number of stakeholders including SAB Chairs, academics and safeguarding practitioners also expressed concerns about an over-reliance on sector-led change across agencies. Stakeholders described a system which relies heavily on the will of individuals rather than strategic direction to best meet the needs of people receiving care in England and to protect them from harm and abuse.
74. To address accountability concerns, stakeholders want to see increased cross-government and multi-agency working, among organisations with safeguarding responsibilities for protecting people with care and support needs in England. Most stakeholders highlighted the need for leaders at both a national and local level to create more robust systems and mechanisms for accountability. This would serve to shift responsibility away from informal, sector- and individual-led improvement approaches to a more clearly formalised leadership and accountability approach.
75. Stakeholders informed the review team that there needs to be strengthened oversight and accountability mechanisms of safeguarding people with care and support needs who receive care at home. This would improve the coherence of the response to this type of harm and better protect and support victims of abuse and neglect with care and support needs.
What will government do?
- a) DHSC and the Home Office will encourage the Domestic Abuse Commissioner, the Victims’ Commissioner and the Chief Social Worker, to review, promote and disseminate best practices concerning the protection of people with care and support needs – specifically those who are at risk of being abused in their own home by the people providing their care.
- b) DHSC will review sections of the Care Act 2014 guidance covering safeguarding roles and responsibilities, identifying opportunities to clarify the roles and responsibilities of government departments and statutory agencies, and rights and redress for victims and survivors. If changes to statutory guidance cannot be prioritised, DHSC will explore opportunities to develop or amend non-statutory guidance.
- c) DHSC and the Home Office, working with the Chief Social Worker, will regularly bring together representatives from across government to promote better join up between departments with oversight responsibilities and monitor the progress of actions from this review, leveraging existing governance where appropriate. Attendees of this new cross-government meeting may include members of the DHSC Adult Safeguarding Forum, chaired by the Chief Social Worker and Chief Nurse convening key representatives of organisations with safeguarding duties (local authorities) and responsibilities (including the CQC, police and the NHS).
Competing pressures and insufficient resources have a negative impact on the safety of the people with care and support needs and exacerbate pressures on those delivering care.
Often safeguarding concerns are never responded to. Even on the rare occasions a person can speak to a safeguarding officer, the help and support that is needed doesn’t happen. Care agencies are not changes, staff delivering care remain the same and issues are shunted between professionals and agencies with no one taking responsibility for resolving the issue of unsafe care.
Quote from by-and-for organisation supporting women living with disability
76. Most stakeholders reported that wider pressures on health and social care services are impacting a system, which was also perceived by stakeholders as fragile, under strain and facing difficulties in upholding safeguarding provisions for people with care and support needs. Such pressures include workforce issues and turnover, the impacts of COVID-19, concerns over the quality of staff training and cost of living pressures.
77. In the Skills for Care Workforce Intelligence Summary of domiciliary care services in the adult social care sector 2021/22, it was reported that there were an estimated 76,000 vacancies for care workers providing care in people’s homes, with 570,000 filled posts. This is the highest vacancy rate since records began in 2012/13. Just under half of staff in home (domiciliary) care services were employed on a full-time basis (46%) and 54% were employed part-time. The turnover rate for domiciliary care services was 31%, which equates to an estimated 159,000 workers leaving their role in the previous 12 months. Pay for doing this vital work remains an issue.[footnote 42]
78. The Association of Directors of Adult Social Services (ADASS) Autumn Survey Report 2022 stated that 491,663 people were waiting for an assessment, review or the start of a service or direct payment on 31 August 2022. Over the three-month period from 1 April to 30 June 2022, 1.1 million hours of homecare could not be delivered because of insufficient workforce capacity, leading to unmet and under met needs.[footnote 43]
79. Most stakeholders highlighted funding pressures within local authorities as a risk factor. The review team were provided with examples of where this has resulted in local authorities having less headroom to find savings, which echoes findings from a National Audit Office report on the state of the adult social care market in England.[footnote 44] Stakeholders including SAB Chairs, charitable organisations and frontline staff working with local authorities highlighted that as a result of such funding pressures, some local authorities have adjusted their threshold for support, meaning that where an at-risk individual who might have once qualified for care and support, may now be less likely to be offered it (see Chapter 4 for more detail on thresholds). Some stakeholders’ view was that this may in turn place vulnerable people at higher risk of being ‘missed’ by safeguarding professionals.
80. Government is already taking action to address some of these concerns by making up to £7.5 billion of new funding available for adult social care and discharge in England over two years. This includes up to £2.8 billion in 2023/24 and up to £4.7 billion in 2024/25. In addition, government has set out its plans for reforming adult social care in ‘Next steps to put People at the Heart of Care’, which sets out how government will be spending £700 million on reform over the next two years – building on the £100 million invested in the past year.
81. Stakeholders identified a need for increased funding and resources across all areas of safeguarding. Attention was drawn to low wages for care staff; the lack of resources among local authorities; the impact of care on individuals’ personal finances; and to the lack of available funding for nationwide support services.
82. The review also examined the links between funding and the provision and accessibility of support services for individuals who have been victims of this type of abuse.[footnote 45] Stakeholders were particularly concerned about the ‘patchy’ provision of specialist ‘by and for’ support services due to a lack of sustainable long-term funding. It is important to note that funding for such specialist and ‘by and for’ services is available primarily for victims of domestic abuse, where the perpetrator is “personally connected” to them. Victims of abuse where the perpetrator is not “personally connected” to them (i.e. friend, neighbour, or paid carer), and who therefore do not fall under the definition of domestic abuse, usually rely on local authority support or on the support of organisations that do not specialise in domestic abuse.
83. This finding, about access to support services, is echoed by the Domestic Abuse Commissioner’s recent research analysing over 4,000 survey responses.[footnote 46] The research refers to a ‘postcode lottery’, which highlights significant regional variation in the provision of services. The research also found that the combination of piecemeal funding, variation in service provision and increased demand on services make it all the more difficult for victims of abuse to access the support they need when they need it. The Domestic Abuse Commissioner’s research found that only 33% of organisations provide specialist community-based support for older victims of domestic abuse, while 14% provide specialist support for deaf victims and 26% for disabled victims. This research only considered individuals in “personally connected” relationships, so there is a gap in the review’s understanding of the specialist support available to people experiencing abuse from people who do not fall within the parameters of the Domestic Abuse Act 2021 definition. The report also reiterated the importance of allocating sufficient funding to ‘by and for’ and specialist services, to improve the availability of community-based service provision, noting that to date, funding for these services has been concentrated in London and the South East of England.
84. Government currently supports access to domestic abuse services, including specialist and ‘by and for’ services which deliver tailored support to disabled and older victims. The Home Office has already committed to multi-year funding for specialist and ‘by and for’ organisations as part of the Tackling violence against women and girls (VAWG) strategy[footnote 47] and the Tackling Domestic Abuse Plan.[footnote 48] In light of this commitment, last year the Home Office launched a consolidated VAWG Support and Specialist Services Fund with the Ministry of Justice, which will see up to £6 million ring-fenced funding for ‘by and for’ services over two years, from 2023/24 to 2024/25. This is the first national ‘by and for’ ring-fenced fund of its kind.
85. For all victims of crime, the Ministry of Justice has committed £154 million per year on a multi-year basis, for the next three years (2022/23 to 2024/25 inclusive). Most of this funding will be allocated via Police and Crime Commissioners who are responsible for funding victim services based on local commissioning needs and strategies. The Ministry of Justice published the Victims Funding Strategy in May 2022, which introduced national commissioning standards which encourage an expected level of service for victims.[footnote 49]
86. In addition, to drive improvement in the sector, DHSC has worked closely with the Local Government Association and ADASS to deliver the improvement programme through Partners in Care and Health (PCH) – formerly the care and health improvement programme. PCH conducts sector-led initiatives aimed at improving ‘care and health’ practices across adult social care, including adult safeguarding. To date, PCH has been funded by DHSC to facilitate projects such as:
- improving legal literacy among the social care safeguarding sector
- hosting webinars on transitional safeguarding, Making Safeguarding Personal, and discriminatory abuse
- developing the Safeguarding Adult Review (SAR) library and championing the Social Care Institute of Excellence’s (SCIE) SARs in rapid time model[footnote 50]
87. DHSC has funded SCIE to produce and maintain training and awareness resources on safeguarding adults and to deliver safeguarding improvement projects, including the development and dissemination of SAR quality markers to support people involved in commissioning, conducting and quality-assuring SARs.[footnote 51]
88. Stakeholders called for an increase in sustainable, multi-year investment to improve adult safeguarding responses and victim support, with a focus on specialist services tailored to people with care and support needs.
89. DHSC is increasing funding to local authorities to ensure that they have the resources needed for adult social care. At the Autumn Statement in November 2022, DHSC made the difficult decision to delay reforms to the charging system. But none of the £3.6 billion announced for charging reform in 2021 has been diverted away. The savings from this decision are being retained in local authority budgets to help them meet the current pressures in social care. In addition, DHSC are providing more funding for adult social care on top of the £3.6 billion, with an additional £2.7 billion in new grant funding. This will help to enable people to access the right care and support at the right time.
What will government do?
- a) DHSC will explore how findings from the CQC local authority assessment framework could better support safeguarding outcomes. One of the four themes that CQC will assess local authorities on is ‘how local authorities ensure safety within the system’. This will include assessing local authorities on the following safeguarding quality statement:
We work with people to understand what being safe means to them and work with our partners to develop the best way to achieve this. We concentrate on improving people’s lives while protecting their right to live in safety, free from bullying, harassment, abuse, discrimination, avoidable harm and neglect. We make sure we share concerns quickly and appropriately.[footnote 52]
The duty on CQC to assess local authorities’ delivery of their Care Act 2014 duties was commenced on 1 April 2023. Local authority assessments could inform whether targeted support is needed in specific local authorities to help improve safeguarding responses.
- b) The Home Office will invest £3 million specifically for ‘by and for’ organisations over 2023/24 and 2024/25, including organisations who support victims of abuse with different protected characteristics, for example, older victims or victims living with disability.
There is limited sharing of information and learning from best practice and failures where exists there is limited accountability for monitor progress to address failures.
90. Stakeholders, particularly SAB Chairs, reflected that they rely on a ‘jigsaw of co-operation’ driven by their network and others, rather than being supported by a single department or body responsible for driving improvements.
91. Safeguarding Adults Reviews (SARs) commissioned by SABs are a key source of information on lessons learned and failures in safeguarding practices (for more information, see Chapter 2 on the Care Act 2014).
92. The majority of SARs published from 1 April 2019 are stored and can be accessed via the SAR library on the National Network for Chairs of Adult Safeguarding Board website.[footnote 53] There is no duty on SABs to publish SARs. However, there is a requirement that SABs report on the SARs commissioned and completed in their annual reports. The purpose of this requirement is to provide transparency about how findings from each SAB’s annual report are being implemented, or specifically if any actions are not being implemented, why, and what is being done instead to implement findings. As outlined, having a SAR library is positive, however, the library does not allow users to easily identify patterns, or draw lessons learned between different SARs and does not facilitate easy data analysis across SARs. The SAB Chairs Network itself has regular meetings to share best practice and to identify issues of national importance between SABs. The review heard other ways to share best practice, including through the Business Managers Network, Reviewers Network, Regional Networks and webinars hosted by SCIE and PCH.
93. A new National Escalation Protocol was established in 2021 to begin to bridge the gap between local safeguarding issues that require a national response, and to address the issue of fragmentation of accountability and oversight of safeguarding for people with care and support needs.[footnote 54] The protocol will address issues from SARs that require a response that is beyond the scope of local SABs. The protocol allows issues to be flagged to central government for review and action, as outlined in Figure 5.
Figure 5: The National Escalation Protocol
Stage 1: Regional discussion
- local SAB chair raises issue/learning region
Stage 2: National Discussion
- regional group escalates to National Network
Stage 3: Discussion with DHSC
- National Network Chair(s) escalate to DHSC
- DHSC officials ensure the Minister is sighted on the issue raised in the national escalated SAR
Stage 4: Feedback
- National Network Chairs report back
94. SCIE, funded by DHSC, also provides training sessions to support the use of SAR Quality Markers.[footnote 55] This is a tool which supports people involved in commissioning, conducting and quality-assuring SARs, as well as responding to the learning generated from SARs. Attendance at this training is not mandatory, which was highlighted as an issue by some stakeholders including SAB Chairs and social work practitioners.
95. An analysis commissioned by the Care and Health Improvement Programme (CHIP, now known as PCH) of SARs in 2020 highlighted that 22% of responding local authorities had not carried out any SARs between 2017 and 2019.[footnote 56] The Care Act 2014 allows SABs to interpret when they need to commission a SAR. However, section 44 of the Care Act 2014 outlines the criteria that SABs must follow when commissioning a SAR.
96. In their review of SARs, PCH noted that the lack of clarity on the timings of SARs could have a detrimental effect on the ability to gather evidence if the SAR is not commissioned in a timely manner. The review noted that there is not a rigorous enough focus on protected characteristics of individuals, leading to possible unconscious bias, potentially preventing learning from being embedded across teams.
97. The SAB Chair Network reflected on how partners disseminate and use learning when a SAR does take place. The SAB is responsible for ensuring that the learning and recommendations for change are embedded in practice and service improvement. However, a SAB alone cannot command change, and the SAB Chair Network noted that change happens because individual agencies and partnerships make it happen. At present, there is no strategic oversight of sharing best practice, or follow-up mechanisms to hold local areas to account for implementing recommendations and taking on board learning set out in SARs.
98. Stakeholders also identified inconsistencies in the application of the Care Act 2014 safeguarding duties. For example, whether a SAR is published and how its learning is disseminated can vary depending on the individual commitment of SAB members. Stakeholders were concerned that the lack of strategic oversight of SAR learning had contributed to a lack of accountability around successful implementation of SARs at a local, regional and national level.
99. Where SAR findings require a response or dissemination of learning at a national level (central government departments and national regulatory bodies), government has already taken steps to try and improve engagement with SABs. This includes working with SABs to co-ordinate and learn from SAR findings by introducing the SAR Escalation Protocol. Stakeholders called on government to further improve the ways in which different agencies and organisations share information and learn from best practice and failures at local and national levels.
What will government do?
- a) DHSC will consider opportunities to strengthen the oversight of SARs, to monitor the effective implementation of SAR recommendations by reviewing the SAR national Escalation Protocol via engagement with SAB Chairs. Any updates to the protocol could learn from emerging best practice in the development of other oversight initiatives, such as the Domestic Homicide Review oversight mechanism and the Wales ‘Single Unified Safeguarding Response’.
- b) DHSC will continue to engage regularly with the SAB Chairs network via their network meetings, to proactively discuss this review’s key findings on what SARs should consider (including links to other reviews and perpetrator behaviour), with a view to encouraging best practice and reflecting any relevant changes in the SAR quality markers.
- c) DHSC will review the Care Act 2014 guidance sections covering safeguarding roles and responsibilities, including current guidance on SARs as part of action (b) under key finding 1 to tackle the fragmented oversight of safeguarding of people with care and support needs in England (review of Care Act guidance sections covering safeguarding roles and responsibilities).
- d) DHSC will explore commissioning another analysis of SARs, building on the SAB Chair analysis completed between 2017-19; where the SARs relate to abuse at home, identify key areas for improvement and share with relevant stakeholders, including through the new cross-government meetings referenced in action (c) under key finding 1 to tackle the fragmented oversight of people with care and support needs in England. This could include looking specifically at findings from SARs that mention power of entry, and consideration should be given to reviewing power of entry related findings from SARs on a regular basis.
- e) DHSC and the Home Office, working with other government departments, will consider ways in which to incorporate the voices of victims and survivors in policy-making and support operational safeguarding improvements, including where relevant the Domestic Abuse Commissioners’ lead on victim engagement.
- f) DHSC will ensure actions from the review, delivered by funded partners via the sector-led improvement offer, are informed by the voices of victims and survivors with personal experience.
- g) The Home Office is funding the Domestic Abuse Commissioner to develop a National Domestic Homicide and Suicide Oversight Mechanism. The mechanism will be used to strengthen the evidence base in this area and to hold national and local agencies to account in implementing learning to prevent future deaths and will draw on data from other post-death and serious incident reviews, including coroner’s reports and SARs. Home Office will consider insights and evidence from this mechanism.
Chapter 4: effectiveness of the local response to abuse and neglect in the home
The second main theme explored by the review focuses on the effectiveness of local and multi-agency responses to abuse in the home. The three key findings set out in this chapter are:
- i. There is varying implementation of the Care Act 2014 safeguarding provisions between different local areas.
- ii. This type of harm and relevant legislation is often poorly understood by frontline professionals.
- iii. Frontline professionals often lack the necessary tools and resources to allow them to best protect and support people with care and support needs who are, or are at risk of being, abused in their own home by the person providing their care.
There is varying implementation of the Care Act 2014 provisions between different local areas.
100. The review team engaged with stakeholders on the effectiveness of the Care Act 2014 and the supporting statutory guidance which embeds the Making Safeguarding Personal approach to decision making. This is a framework for protecting and supporting people with care and support needs from abuse and neglect. Stakeholders in general reflected that the experience of victims and the availability of support for individuals with care and support needs who are, or are at risk of being, abused in their home by people providing their care, can vary significantly between different areas. Although specific to “personally connected” relationships, this finding is also mirrored in the Domestic Abuse Commissioner’s ‘A Patchwork of Provision’ report.[footnote 57]
101. Some stakeholders highlighted that pressures on funding and resources, as set out in Chapter 3, have meant that some local authorities have set a high threshold for section 42 enquiries. For example, when local authorities are notified about a safeguarding concern, before undertaking a section 42 enquiry, they will first check that the person has care and support needs under section 9 of the Care Act 2014, as local authorities are only responsible for enquiring into safeguarding concerns if the person has care and support needs (as set out in Chapter 2). Stakeholders, including those from ‘by and for’, and larger charities, reflected that victims in different localities experience different sorts of barriers which make it more difficult to report abuse or contact their local authority safeguarding team. Some stakeholders also noted that some victims find themselves not believed that they have care and support needs.
102. The implementation of section 10 of the Care Act 2014, the duty to undertake carer assessments, was reported by stakeholders to vary significantly across different regions. As set out in Chapter 2, local authorities are required to undertake a carer’s assessment of any carer who appears to have a need for support. In 2021/22, local authorities assessed and/or supported 381,000 unpaid carers.[footnote 58] One quarter of carers who responded to the Carers UK State of Caring report 2022 said that they had received an assessment, or a review of their assessment, in the previous 12 months.[footnote 59] Stakeholders cautioned that such assessments must remain focused on carers’ changing circumstances. Stakeholders also reflected that if safeguarding actions arise as a result of the carer assessment, then relevant information should be shared with appropriate agencies that may need to be aware, such as the police. They noted that relevant safeguarding information should then be used to inform risk assessments of other agencies to draw a holistic picture of what the level of risk is, and what the appropriate safeguarding actions should be.
103. Some studies report that providing unpaid care at low levels of intensity can have positive impacts on an individual’s health and wellbeing. Most research, however, suggests that providing care, particularly at higher intensities, is associated with poorer physical and mental health.[footnote 60] The NHS Digital Personal Social Services Survey of Adult Carers in England, 2021-22 found that 67% of responding carers had had disturbed sleep in the last 12 months as a result of their caring role. 64% reported that they had felt a general feeling of stress and 48% reported that they had felt depressed. The majority of carers (57%) said that their caring role had not caused any financial difficulties over the past 12 months. However, approximately 43% stated that it had caused financial difficulties ‘to some extent’ or ‘a lot’.[footnote 61]
104. While registered providers are required to ensure that their care staff have suitable support, supervision and appraisal to enable them to carry out their duties, people caring for a loved one or friend may have limited access to formal support or resources.[footnote 62] The review heard from carer organisations who are concerned that informal and unpaid carers might be stigmatised for not providing ‘good care’ when they are doing their best, overlooking the very real challenges faced by people performing these vital roles.[footnote 63]
105. The 2021 ‘Caring as a social determinant of health’ (published by Public Health England, now known as The National Institute for Health Protection) concluded that: “More robust evidence is needed to identify if there are unique consequences for those people caring for older adults and how best to support them”.[footnote 64] The importance of support for carers is acknowledged in the People at the Heart of Care white paper.
106. Stakeholders called for the government to strengthen the implementation of the different Care Act 2014 provisions, in order to promote and achieve consistency in the protection and support available for people with care and support needs. The government is committed to improving implementation of the Care Act 2014 and has provided the introduction of the Care Quality CQC Assessment Framework, as outlined in the Health and Care Act 2022. Through this framework, the CQC will assess the performance of local authorities’ delivery of their adult social care duties, as set out under the Care Act 2014, including those relating to safeguarding.
What will government do?
- a) The Chief Social Worker team will support updates to the ‘Research in Practice’ materials on training, increase support and engagement for social workers in relation to unpaid carers, including undertaking carers’ assessments and care needs assessments for the person being cared for.[footnote 65]
This type of harm and relevant legislation is highly complex, making it challenging for frontline professionals to address.
107. SAB Chairs, frontline practitioners and academics commented on the difficulties frontline professionals experience in understanding or applying the range of existing legislation. This gap in understanding means that relevant legislative powers are sometimes not being effectively utilised to protect people with care and support needs. SAB Chairs reflected that there is a need for more support for frontline professionals to navigate this complex legal framework and to understand how relevant pieces of legislative guidance and provision interact. It was reported that local authorities, in some instances, are struggling to recruit lawyers in adult social care, to guide practitioners through this complex legislative landscape. A lack of ‘legal literacy’ was also referred to as a challenge among frontline professionals, with complex legislation remaining inaccessible and access to legal advice to support comprehension being limited.
Case study 2: ‘Zara’s story’ [footnote 66], [footnote 67] – a SAR highlighting the challenges for frontline professionals of addressing mental capacity when someone refuses care
Zara lived alone; she had some medical conditions that meant she could not leave her home for many years. She had experienced loss in her life but maintained contact with her family. Zara’s nephew supported his aunt with shopping, visiting her three times a week. Despite these regular visits, Zara felt lonely and isolated.
In the last five years of her life Zara was receiving care and support with personal care, food preparation and household tasks three times a day. This was organised by the local authority and support was given to Zara through a care agency. Zara was not easy to care for, she often refused any help, she was private and didn’t want to bother anyone. During this time, she wasn’t eating enough and often remained on the sofa under a blanket for long periods of time. Over time, the care agency, the local authority and health partners tried to strike a balance between respecting Zara’s wishes and fulfilling their duties to provide her with the care and support she required.
Eventually Zara’s situation deteriorated significantly, and she died in hospital. The cause of death was multiple organ failure and septicaemia. Zara has multiple pressure ulcers and was emaciated. Hospital staff noted the smell of wounds on admission, although the care workers had not noticed how bad they were in the time preceding her death. Nor did they note how thin she had become. After her death, a SAR was carried out and among the findings were poor legal literacy of practitioners and a lack of understanding of the requirements of the Mental Capacity Act 2005. Risk assessments did not consider that Zara was unable to make safe decisions in her own best interests and the balance between choice and safety, when dealing with someone who self-neglects, was not fully understood. This filtered through to care workers who did not challenge her when she said she was okay and who would not undertake the personal care she needed, despite this being laid out in the care plan put in place by the local authority.
A SAR was carried out to investigate the circumstances surrounding Zara’s death. The SAR found that there were multiple factors that led to Zara’s death and the review into her death made a series of recommendations which the local authority and relevant partners accepted to improve future practices and to learn from failures in safeguarding, as highlighted in Zara’s story.
108. Understanding the implementation of the Mental Capacity Act 2005 and its interaction with the Care Act 2014, was especially highlighted by social work and policing practitioners as an area where significant improvements are needed. For example, stakeholders reflected that in some cases, section 42 enquiries under the Care Act 2014 may not be investigated fully if there is any question about the victim’s mental capacity. Existing guidance and resources available to support the police include ‘Achieving Best Evidence’ which is designed to ensure that victims are heard no matter their needs. Despite this, practitioners noted that the police would sometimes halt investigations when there was a question of someone lacking capacity. This was because police officers felt that they would not be able to gather enough evidence to pursue these sorts of cases in court.[footnote 68]
109. DHSC have supported SCIE, as a sector-led improvement partner, in the development of online training materials regarding the Mental Capacity Act 2005, to increase understanding of the application of the Act among social care professionals. However, some stakeholders emphasised that training on the Act alone will not address all issues with its implementation. Knowledge and understanding of executive functioning, referring to the ability of an individual to understand the relevant information and give effect to their decision, has developed since the inception of the Act. [footnote 69] The University of Bristol noted in their SAR analysis on self-neglect, that practitioners lack confidence in carrying out capacity assessments or determining when they would need to do them.[footnote 70] Someone may ‘seem’ able to make a decision on a specific issue at a given time and place, such as accepting they ‘agreed’ to gift someone providing care with their assets, but may not be able to understand the consequences of this decision in the longer term. Safeguarding leads reported that continual updating of training on mental capacity aimed at frontline professionals is required, but that it is challenging to get it right despite their best efforts.
110. Practitioners including police and social workers expressed concerns about abuse of people with care and support needs who ‘do have capacity’ to make all relevant decisions but are targeted by people ostensibly providing care. Stakeholders shared the example of individuals with disabilities being ‘groomed’ to provide sexual favours or financial payments. Policing and social work stakeholders highlighted that the combination of limited resources and the complexities of these cases make them difficult to respond to.
111. The review also heard from stakeholders that there are gaps in frontline professionals’ understanding of the Mental Health Act 1983 and how this interacts with the Care Act 2014. For example, in cases where individuals are discharged into the community without linking them to other local services. In some cases, families providing care post-discharge may not know what support or carer assessments they are eligible for.
112. There is a range of existing guidance available, including for example Domestic Abuse statutory guidance and Domestic Homicide Reviews statutory guidance. However, stakeholders were still generally concerned about the limited understanding of abuse in care relationships, including the extent to which it is detected and reported. These difficulties are exacerbated by the fact that abuse in a domestic context is likely to remain hidden from plain sight and the individuals experiencing it may be vulnerable, isolated or dependent on the person providing their care. It may also be challenging for frontline professionals to identify when a carer’s behaviour is abusive or neglectful, as this behaviour can sometimes be mistaken as an individual ‘caring’ or acting in the victim’s ‘best interests’. An example of this is highlighted in case study 3.
Case study 3: ‘Edward and Caroline’ [footnote 71],[footnote 72] – a SAB review of financial abuse and psychological abuse
Edward was 90-year-old man who lived on his own. He relied on a walking stick due to issues with his mobility, had partial hearing loss and there were some concerns about his memory. For many years, he was supported by Simon, a long-term family friend. Sadly, Simon passed away unexpectedly. Simon’s daughter, Caroline, then began visiting Edward saying that she would help him. He gave her £20-£60 every week, which she said she needed for food - and she sometimes brought him a pint of milk but never anything worth the amount of money given. He said that he sometimes found Caroline very nice and supportive but, that at other times, she could yell and become abusive. Edward was worried about the amount of money that he was giving her but didn’t want to report her to the police because he had been close to her father and thought she was vulnerable.
A safeguarding concern was raised by someone who knew Edward was experiencing difficulties. During this process it was found Edward required a full assessment of all his needs and care services were put in place. A mental capacity assessment around his ability to manage his finances was completed. The assessment found that, with the support of another friend, Georgina, to prompt him, he was able to do this. Edward’s desired outcome was that he continued to give Caroline money because he was worried about her but that this be restricted to only £20 a week. Professionals were concerned about this but as he had capacity to make this decision, this was the agreement they settled on.
When the Safeguarding Review was conducted, six months later, it was found that (although Edward was generally happier with his care), Caroline was still regularly taking his money and he was unhappy about this. A new mental capacity assessment was conducted that concluded that he did not have capacity to manage this own finances anymore even with support from his friend Georgina. Edwards had arranged for Georgina to have power of attorney to support Edward so, in line with his wishes, she could arrange for Caroline to receive £20 a week.
113. Stakeholders flagged that more awareness is needed to promote further understanding of abuse in care relationships. Additionally, stakeholders noted that the different types of support services that victims engage with may have different levels of understanding of guidance and legislation. For example, VAWG service providers may have a better understanding of the Domestic Abuse Act 2021, and health and social care workers may have a better understanding of the Care Act 2014.
114. Beyond the complex legislative framework, some stakeholders reflected that there are discrepancies in the response of frontline professionals when such instances of abuse are disclosed. Stakeholders referred to this as a ‘fork in the road’. When someone who does not have care and support needs is subject to abuse, this can be addressed directly by the police and a criminal justice response may follow. However, when someone with care and support needs makes a disclosure, professionals should make initial ‘safeguarding’ referrals to local authorities who are then responsible for referring to, and involving the police if necessary. Some stakeholders expressed concerns that as a result, referrals are not always made to both criminal justice and health and social care agencies and the response to criminal abuse in care contexts is sometimes missed. This makes any criminal justice outcome even more difficult to access for victims who suffer from abuse perpetrated by a family member or friend. This is because they may be unwilling to engage with the criminal justice system for fear of the consequences this may have on their loved ones, a sentiment which may be further compounded by their dependence on family members or friends providing them with care and support.
115. Stakeholders called for more action from government to promote further understanding of this type of harm. Suggestions included strengthening the understanding of relevant legislation and making legislation accessible to all relevant frontline practitioners; improving access to legal advice; and addressing staffing capacity issues.
What will government do?
- a) The Home Office and DHSC will consider how to support agencies with statutory responsibilities to improve training among relevant frontline professionals on existing guidance and legislation to protect adults at risk of or experiencing abuse by people providing their care in their own home. This will empower professionals to use the full range of legislative protective measures and powers available, including by working with the College of Policing on relevant training and guidance for police officers.
- b) The Home Office and DHSC will consider how to use government channels to increase awareness amongst frontline staff of the prevalence and signs of abuse of adults by people providing care in their own home.
- c) Government will build on existing communication activities to help to raise public awareness of this form of abuse, with a focus on economic abuse and abuse of older people.
- d) As part of reforming the Domestic Homicide Review process, Home Office will launch a public consultation on the Domestic Homicide Review statutory guidance. We will use this as an opportunity to improve and strengthen guidance on how Domestic Homicide Reviews are conducted and what they must consider. This may include: (1) where possible strengthening the voices of victims, (2) improving awareness of forms of domestic abuse such as economic abuse and CCB, (3) integrating cross-government reviews such as SARs as evidence and (4) strengthening understanding and consideration of protected characteristics and intersectionality, including for example, age and disability.
Frontline professionals often lack the necessary tools and resources to allow them to best protect and support people with care and support needs who are, or are at risk of being, abused in their own home by the person providing their care.
116. Beyond the protections available to people with care and support needs under the Care Act 2014 provisions, it is important to consider all the tools available to frontline professionals to prevent or stop abuse. The lack of power of entry rights for social workers was often referenced by social care professionals over the course of this review. Such powers are available to the police when there is risk to life or risk of high harm, under the Police and Criminal Evidence Act 1984, or under the Mental Health Act 1983. Such powers focus on risk of physical harm and may neglect to address other forms of high harm abuse, such as controlling or coercive behaviour that is a high- risk factor of future violence towards the victim, and a known risk factor in domestic homicides and domestic abuse related suicides.[footnote 73], [footnote 74]
117. During stakeholder engagement, academics, SAB Chairs and frontline professionals in social care expressed that providing such powers to social workers in England would enable them to better protect and support people with care and support needs who are, or are at risk of being, abused in their own home by the people providing their care. It is worth noting that social workers in Scotland (Adult Support and Protection Act (Scotland) 2007) and Wales (Social Services and Well-being (Wales) Act 2014) have these similar rights.
118. Frontline professionals told the review that access to people with care and support needs can be especially difficult when their families distrust the authorities. In cases where there is deliberate and ongoing obstruction which can prevent social workers from engaging with adults at risk, social workers have few routes until the situation escalates to a point where it might be too late. Stakeholders consistently expressed that more should be done to provide social workers with the power of entry rights in England.
119. The review also looked specifically at the response of frontline police officers, as the police hold statutory responsibility for safeguarding together with local authorities who deliver social care. Similar to social care, the review heard that the response to people with care and support needs can vary. Throughout the review’s stakeholder engagement, the review only identified one police force area with a team who are solely focused on people with care and support needs.
120. Safeguarding practitioners within police forces described that ‘boundary issues’ further complicate their responses to individual cases, as a single police force may cover several different local authority areas. Police officers spoke passionately to the review team about their commitment to their work but noted that they often struggle with the limited resources available. Other stakeholders noted that they have observed that police partners do not have clear guidance when it comes to safeguarding those with care and support needs.
121. In relation to protection orders and their use, there are a variety of protection orders and penalties available to frontline professionals and victims in England which serve to protect individuals from harm. The Domestic Abuse Act 2021 has introduced Domestic Abuse Protection Orders (DAPOs) [footnote 75], although these are only applicable in circumstances involving “personally connected” individuals, they are broader than other forms of orders such as Domestic Violence Protection Orders (DVPOs) and Non-Molestation Order (NMOs) and have no maximum or minimum duration. However, there is no data available on how protection orders are being used, and what impact they might be having in protecting adults with care and support needs. During stakeholder engagement with frontline social workers, police officers and SAB Chairs, it was reported that protection orders are not an avenue they pursue often.
122. Stakeholders called for government to improve the resources available to frontline staff. This would ensure that they have the right tools to effectively protect and support people with care and support needs who are, or are at risk of, being abused in their own home by the person providing their care. This includes how effectively risk is assessed and how relevant information is shared between safeguarding partners.
What will government do?
- a) DHSC will review any new and relevant evidence on powers of entry for social workers since this issue was last considered by government during the passage of the Domestic Abuse Act 2021. This should include Safeguarding Adult Reviews in England and the use of equivalent powers in Scotland and Wales.
- b) DHSC and the Home Office will work with local authorities, the NHS and the police to identify opportunities to improve the consistency in application of risk assessment processes to better protect adults with care and support needs receiving care in their own homes from abuse, including through the sector- led improvement offer.
- c) DHSC and the Home Office will work with local authorities, the NHS and the police to identify opportunities to improve reporting and recording practices to take into account economic abuse and abuse in care contexts, for example recording the use and effectiveness of court orders.
- d) DHSC will explore commissioning a new, one-off qualitative survey for local authority partners to understand their views on improvements to the reporting and recording practices on this topic, via the sector-led improvement offer.
- e) Home Office and Ministry of Justice will pilot the new Domestic Abuse Protection Orders in three pilot sites and will consider how to review their effectiveness during the pilot, to determine whether the new notices and orders should be rolled out nationally. Third parties (with leave of the court) will be able to apply to the family court for a Domestic Abuse Protection Order on behalf of someone else, to protect victims from all forms of domestic abuse, including non-physical abuse and controlling or coercive behaviour. The police will also be able to apply for these orders directly in the magistrates’ courts, and criminal, family and civil courts. The court will also be able to make these orders on conviction of a criminal offence involving domestic abuse.
Chapter 5: research, evidence and learning
This final chapter of the review explores the limitations of existing research, evidence and learning. The key findings in this chapter are:
- i. There is a lack of available data on the prevalence of abuse in care relationships and the data that is available is poorly utilised.
- ii. There is a lack of understanding into the causes of abuse in care relationships, and the behaviours of perpetrators in this context.
There is a lack of available data on the prevalence of abuse in care relationships and the data that is available is poorly utilised.
123. We do not have robust data on the prevalence of abuse in care relationships. Our best estimates of prevalence relate to abuse that is reported or responded to by authorities. However, this data is poorly utilised and, as with reported domestic abuse more generally, is likely to be an underestimate of actual abuse experienced. Assessing the prevalence of abuse in care relationships is therefore challenging, considering the different types and ways in which care is provided. Additionally, where there has been research on this topic, it is often outdated and focuses on specific subsets of groups such as those with disabilities or older people, which cannot be generalised to the adult population receiving care.
124. An example of research specifically focusing on abuse of older people is the ‘UK Study of Abuse and Neglect of Older People Prevalence Survey Report’, a nationally representative survey based on older people living in private households in the UK. The survey estimated that 4% of adults aged 66 and over reported experiencing mistreatment involving a family member, friend, care worker, neighbour or acquaintance during the previous year.[footnote 76] In a similar study, Cooper and others conducted a systematic review of studies of elder abuse and neglect in domiciliary settings, care, and nursing homes both in the UK and abroad. One study focusing on intermediate care and nursing homes found that almost 36% staff reported observing and 10% reported committing physical abuse in the previous year. Most staff (81%) had observed and 40% had committed psychologically abusive acts.[footnote 77]
125. The Crime Survey for England and Wales (CSEW) provides the most reliable data on the prevalence of different crimes, including domestic abuse. The CSEW, however, does not collect data on abuse happening within care relationships, which limits our understanding on the scale of the issue. The Office for National Statistics, in line with commitments set out in the Inclusive Data Taskforce and as set out in the Tackling Domestic Abuse Plan, aim to be as inclusive as possible with their sample, and are exploring the feasibility of expanding the CSEW to include those in residential care settings.
126. The CSEW does collect data on the experiences of domestic abuse among older adults and people who report having a disability. This may include individuals with care and support needs but should not be used as a proxy for the levels of abuse within care relationships. The year ending March 2022 survey found that those aged 75 and over were the least likely age group to experience domestic abuse in the last year (2%) and disabled people were more than twice as likely to experience abuse than non-disabled people (10% and 4% of adults aged 16 and over respectfully).[footnote 78]
127. Barriers to identification, reporting, and recording these abuses may translate into limited and incomplete information about cases brought to the attention of safeguarding authorities. The NHS Digital Safeguarding Adults Collection (SAC) brings together data collected by local authorities demonstrating the scale of safeguarding activities taking place at both regional and national levels.[footnote 79] The SAC publication notes that there are limitations around the interpretation and usage of the data, due to local variation in how the safeguarding activity is defined and reported.[footnote 80] Stakeholders reflected that the SAC does not provide a true national picture, as local authorities use different IT systems, which makes it very difficult to combine local level data to aggregate regional trends, and can lead to inefficiencies in data collection and analysis. Other data sets that monitor abuse of people with care and support needs in their own homes are the CQC regulatory data (which covers regulated providers providing personal care in someone’s home). Additionally, SAB annual reports and SAB strategic plans both highlight learning points and actions to take forward if a SAR relating to abuse or neglect in someone’s own home was commissioned by the SAB. The SAR library has the potential to be a useful source of data but requires significant improvements to the way information is recorded and organised, akin to the Domestic Homicide Reviews repository.
128. Data collected by the police on abuse perpetrated in care relationships reportedly varies by force and is dependent on individual force systems. The Crown Prosecution Service also reported difficulties in isolating data on abuse and neglect within care relationships on their IT systems.
129. In some cases, the review heard that relevant data is not collected at all. For example, coroners do not collate information on cases where there might have been a concern about care leading to death in a domestic setting. Individual coroners may raise a ‘Prevention of Future Death’ report, which sets out recommendations for government action. However, there has been no analysis to date of all Prevention of Future Death reports to synthesise common themes across findings and promote national learning. There is also no systematic follow up or accountability mechanism to determine to what extent or how effectively recommendations have been implemented across government departments.
130. When relevant data is collected, the review heard that a lot of cases are not escalated appropriately to manage risk and protect victims. As discussed earlier in the report, a Multi-Agency Risk Assessment Conference (MARAC) is a regular local meeting to discuss how to help victim/survivors of domestic abuse who have been assessed as being in the top 10% at risk of homicide or serious harm.[footnote 81] In the year ending March 2022, less than 1% of MARAC referrals in England were from adult social care services.[footnote 82]
131. Criminal justice data provides insight on crimes related to ill-treatment or neglect of cared-for people. These are recorded under section 20 (‘Care worker ill-treatment or wilful neglect of an individual’) and section 21 (‘Care provider breach duty of care resulting in ill-treatment/neglect of individual’) of the Criminal Justice and Courts Act 2015. Data on the total number of offences and crime outcomes are not currently published at this level of detail. However, Home Office unpublished data for 38 forces that provided data across England and Wales, show for financial year 2020/21, there were 613 section 20 and 21 offences recorded.[footnote 83] Over a third (35%) of these offences had the outcome of evidential difficulties (suspect identified; victim supports action). Further action was undertaken by another body/agency in one in five offences (20%), while only 4% resulted in a charge. The Ministry of Justice publish data on prosecutions and convictions of section 20 and section 21. In 2021, on an all-offence basis, there were 139 prosecutions and 31 convictions for the offences.[footnote 84] These both reflect increases from the previous year (68 prosecutions and 24 convictions).[footnote 85]
132. Available data shows that abuse in care relationships can result in court enforced protection orders or CQC-led action, such as fines or more serious charges where there is evidence of harm caused. Social workers tend to be on the frontline of identifying abuse in care contexts, but whether such concerns subsequently involve a criminal justice response is not clear. This makes it difficult to efficiently monitor the effectiveness of safeguarding and criminal justice responses, and to identify lessons learned.
133. Stakeholders called on government to improve the quality and frequency of data gathering and analysis to better understand this type of harm, including by conducting further research into the scale of harm in care relationships and into opportunities for prevention.
What will government do?
- a) The DHSC and the Home Office will work with other government departments to better understand where links have been made, and where further links could be explored between the information captured by relevant existing data sources on the prevalence and forms of abuse experienced at home by people with care and support needs by carers. Data sources could include NHS Digital SAC data, the Domestic Homicide Reviews repository, SAR library, cold case reviews, prevention of death reports, coroners’ reports, mental health risk assessments, CSEW and CQC safeguarding data.
- b) The Health and Care Act 2022 includes provisions for the CQC to assess the performance of local authorities’ delivery of their adult social care duties, as set out under the Care Act 2014, including those relating to safeguarding. DHSC will work with the CQC to consider how the recommendations and outcomes of this review could inform CQC’s new assessment of local authorities.
- c) To support strengthening evidence and data, the Home Office will build an online repository to hold all Domestic Homicide Reviews which will go live later this year. The repository will allow stakeholders and academics to analyse patterns in domestic homicides, coming to a fuller understanding of potential triggers and causes. Within the repository we will be collecting data on victims and perpetrators of domestic homicide who were carers, either for each other or for someone else in their lives, and other demographic data such as age. The site will be publicly accessible and safeguarding professionals will be able to search for Domestic Homicide Reviews where either the victim or perpetrator was a carer and identify themes, learning and actions that they can take away to improve their own agencies’ responses to victims of domestic abuse in the future.
There is a lack of understanding of the nature and causes of abuse in care relationships, and the behaviours of perpetrators in this context.
134. As mentioned in earlier sections of this review, there is limited understanding about the causes and nature of abuse within caring relationships. Research on care-related abuse within the home is even more sparse. Studies are often small-scale or international which makes it difficult to generalise findings to those at risk across England.
135. A systematic review identified risk factors on abuse or neglect in adult residential care services using the following categories: cultural or organisational characteristics, staff characteristics and characteristics of cared for people.[footnote 86] Cultural or organisational factors included staff shortages, inexperience and lack of training.[footnote 87] For staff characteristics, factors included being younger, a tendency towards abusive behaviour/pre-existing problems and staff ‘burnout’.[footnote 88] Risk factors for cared for people included older age and physical and/or mental impairments that would mean that the cared for person was highly dependent on others for help and care.[footnote 89]
136. To improve understanding in this area, the government has funded and supported relevant research projects. This includes DHSC who currently fund and support research through the National Institute for Health and Care Research (NIHR). The NIHR Adult Social Care Research Unit provides policymakers with the evidence they need to make decisions about adult social care. They are currently undertaking research that could help improve our understanding of the care at home landscape and unpaid care relationships, including ‘Quality, workforce and homecare’, ‘Assessing attitudes to providing unpaid care’ and ‘Understanding adult hidden carers’ (unpaid carers that do not identify as carers in England). NIHR-funded projects have explored abuse in a care context, including Stevens and others 2014 which reviewed local authority approaches to safeguarding and found that responses to elder abuse have created different kinds of ambiguity and conflict, requiring both top-down and bottom-up policy interventions. [footnote 90] Another study identified factors underlying cases of mistreatment in the care of older people, including: infrastructure, management and procedures, training and skills of staff, resident population characteristics, organisational culture, isolation and changes from outside the organisation.[footnote 91] However, these research examples do not have a specific focus on understanding nature and causes of abuse in care at home relationships.
137. Home Office funded relevant research; the Vulnerability Knowledge and Practice Programme (VKPP) Domestic Homicide Project is the first police-led work of its kind to collect and analyse data on domestic homicides and suspected domestic abuse related victim suicides across England and Wales (see Figure 6 for more information on the key findings).[footnote 92] The VKPP Carer’s Spotlight Briefing found that one in six domestic abuse related deaths involved a care relationship.[footnote 93] Adult family homicides made up the largest proportion of these deaths, which is the converse of overall domestic homicides where intimate partner homicides are most common. Analysis of the 79 victims revealed that in just over one-fifth of the intimate partner homicides the suspect either died or attempted to die by suicide following the murder. The issue of neglect was present in a number of intimate partner and adult family homicides where the suspect cared for the victim.
138. In 2022, the Home Office published findings from an analysis of 108 Domestic Homicide Reviews regarding 113 victims.[footnote 94] Sixty-nine percent of those deaths occurred in 2018 or 2019. The analysis found that 11% of all victims were carers. Only one of the victims with a caring role had received a carer’s assessment of their support needs. 11% of the 94 perpetrators were carers, and none had received a carers assessment under the Care Act 2014. Given this is a one-off analysis, continued work on the development of a Domestic Homicide Reviews repository will facilitate greater knowledge in this area, particularly where SARs and Domestic Homicide Reviews may have been conducted jointly or where abuse is identified to have occurred in care contexts.
Figure 6: VKPP Carers Spotlight Briefing summary of key findings
The VKPP Carers Spotlight Briefing found that:
-
Cases involving a caring relationship increased overall from Year 1 (2020- 21) to Year 2 (2021-22) by 39% (n=13). This was driven by adult family homicide deaths as intimate partner homicide cases decreased – COVID- 19 restrictions may have put intimate partner cared-for victims at more risk, whereas emergence from the pandemic exposed victims of familial domestic abuse to more risk – especially where the suspect was cared-for by the victim.
-
Nearly three quarters of the 79 victims were female (n=58) and one quarter were male (n=21).
-
The direction of caring relationship varied by case type. Intimate partner homicide (IPH) cases were more likely to involve a cared-for victim (86%, n=25), whereas adult family homicides (AFH) and suspected victim suicides had a more even split of cared-for victim and cared-for suspect.
-
AFH victims tended to be older than IPV victims. The opposite was true for suspects, where AFH suspects tended to be younger. This is in keeping with the profile of AFH which often involved adult children or grandchildren killing older relatives.
-
Care needs profiles between cared-for victims and cared-for suspects differed. Cared-for victims were most likely to have physical health needs and cared for suspects mental health needs or illnesses.
-
71% (n=51) of victims and/or suspects were known to non-police agencies – most commonly social care, health, or mental health services. Multi- agency groups were noted as being involved in 13 cases.
-
The briefing makes four recommendations for improving practice which highlight the need for greater awareness of domestic abuse in caring relationships, in particular in completing DASH, DARA or Care Act 2014 risk assessments and making multi-agency or adult safeguarding referrals, noting where relevant – incidents of mental ill health and caring dynamics.
139. Proposed actions for government in Chapter 4 of this review reflects the suggestions for practice improvements made in the VKPP Carers Spotlight Briefing. There remain significant gaps in research and data on abuse and neglect in care relationships. Stakeholders called for further research to improve our understanding of the nature and causes of abuse in care relationships.
What will government do?
- a) DHSC and the Home Office will work with other government departments and relevant independent partners to scope further research to better understand this form of abuse in line with the review’s findings.
Chapter 6: conclusion
This chapter summarises the key findings of the review and what government will do in response.
140. As set out in the Terms of Reference, the aims of this review were to review the scope and accessibility of the: existing protections for adults at risk of or experiencing abuse in their own home by people providing their care support for adults abused in their own home by people providing their care.
141. To achieve this, the review team engaged with, and collected evidence from, a broad range of stakeholders as set out in detail in Annex A, worked across government, and sought views of people with personal experience.
142. Based on the evidence collected, this review has identified three key themes as areas where improvements should be made, underpinned by eight key findings. The review proposes a set of actions for government to take forward in response to these findings. These are summarised in Figure 7 below.
143. The Home Office and DHSC will provide an update on this programme of work in due course. The review reflects policy and legislative developments at the time of writing, and any implementation plan should continue to consider changes and developments to the social and political landscape and context.
Figure 7: Summary of key themes, issues and what government will do in response
Leadership and accountability
There is fragmented oversight and accountability of safeguarding in England resulting in an over-reliance on sector led improvement and insufficient learning from missed opportunities.
Key finding 1: Oversight of safeguarding in England is fragmented and there is limited accountability.
Stakeholders called for strengthened oversight and accountability mechanisms of safeguarding people with care and support needs who receive care at home in England to improve the coherence of the response to this type of harm and better protect and support victims of abuse and neglect with care and support needs.
What will government do?
-
a) DHSC and the Home Office will encourage the Domestic Abuse Commissioner, the Victims’ Commissioner and the Chief Social Worker, to review, promote and disseminate best practices concerning the protection of people with care and support needs – specifically those who are at risk of being abused in their own home by the people providing their care.
-
b) DHSC will review sections of the Care Act 2014 guidance covering safeguarding roles and responsibilities, identifying opportunities to clarify the roles and responsibilities of government departments and statutory agencies, and rights and redress for victims and survivors. If changes to statutory guidance cannot be prioritised, DHSC will explore opportunities to develop or amend non-statutory guidance.
-
c) DHSC and the Home Office, working with the Chief Social Worker, will regularly bring together representatives from across government to promote better join up between departments with oversight responsibilities and monitor the progress of actions from this review, leveraging existing governance where appropriate. Attendees of this new cross-government meeting may include members of the DHSC Adult Safeguarding Forum, chaired by the Chief Social Worker and Chief Nurse convening key representatives of organisations with safeguarding duties (local authorities) and responsibilities (including the CQC, police and the NHS).
Key finding 2: Competing pressures and insufficient resources available have a negative impact on the safety of the people with care and support needs.
Stakeholders called for an increase in sustainable, multi-year investment to improve the adult safeguarding responses and available victim support, with a focus on specialist services tailored to the needs of people with care and support needs.
What will government do?
- a) DHSC will explore how findings from the CQC local authority assessment framework could better support safeguarding outcomes. One of the four themes that CQC will assess local authorities on is ‘how local authorities ensure safety within the system’. This will include assessing local authorities on the following safeguarding quality statement:
We work with people to understand what being safe means to them and work with our partners to develop the best way to achieve this.
We concentrate on improving people’s lives while protecting their right to live in safety, free from bullying, harassment, abuse, discrimination, avoidable harm and neglect. We make sure we share concerns quickly and appropriately.[footnote 95]
The duty on CQC to assess local authorities’ delivery of their Care Act 2014 duties was commenced on 1 April 2023. Local authority assessments could inform whether targeted support is needed in specific local authorities to help improve safeguarding responses.
- b) The Home Office will invest £3 million specifically for ‘by and for’ organisations over 2023/24 and 2024/25, including organisations who support victims of abuse with different protected characteristics, for example, older victims or victims living with disability.
Key finding 3: There is limited sharing of information and learning from best practice and failures.
Stakeholders called on government to improve the ways in which different agencies and organisations share information and learning from best practice and failures.
What will government do?
-
a) DHSC will consider opportunities to strengthen the oversight of SARs, to monitor the effective implementation of SAR recommendations by reviewing the SAR national Escalation Protocol via engagement with SAB Chairs. Any updates to the protocol could learn from emerging best practice in the development of other oversight initiatives, such as the Domestic Homicide Review oversight mechanism and the Wales ‘Single Unified Safeguarding Response’.
-
b) DHSC will continue to engage regularly with the SAB Chairs network via their network meetings, to proactively discuss this review’s key findings on what SARs should consider (including links to other reviews and perpetrator behaviour), with a view to encouraging best practice and reflecting any relevant changes in the SAR quality markers.
-
c) DHSC will review the Care Act 2014 guidance sections covering safeguarding roles and responsibilities, including current guidance on SARs as part of action (b) under key finding 1 to tackle the fragmented oversight of safeguarding of people with care and support needs in England (review of Care Act guidance sections covering safeguarding roles and responsibilities).
-
d) DHSC will explore commissioning another analysis of SARs, building on the SAB Chair analysis completed between 2017-19; where the SARs relate to abuse at home, identify key areas for improvement and share with relevant stakeholders, including through the new cross-government meetings referenced in action (c) under key finding 1 to tackle the fragmented oversight of people with care and support needs in England. This could include looking specifically at findings from SARs that mention power of entry, and consideration should be given to reviewing power of entry related findings from SARs on a regular basis.
-
e) DHSC and the Home Office, working with other government departments, will consider ways in which to incorporate the voices of victims and survivors in policy-making and support operational safeguarding improvements, including where relevant the Domestic Abuse Commissioners’ lead on victim engagement.
-
f) DHSC will ensure actions from the review, delivered by funded partners via the sector-led improvement offer, are informed by the voices of victims and survivors with personal experience.
-
g) The Home Office is funding the Domestic Abuse Commissioner to develop a National Domestic Homicide and Suicide Oversight Mechanism. The mechanism will be used to strengthen the evidence base in this area and to hold national and local agencies to account in implementing learning to prevent future deaths and will draw on data from other post-death and serious incident reviews, including coroner’s reports and SARs. Home Office will consider insights and evidence from this mechanism.
Effectiveness of the local response to abuse in the home
Local responses to this form of abuse are inconsistent and ineffective because frontline staff do not sufficiently understand this form of abuse and experience difficulties navigating the complex legislative framework.
Key finding 4: There is varying implementation of the Care Act 2014 safeguarding provisions between different local areas.
Stakeholders called for the government to strengthen the implementation of the different Care Act 2014 provisions in order to promote and achieve consistency in the protection and support available for people with care and support needs.
What will government do?
- a) The Chief Social Worker team will support updates to the ‘Research in Practice’ materials on training, increase support and engagement for social workers in relation to unpaid carers, including undertaking carers’ assessments and care needs assessments for the person being cared for.[footnote 96]
Key finding 5: This type of harm and relevant legislation is often poorly understood by frontline professionals.
Stakeholders called for more action from Government to promote further understanding of this type of harm, including strengthening the understanding of relevant legislation and making legislation accessible to all relevant frontline practitioners, improving access to legal advice, and addressing staffing capacity issues.
What will government do?
-
a) The Home Office and DHSC will consider how to support agencies with statutory responsibilities to improve training among relevant frontline professionals on existing guidance and legislation to protect adults at risk of or experiencing abuse by people providing their care in their own home. This will empower professionals to use the full range of legislative protective measures and powers available, including by working with the College of Policing on relevant training and guidance for police officers.
-
b) The Home Office and DHSC will consider how to use government channels to increase awareness amongst frontline staff of the prevalence and signs of abuse of adults by people providing care in their own home.
-
c) Government will build on existing communication activities to help to raise public awareness of this form of abuse, with a focus on economic abuse and abuse of older people.
-
d) As part of reforming the Domestic Homicide Review process, Home Office will launch a public consultation on the Domestic Homicide Review statutory guidance. We will use this as an opportunity to improve and strengthen guidance on how Domestic Homicide Reviews are conducted and what they must consider. This may include: (1) where possible strengthening the voices of victims, (2) improving awareness of forms of domestic abuse such as economic abuse and CCB, (3) integrating cross-government reviews such as SARs as evidence and (4) strengthening understanding and consideration of protected characteristics and intersectionality, including for example, age and disability.
Key finding 6: Frontline professionals often lack the necessary tools and resources to fully protect and support people with care and support needs who are, or are at risk of being, abused in their own home by the person providing their care.
Stakeholders called for Government to improve the resources available to frontline staff and ensure they have the right tools to be able to effectively protect and support people with care and support needs who are, or are at risk of, being abused in their own home by the person providing their care. This includes how effectively risk is assessed and how relevant information is shared between safeguarding partners.
What will government do?
-
a) DHSC will review any new and relevant evidence on powers of entry for social workers since this issue was last considered by government during the passage of the Domestic Abuse Act 2021. This should include Safeguarding Adult Reviews in England and the use of equivalent powers in Scotland and Wales.
-
b) DHSC and the Home Office will work with local authorities, the NHS and the police to identify opportunities to improve the consistency in application of risk assessment processes to better protect adults with care and support needs receiving care in their own homes from abuse, including through the sector-led improvement offer.
-
c) DHSC and the Home Office will work with local authorities, the NHS and the police to identify opportunities to improve reporting and recording practices to take into account economic abuse and abuse in care contexts, for example recording the use and effectiveness of court orders.
-
d) DHSC will explore commissioning a new, one-off qualitative survey for local authority partners to understand their views on improvements to the reporting and recording practices on this topic, via the sector-led improvement offer.
-
e) Home Office and Ministry of Justice will pilot the new Domestic Abuse Protection Orders in three pilot sites and will consider how to review their effectiveness during the pilot, to determine whether the new notices and orders should be rolled out nationally. Third parties (with leave of the court) will be able to apply to the family court for a Domestic Abuse Protection Order on behalf of someone else, to protect victims from all forms of domestic abuse, including non-physical abuse and controlling or coercive behaviour. The police will also be able to apply for these orders directly in the magistrates’ courts, and criminal, family and civil courts. The court will also be able to make these orders on conviction of a criminal offence involving domestic abuse.
Research, evidence and learning
Available data is collected, analysed and held disparately across government departments and agencies. There is limited research on this type of abuse.
Key finding 7: There is a lack of available data on the prevalence of abuse in care relationships and the data that is available is poorly utilised.
Stakeholders called on government to improve the quality and frequency of data gathering and analysis to better understand this type of harm, including further research on the scale of harm in care relationships and opportunities for prevention, drawing on available data sources resources available to frontline staff to protect and support people with care and support needs.
What will government do?
-
a) The DHSC and the Home Office will work with other government departments to better understand where links have been made, and where further links could be explored between the information captured by relevant existing data sources on the prevalence and forms of abuse experienced at home by people with care and support needs by carers. Data sources could include NHS Digital SAC data, the Domestic Homicide Reviews repository, SAR library, cold case reviews, prevention of death reports, coroners’ reports, mental health risk assessments, CSEW and CQC safeguarding data.
-
b) The Health and Care Act 2022 includes provisions for the CQC to assess the performance of local authorities’ delivery of their adult social care duties, as set out under the Care Act 2014, including those relating to safeguarding. DHSC will work with the CQC to consider how the recommendations and outcomes of this review could inform CQC’s new assessment of local authorities.
-
c) To support strengthening evidence and data, the Home Office will build an online repository to hold all Domestic Homicide Reviews which will go live later this year. The repository will allow stakeholders and academics to analyse patterns in domestic homicides, coming to a fuller understanding of potential triggers and causes. Within the repository we will be collecting data on victims and perpetrators of domestic homicide who were carers, either for each other or for someone else in their lives, and other demographic data such as age. The site will be publicly accessible and safeguarding professionals will be able to search for Domestic Homicide Reviews where either the victim or perpetrator was a carer and identify themes, learning and actions that they can take away to improve their own agencies’ responses to victims of domestic abuse in the future.
Key finding 8: There is a lack of understanding into the causes of abuse in care relationships.
Stakeholders called for further research to improve our understanding of the nature and causes of abuse in care relationships.
What will government do?
- a) DHSC and the Home Office will work with other government departments and relevant independent partners to scope further research to better understand this form of abuse in line with the review’s findings.
Annex A – Methodology
144. The evidence presented in the review includes a combination of findings from stakeholder engagement and a review of the existing literature and data (such as the Crime Survey for England and Wales and published social care statistics). This evidence sought to shed light on the prevalence, experiences of, and responses to abuse towards adults in their own homes by people providing their care.
Stakeholder engagement
145. The review team sought to generate evidence representing a broad group of stakeholders and the specific needs of different cohorts, such as older people, and deaf and disabled people. In total, the review team engaged with 127 individuals, representing over 40 organisations and stakeholder groups via roundtable discussions, workshops and one-to-one interviews.
146. The review team engaged cross-government policy teams within the Home Office, Department of Health and Social Care, Ministry of Justice, Department for Work and Pensions, Department for Levelling Up, Housing and Communities, and the Cabinet Office. Evidence was also collected from experts by experience, including: representatives from the violence against women and girls and domestic abuse sector, the deaf and disability sector, organisations representing and working with older people with care and support needs and, experts involved in delivery of the existing criminal and safeguarding system including local authorities and social work professionals, police, academics, and the Crown Prosecution Service.
147. A total of seven stakeholder workshops and roundtable discussions were held with thematic stakeholder groups, attended by seventy-seven stakeholder participants. Fifty one-to-one interviews with stakeholder representatives as summarised in the table below. Workshops and roundtables were held virtually and included frontline professionals including social workers, police officers, care workers and advocates and ‘by and for’ organisations. Separate sessions were held with police and criminal justice partners, and academics. The disability and older people organisations (specialist and ‘by and for’) were represented in roundtables to provide the voice of victims and survivors.
Table 1: Summary of one-to-one interviews with stakeholder representatives
| Academic experts | 9 |
|---|---|
| Disability sector | 8 |
| Health and social care | 10 |
| Housing sector | 7 |
| Other (such as other government departments and local government representatives) | 9 |
| Police and criminal justice | 7 |
| Total | 50 |
148. The review team aimed to hear the views of victims and survivors through expert sector organisations. Discussion guides were developed and agreed alongside these expert sector organisations, prioritising the wellbeing of the interviewees, and avoiding re-traumatisation.
149. In addition to targeted stakeholder engagement, the review team maintained an open mailbox, receiving correspondence from over 130 organisations.
Limitations
150. Throughout the report the review team discussed the particularly hidden nature of the abuse that people with care and support needs may be suffering at the hands of the people providing their care and the complex nature of this abuse type. This review does not aim to be an exhaustive analysis of this type of harm, but it rather aims to shed a light on the complexity and key issues present when dealing with this type of abuse. Therefore, the report may not cover all issues related to harm in the context of victims with care and support needs exhaustively. The review focuses on the key themes that arose from stakeholder engagement and existing literature. The review recognises that further research should be undertaken to better understand and tackle this type of harm as set out in Chapter 5.
151. While extensive stakeholder engagement was undertaken as outlined above, findings cannot be viewed as representative of all views and experiences across England.
Use of quotes and case studies
152. To illustrate evidence which came to light in the process of carrying out this review, the report contains case studies. The review summarises findings from stakeholder roundtables, workshops, and one-to-one interviews, and quotes have been used to reflect some of the common themes. All quotes and case studies have been anonymised so personally identifiable information has been removed. Permission has been obtained from all relevant stakeholders to include anonymised quotes within the review. Quotes reflect what the review team heard from stakeholder representatives, and therefore express personal and professional perspectives.
Annex B – Acronyms
| CQC | Care Quality Commission |
|---|---|
| AFH | Adult family homicides |
| ADASS | Association of Directors of Adult Social Services |
| APCC | Association of Police and Crime Commissioners |
| CSEW | Crime Survey for England and Wales |
| DfE | Department for Education |
| DHSC | Department for Health and Social Care |
| DLUHC | Department for Levelling Up, Housing and Communities |
| DWP | Department for Work and Pensions |
| DBS | Disclosure and Barring Service |
| DA Act | Domestic Abuse Act 2021 |
| DAPO | Domestic Abuse Protection Orders |
| DARA | Domestic Abuse Risk Assessment |
| DASH | Domestic Abuse, Stalking and Harassment |
| DHR | Domestic Homicide Reviews |
| DVPO | Domestic Violence Protection Orders |
| HSE | Health Survey for England |
| ICB | Integrated Care Board |
| IPH | Intimate partner homicides |
| MHA | Mental Health Act |
| MOJ | Ministry of Justice |
| MARAC | Multi-Agency Risk Assessment Conferences |
| MASH | Multi-Agency Safeguarding Hubs |
| NIHR | National Institute for Health and Care Research |
| NMO | Non-Molestation Order |
| OPG | Office of the Public Guardian |
| PCH | Partners in Care and Health |
| PSW | Principal Social Worker |
| SAR | Safeguarding Adult Review |
| SAC | Safeguarding Adults Collection |
| SAB | Safeguarding Adults Board |
| SANN | Safeguarding Adults National Network |
| SCIE | Social Care Institute for Excellence |
| CPS | The Crown Prosecution Service |
| ONS | The Office for National Statistics |
| VKPP | Vulnerability Knowledge and Practice Programme |
Annex C – Definitions contained within the review’s Terms of Reference
-
Own home: This is where the individual permanently resides, whether rented, owned or provided by the local authority. It is where the adult is fully supported to live independently with care arrangements and pays either full or part towards tenancy.
-
Personally connected: People providing care who are “personally connected” for example family members, intimate partners and people who were or are in a civil partner or married.
-
Unpaid carers: Unpaid carers, for example neighbours or friends who provide care for the person.
-
Paid carers: Paid carers – employed care workers, personal assistants and other paid individuals in a position of trust who provide care for the person.
-
Volunteers: Individuals providing care as part of a voluntary organisation to the person.
Annex D – Definition of domestic abuse under the Domestic Abuse Act 2021
Section 1: Definition of “domestic abuse”
(1) This section defines “domestic abuse” for the purposes of this Act.
(2) Behaviour of a person (“A”) towards another person (“B”) is “domestic abuse” if—
-
(a) A and B are each aged 16 or over and are “personally connected” to each other, and
-
(b) the behaviour is abusive.
(3) Behaviour is “abusive” if it consists of any of the following—
-
(a) physical or sexual abuse;
-
(b) violent or threatening behaviour;
-
(c) controlling or coercive behaviour;
-
(d) economic abuse (see subsection (4));
-
(e) psychological, emotional or other abuse;
and it does not matter whether the behaviour consists of a single incident or a course of conduct.
(4) “Economic abuse” means any behaviour that has a substantial adverse effect on B’s ability to —
-
(a) acquire, use or maintain money or other property, or
-
(b) obtain goods or services.
(5) For the purposes of this Act, A’s behaviour may be behaviour “towards” B despite the fact that it consists of conduct directed at another person (for example, B’s child).
(6) References in this Act to being abusive towards another person are to be read in accordance with this section.
(7) For the meaning of “personally connected”, see section 2.
Section 2: Definition of “personally connected”
(1) Two people are “personally connected” to each other if any of the following applies —
-
(a) they are, or have been, married to each other;
-
(b) they are, or have been, civil partners of each other;
-
(c) they have agreed to marry one another (whether or not the agreement has been terminated);
-
(d) they have entered into a civil partnership agreement (whether or not the agreement has been terminated);
-
(e) they are, or have been, in an intimate personal relationship with each other;
-
(f) they each have, or there has been a time when they each have had, a parental relationship in relation to the same child (see subsection (2));
-
(g) they are relatives.
(2) For the purposes of subsection (1)(f) a person has a parental relationship in relation to a child if —
-
(a) the person is a parent of the child, or;
-
(b) the person has parental responsibility for the child.
(3) In this section —
-
“child” means a person under the age of 18 years;
-
“civil partnership agreement” has the meaning given by section 73 of the Civil Partnership Act 2004;
-
“parental responsibility” has the same meaning as in the Children Act 1989; “relative” has the meaning given by section 63(1) of the Family Law Act 1996.
Section 3: Children as victims of domestic abuse
(1) This section applies where behaviour of a person (“A”) towards another person (“B”) is domestic abuse.
(2) Any reference in this Act to a victim of domestic abuse includes a reference to a child who –
-
(a) sees or hears, or experiences the effect of, the abuse, and
-
(b) is related to A or B.
(3) A child is related to a person for the purposes of subsection (2) if –
-
(a) the person is a parent of, or has parental responsibility for, the child, or
-
(b) the child and the person are relatives.
(4) In this section –
-
“child” means person under the age of 18 years;
-
“parental responsibility” has the same meaning as in the Children Act 1989 (see section 3 of that Act);
-
“relative” has the meaning given by section 63(1) of the Family Law Act 1996.
Annex E – Eligibility to access care and support under the Care Act 2014
153. Assessing needs can be done within people’s homes with families and friends or by social workers in the community or in health settings. This typically happens as someone gets older and their needs change incrementally. The statutory responsibility to assess care needs sits with local authorities.
154. Where the person meets the eligibility threshold to receive care and/or support, the local authority will conduct a means test to determine the cost of care and some people will be entitled to free care. The overarching principle is that people should only be required to pay what they can afford. Payment can also be made through a personal budget, which local authorities fund in part or whole. The individual will then decide how they choose to manage their personal budget.
155. Where an individual fails to meet the local authority threshold, they may need to purchase care for themselves (self-funders) or, in a number of cases, depend on family for care and support.[footnote 97], [footnote 98]
How are care assessments made?
156. Under the Care Act 2014, the local authority must carry out an assessment of anyone who appears to require care and support. The purpose of an assessment is to identify the person’s existing needs and how these impact on their wellbeing, and the outcomes that the person wishes to achieve in their day-to-day life. The assessment is done by measuring how someone is able to do daily tasks including:
-
managing and maintaining nutrition
-
maintaining personal hygiene
-
managing toilet needs
-
being appropriately clothed
-
being able to make use of the adult’s home safely
-
maintaining a habitable home environment
-
developing and maintaining family or other personal relationship
-
accessing and engaging in work, training, education or volunteering
-
making use of necessary facilities or services in the local community, including public transport, and recreational facilities or services
-
carrying out any caring responsibilities the adult has for a child
The local authority has a duty to provide assistance if someone is unable to meet two or more of these outcomes.[footnote 99]
157. The Care Act 2014 states that a local authority must arrange an independent advocate in certain circumstances to facilitate the involvement of a person in their assessment (section 67).[footnote 100] The Mental Capacity Act 2005 provides for an Independent Mental Capacity Advocate for all those who lack capacity in certain situations (sections 35-41 of the Mental Capacity Act 2005).
158. When someone is assessed to need care by their local authority, they will be assigned a ‘personal budget’. In some cases, people will use their personal budget to hire directly from a care agency or someone to provide care from their community or a personal assistant. Skills for Care, a workforce development and planning body for adult social care provides comprehensive information for employing personal assistants. The local authority may not necessarily know if someone has employed someone to provide care for them. People will make decisions to suit their own needs. There are situations where volunteers from charities provide care but the charity itself is paid by the local authority or health body.
Annex F - Types of abuse and neglect
159. The table below outlines forms of abuse and neglect as identified in the Domestic Abuse Act 2021 and statutory guidance, the Care and Support statutory guidance and the Equalities Act 2010.[footnote 101] [footnote 102]
| Type of abuse | Description |
|---|---|
| Physical abuse | Examples include: assault, hitting, slapping, pushing, misuse of medication, restraint and inappropriate physical sanction. |
| Domestic abuse | Domestic abuse can be physical, verbal, sexual, emotional, psychological, economic, a combination of these, and include many other forms of harmful behaviour. There is no one type of domestic abuse, nor is there one solution to remedy it. This is reflected in the statutory definition of domestic abuse as set out in the Domestic Abuse Act 2021, and further explained in the Domestic Abuse Act 2021 statutory guidance.[footnote 103] It sets out numerous forms of behaviour, any one of which can constitute domestic abuse, if both the victim and perpetrator are “personally connected”. |
| Sexual abuse | Examples include: rape, indecent exposure, sexual harassment, inappropriate looking or touching, sexual teasing or innuendo, sexual photography, subjection to pornography or witnessing sexual acts, indecent exposure, sexual assault, and sexual acts to which the adult has not consented or was pressured into consenting. |
| Psychological or emotional abuse | Examples include: emotional abuse, threats of harm or abandonment, deprivation of contact, humiliation, blaming, controlling, intimidation, coercion, harassment, verbal abuse, cyber bullying, isolation, unreasonable and unjustified withdrawal of services or supportive networks. |
| Financial or material abuse | Examples include: theft, fraud, internet scamming, coercion in relation to an adult’s financial affairs or arrangements, including in connection with wills, property, inheritance or financial transaction, and the misuse or misappropriation of property, possessions or benefits. |
| Modern slavery | Examples include: human trafficking, forced labour, domestic servitude, sexual exploitation (such as escort work, prostitution, pornography and debt bondage). |
| Discriminatory abuse | Examples include: harassment, slurs or similar treatment because of race, sex, gender identity, age, disability, sexual orientation or religion. |
| Organisational abuse | Includes neglect and poor care practice within an institution or specific care setting such as a hospital or care home, or in relation to care provided in one’s own home. This may range from one off incidents to on-going ill-treatment. It can be through neglect or poor professional practice as a result of the structure, policies, processes and practices within an organisation. |
| Neglect and acts of omission | Examples include: ignoring medical emotional or physical care needs; failure to provide access to appropriate health, care and support or educational services; or the withholding of the necessities of life, such as medication, adequate nutrition and heating. |
| Self-neglect | This covers a wide range of behaviours, neglecting to care for one’s personal hygiene, health or surroundings and includes behaviour such as hoarding. It should be noted that self- neglect may not prompt a section 42 enquiry. An assessment should be made on a case-by-case basis. A decision on whether a response is required under safeguarding will depend on the adult’s ability to protect themselves by controlling their own behaviour. There may come a point when they are no longer able to do this, without external support. |
Annex G – Agencies and organisations with safeguarding responsibilities
160. Safeguarding responsibilities cut across statutory agencies and government departments. The Care Act 2014 sets out that all public organisations should work together and co-operate where needed to ensure a focus on the care and support of adults (including carers’ support) and health and health-related needs of their local population.
161. The table below provides an overview of the roles and responsibilities of government departments to oversee safeguarding policy and law in England, as well as the regulators responsible for managing adult safeguarding concerns with their responsibilities outlined.
| Government department | Safeguarding responsibility |
|---|---|
| Department for Education (DFE) | Policy and legislation child safeguarding and protection. |
| Department of Health and Social Care (DHSC) | Responsible for policy and legislation regarding health and social care, including safeguarding adults with care and support needs. The department ensures adults with care and support needs are safeguarded when receiving health and social care services through their work with the following agencies and public bodies: the Care Quality Commission, NHS England and local authorities. The minister responsible for social care reform, including safeguarding adults receiving social care services at home, is the Minister for Care Services. |
| Home Office | Responsible for home affairs, including crime and policing, domestic abuse, and domestic homicide reviews. The Safeguarding Minister and Policing Minister are both situated within the Home Office. |
| Department for Levelling Up, Housing and Communities (DLUHC) | Responsible for housing policy, including homelessness. Works closely with the Local Government Association and includes oversight of the Local Government Body. |
| Public and independent bodies | Safeguarding responsibility |
|---|---|
| Care Quality Commission (CQC) | Ensures all registered health and social care providers, are delivering safe care, to a high standard by registering care providers, monitoring, inspecting and rating services and taking action to protect the lives of people who use the service. |
| Local authority social services | Local authorities have a statutory duty to safeguard and promote adults with care and support needs. This includes carrying out safeguarding enquiries and setting up Safeguarding Adults Boards. Local authorities and clinical commissioning groups already have an equal and joint duty to prepare Joint Strategic Needs Assessments and Joint Health and Wellbeing Strategies through health and wellbeing boards. |
| Local Safeguarding Adult Boards (SABs) | Under the Care Act 2014, local Safeguarding Adults Boards must lead adult safeguarding arrangements across its locality and oversee and co-ordinate the effectiveness of the safeguarding work of its member and partner agencies. Each Safeguarding Adults Board should have in place a framework to respond to allegations raised about a person who may have harmed or who may pose a risk to adults. |
| Police | Investigate allegations of criminal abuse against children and adults. The police have powers to initiate specific protective actions which may apply, such as Domestic Violence Protection Orders. |
| Disclosure and Barring Service (DBS) | Helps employers make safer recruitment decisions and prevent unsuitable people from working with adults at risk and children. The DBS maintains the ‘adults’ and ‘children’ barred lists. |
| Office of the Public Guardian (OPG) | Protects people in England and Wales who may not have the mental capacity to make certain decisions for themselves, such as about their health and finance. |
| NHS England | The NHS is a clinical commissioning body. GPs and hospitals provide care and are at the front lines of assessing clinical need. Under the NHS Act, NHS England must encourage partnership arrangements between Integrated Care Systems and local authorities where it considers this would ensure the integrated provision of health services and that this would improve the quality of services or reduce inequalities. |
Annex H – Homecare settings
Specialist types of home settings
162. The nature of some people’s care and support needs will mean that they need housing that is specifically designed to support independent, healthy living. This is generally known as supported housing.
163. There are different types of supported housing provision, and they vary according to the user’s care and support needs for independent living. At the end of 2015, there were an estimated 651,500 accommodation-based supported housing units in Great Britain, the majority of which (85%) are in England. An estimated 71% of units across Great Britain accommodated older people; 29% of units accommodated working-age people with a very wide range of support needs.[footnote 104]
Shared Lives and Homeshare
164. Shared Lives is a care and support service that matches people aged 16 and above who want to live independently in their community, with Shared Lives carers. It is a flexible model but generally people move in with their Shared Lives carers and are supported within the context of the carer’s home and family. Pairings are based on shared interests and lifestyles. Fewer than 1% of people drawing on long-term social care in England were supported by Shared Lives in 2020-21.[footnote 105]
165. Other shared living models include Homeshare programmes, which bring together people with spare rooms and individuals who are happy to lend a hand around the house in return for affordable accommodation.
Social housing
166. The Social Housing white paper sets out how the government expects landlords to work with other agencies such as local authorities to develop a policy setting out how they should tackle issues surrounding domestic abuse. There is also a government commitment from the housing sector to provide housing-related advice, for example, securing a permanent home and advice on how to live safely and independently and also the provision of counselling and therapy for both adults and children.[footnote 106]
-
Vulnerability Knowledge and Practice Programme. 2022. Domestic Homicide Project Spotlight Briefing #4: Carers. ↩
-
Public Health England. 2015. Disability and Domestic Abuse: Risk, impacts and response, Domestic Abuse Act 2021(GOV.UK); Home Office. 2022. Domestic Abuse: Statutory Guidance;, SCIE. 2015. Adult safeguarding practice questions. ↩
-
SafeLives. 2017. Disabled Survivors Too.pdf (safelives.org.uk);, SafeLives. 2016. Safe Later Lives - Older people and domestic abuse.pdf (safelives.org.uk).. ↩
-
Vulnerability Knowledge and Practice Programme. 2022. Domestic Homicide Project Spotlight Briefing #4: Carers ↩
-
DHSC. 2021. People at the Heart of Care: adult social care reform white paper. (GOV.UK). ↩
-
Adult Social Care Activity and Finance Report, England, 2021-22. (digital.nhs.uk);, Community Care Statistics, Social Services Activity, England - 2015-16. (digital.nhs.uk). ↩
-
Nicky Stanley, Christine Anne Barter, Nicola Farrelly, Claire Houghton, Leah McCabe, Franziska Meinck, Helen Richardson Foster, Sarah Shorrock. 2021. Innovation, Collaboration and Adaptation: The UK Response to Domestic Abuse under Covid-19; Corinne Peek-Asa, Anne Wallis, Karisa Harland, Kristen Beyer, Penny Dickey, Audrey Saftlas. 2011. Rural disparity in domestic violence prevalence and access to resources. J Womens Health. ↩
-
Based on NHS Digital Short and Long-term Support (SALT) data, available at Adult Social Care Activity and Finance Report (digital.nhs.uk). ↩
-
NHS Digital. 2021. Adult Social Care Activity and Finance Report: Detailed Analysis, England 2020- 21 (digital.nhs.uk). ↩
-
Adult social care charging reform: further details. 2022. (GOV.UK). ↩
-
Charging reform: government response to the consultation on ‘implementing the cap on care costs’ operational guidance. 2023. (GOV.UK). ↩
-
The Care Act 2014 section 10(9) defines a carer as an adult who provides or intends to provide care for another adult, but also states that if the care is provided under or by virtue of a contract or on a voluntary basis, then the adult should not be considered as a carer. However, section 10(9) states that “An adult is not regarded as a carer if the adult provides or intends to provide care – under or by virtue of a contract, or as voluntary work” s.10(10) states that in a case where the local authority considers that the relationship between the adult needing care and the adult providing or intending to provide care is such that it would be appropriate for the latter to be regarded as a carer, that adult is to be regarded as such (and subsection (9) is therefore to be ignored in that case). ↩
-
Unpaid carers may also be family members. Unpaid carers provide care for the person on an unpaid basis due to the person having a long-term condition. ↩
-
Care Quality Commission. 2022. Personal care (cqc.org.uk). ↩
-
More information about who CQC regulates can be found at Care Quality Commission. 2022. Personal care (cqc.org.uk). ↩
-
Office for National Statistics. Unpaid care, England and Wales (ons.gov.uk). ↩
-
DHSC modelling for 2022/23 based on Projections of Adult Social Care Demand and Expenditure 2018 to 2038. ↩
-
NHS Digital. 2020. Health Survey for England 2019 (digital.nhs.uk). ↩
-
ONS. 2020. Domestic abuse prevalence and victim characteristics (ons.gov.uk); SafeLives. 2015. Insights Idva National Dataset 2013-14. Bristol: SafeLives. ↩
-
Jane Monckton-Smith. 2018. Intimate Partner Femicide Timeline. In: UN Day Opposing Violence against Women Seminar and launch of the Femicide Watch 2018, Dublin. ↩
-
See Public Health England. 2015. Disability and Domestic Abuse: Risk, impacts and response Domestic Abuse Act 2021 (GOV.UK); SafeLives. 2017. Disabled Survivors Too.pdf SafeLives. 2016. Safe Later Lives - Older people and domestic abuse.pdf. Home Office. 2022. Domestic Abuse: Statutory Guidance; SCIE. Adult safeguarding practice questions. ↩
-
See SafeLives. 2017. Disabled Survivors Too.pdf (safelives.org.uk); SafeLives. 2016. Safe Later Lives - Older people and domestic abuse.pdf (safelives.org.uk); SCIE. Adult safeguarding practice questions. ↩
-
Janet Anand, Brian Taylor, Lorna Montgomery, Onder Bakircioglu, Colin Harper, John Devaney, Anne Lazenbatt, Katherine Pearson, Kathryn Mackay and Denis Nejbir. 2014. A Review of the Adult Safeguarding Framework in Northern Ireland, the UK, Ireland and Internationally.) Commissioner of Older People Northern Ireland (dickinsonlaw.psu.edu). ↩
-
Davidson, Phil Rossall and Sarah Hart. 2015. Financial Abuse Evidence Review. Age UK Research.) ↩
-
Home Office. 2022. Domestic Abuse: Statutory Guidance; SafeLives. 2017. Disabled Survivors Too (safelives.org.uk). ↩
-
Safeguarding Adult Reviews (SAR’s) – Swindon Safeguarding Partnership. ↩
-
Pseudonyms have been used in all case studies have in order to protect the anonymity and confidentiality of the individuals concerned. ↩
-
NHS Digital. 2022. Safeguarding Adults (digital.nhs.uk). ↩
-
Local Government Association – MSP is a sector-led initiative which aims to develop an outcomes focus to safeguarding work, and a range of responses to support people to improve or resolve their circumstances. ↩
-
Care and support statutory guidance – 1.27 The role of the Principal Social Worker in care and support (GOV.UK). ↩
-
For more information on SABs access SCIE’s guidance on Roles and Duties of Safeguarding Adult Boards. ↩
-
Disclosure and Barring Service (GOV.UK). ↩
-
A Multi-Agency Risk Assessment Conference (MARAC) is a non-statutory process that brings together statutory and voluntary agencies to jointly support adult and child victims of domestic abuse who are at a high risk of serious harm or homicide, and to disrupt and divert the behaviour of perpetrator(s). ↩
-
A Multi-Agency Safeguarding Hub (MASH) is one way of co-ordinating activity around safeguarding referrals, assessments and joined-up responses. Other local areas may call multi-agency safeguarding structures something different. These bring together expert professionals from a range of services that have contact with children, young people, adults and families, making the best possible use of their combined knowledge and information to safeguarding children who are at risk of harm or neglect. ↩
-
The Domestic Abuse Stalking and Harassment (DASH) risk assessment is one of the tools that professionals can use to help identify the level of risk an individual is facing and to tailor their support accordingly. The DASH risk tool is not a definitive assessment of risk but provides for the identification and assessment of risk based on structured professional judgement. ↩
-
Domestic Abuse Risk Assessment (DARA): Rationale for development, structure and content (college.police.uk). ↩
-
Introduction to Intelligence. Pre-read (college.police.uk). ↩
-
Skills for Care. 2022. Summary of domiciliary care services (skillsforcare.org.uk). ↩
-
National Audit Office. 2021. The adult social care market in England (nao.org.uk). ↩
-
‘By and for’ services are specialist services that are led, designed and delivered by and for the users and communities they aim to serve (for example, survivors from ethnic minority backgrounds, deaf and disabled victims and LGBT victims). ↩
-
Domestic Abuse Commissioner. 2022. A Patchwork of Provision. ↩
-
Tackling violence against women and girls strategy. 2021. (GOV.UK). ↩
-
Victims Funding Strategy. 2022. (publishing.service.gov.uk). ↩
-
SCIE. Safeguarding Adult Reviews (SARs) In Rapid Time. 2023 ↩
-
SCIE. Safeguarding adults. ↩
-
Care Quality Commission. 2022. Key questions and quality statements. (cqc.org.uk). ↩
-
National Network for Chairs of Adult Safeguarding Boards. www.nationalnetwork.org.uk. ↩
-
Local Government Association. National Escalation Protocol for Issues from Safeguarding Adults Reviews from Safeguarding Adult Boards. ↩
-
Safeguarding Adult Review Quality Markers are a tool used to support people involved in commissioning and conducting SARs. www.scie.org.uk). ↩
-
Local Government Association. Analysis of Safeguarding Adult Reviews: April 2017 - March 2019. ↩
-
Domestic Abuse Commissioner. 2022. A Patchwork of Provision. ↩
-
NHS Digital. Adult Social Care Activity and Finance Report, England, 2021-22 (digital.nhs.uk). ↩
-
Carers UK State of Caring 2022 (carersuk.org). ↩
-
Carers UK. 2021 Evidence review for adult social care reform (publishing.service.gov.uk). Carers UK State of Caring 2022 (carersuk.org). ↩
-
NHS Digital. Personal Social Services Survey of Adult Carers in England, 2021-22 (digital.nhs.uk). ‘SACE is representative of adult carers known to their local authority rather than all carers in England’. ↩
-
CPEC. 2020. Supporting carers following the implementation of the Care Act 2014: eligibility, support and prevention. ↩
-
Carers UK State of Caring 2022 (carersuk.org). ↩
-
Public Health England. 2021. Caring as a social determinant of health (publishing.service.gov.uk). ↩
-
Research in Practice. Supporting evidence-informed practice www.researchinpractice.org.uk.. ↩
-
Pseudonyms have been used in all case studies have in order to protect the anonymity and confidentiality of the individuals concerned. ↩
-
Camden Safeguarding Adults Partnership Board. 2015. Serious Case Review in respect of ZZ. ↩
-
Ministry of Justice. 2022. Achieving Best Evidence in Criminal Proceedings. ↩
-
Draft MCA Code of Practice: summary. 2022. (GOV.UK). ↩
-
University of Bristol. 2022. Mental Capacity, Self-Neglect, and Adult Safeguarding Practices: Evidence Synthesis and Agenda for Change. ↩
-
Pseudonyms have been used in all case studies have in order to protect the anonymity and confidentiality of the individuals concerned. ↩
-
London Borough of Barnet. 2022. Financial Abuse and Safeguarding: NCL SAB workshop findings report, Fiona Bateman. ↩
-
Andy Myhill and Katrin Hohl. 2019. The “Golden Thread”: Coercive Control and Risk Assessment for Domestic Violence, Journal of Interpersonal Violence, Volume 34, Issue 21-22 pages 4477-4497. ↩
-
Home Office, NPCC, College of Policing. 2021. Vulnerability Knowledge and Practice Programme (VKPP): Domestic Homicides and Suspected Victim Suicides During the Covid-19 Pandemic 2020-2021. ↩
-
Domestic Abuse Protection Notices / Orders factsheet. 2022. ↩
-
Madeleine O’Keeffe, Amy Hills, Melanie Doyle, Claudine McCreadie, Shaun Scholes, Rebecca Constantine, Anthea Tinker, Jill Manthorpe, Simon Biggs and Bob Erens. 2007. UK Study of Abuse and Neglect of Older People Prevalence Survey Report. ↩
-
Claudia Cooper, Amber Selwood and Gill Livingston. 2008. The prevalence of elder abuse and neglect: a systematic review. Age and Ageing, 37(2), pages151-160. ↩
-
ONS. 2022. Domestic abuse prevalence and victim characteristics (ons.gov.uk). ↩
-
NHS Digital. 2022. Safeguarding Adults. ↩
-
SafeLives. MARAC data 2021-2022 England and Wales. ↩
-
Unpublished data is not reconciled and is subject to change. Data is not available for the following police forces for the time period: Greater Manchester, Kent, Staffordshire, West Midlands and Wiltshire. ↩
-
The total number of offences a defendant is prosecuted for (principal offences plus non-principal offences). There is only detailed prosecution and conviction data for all offences. ↩
-
Ministry of Justice. 2022. Outcomes by Offence 2017 to 2021: Pivot Table Analytical Tool for England and Wales (GOV.UK). ↩
-
Andrew Hutchison Biza Stenfert Kroese. 2015. A review of literature exploring the possible causes of abuse and neglect in adult residential care. The Journal of Adult Protection. Volume 17, Issue 4 pages 216 to 233. ↩
-
Also see Catherine Hawes. 2003. Elder Mistreatment: Abuse, Neglect, and Exploitation in an Aging America - PubMed. ↩
-
Also see Kateřina Ivanová. 2009. Elder Abuse and Mistreatment in Residential Settings.. ↩
-
Also see Wenche Malmedal, Astrid Kilvik, Gunn Steinsheim, Anja Botngård. 2020. A literature review of survey instruments used to measure staff‐to‐resident elder abuse in residential care settings; Britt-Inger Saveman, Sture Åström, Gösta Bucht and Astrid Norberg. 2008. Elder Abuse in Residential Settings in Sweden: Journal of Elder Abuse & Neglect: Volume 10, No 1-2 (tandfonline.com). ↩
-
Adult safeguarding policy and law - Research Portal, King’s College, London (kcl.ac.uk). ↩
-
Organizational dynamics of respect and elder care - Social Care Online. ↩
-
Vulnerability Knowledge and Practice Programme. 2022. Domestic Homicide Project Spotlight Briefing #4: Carers. ↩
-
The VKPP’s analysis is of a total of 470 domestic-abuse related deaths recorded between 1st April 2020 and 31st March 2022. Of these, 79 victims (17%, over one in six) were either cared-for by the suspect of were the carer of the suspect. In the year ending March 2022, there were a total of 134 domestic homicides. Homicide in England and Wales - Office for National Statistics (ons.gov.uk). ↩
-
Home Office. 2022. Key findings from analysis of domestic homicide reviews: October 2020 to September 2021 (GOV.UK). ↩
-
Care Quality Commission. 2022. Key questions and quality statements. (cqc.org.uk). ↩
-
Research in Practice. Supporting evidence-informed practice. ↩
-
For more information on charging and financial assessments, access chapter 8 of the Care and Support statutory guidance 2014 (GOV.UK). ↩
-
The Care and Support (Assessment) Regulations 2014 (legislation.gov.uk). ↩
-
For further information on types of abuse and neglect, access the Social Care Institute for Excellence’s guidance. Types of abuse: Safeguarding adults www.scie.org.uk). ↩
-
Domestic Abuse Act statutory guidance (GOV.UK). ↩
-
Ipsos. 2016. Research estimates the scale, scope and cost of the supported housing sector. ↩
-
Shared Lives Plus. Report: The state of Shared Lives in England in 2020-2021 - Shared Lives Plussharedlivesplus.org.uk). ↩
-
For more information on homecare settings, access The Department of Levelling Up, Housing and Communities and Ministry of Housing, Communities & Local Government’s guidance on Housing for Older and Disabled People. ↩