
Near miss with track worker at Euxton Junction, Lancashire, 14 March 2024
Published 19 June 2024

© Crown copyright 2024
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/safety-digest-052024-euxton-junction/near-miss-with-track-worker-at-euxton-junction-lancashire-14-march-2024
1. Important safety messages
This incident demonstrates the importance of:
- following good ‑safety critical communication when undertaking face-to-face briefings, regardless of familiarity with the task, location or staff involved
- the provision of safe work packs containing information that is relevant, and which accurately reflect the needs of the work to be undertaken, such as the location of key equipment.
2. Summary of the incident
At around 14:14 hrs on 14 March 2024, the driver of a train reported a near miss with a track worker near to Euxton Junction on the West Coast Main Line. The track worker involved was a controller of site safety (COSS). At the time of the near miss, the COSS had been looking for a lineside location cabinet (LOC) to undertake scheduled maintenance work.
The COSS was alerted to the approaching train, which was travelling at 110 mph (177 km/h), by a shouted warning from a member of the public on a nearby footbridge and by the train driver sounding the train’s warning horn. The COSS managed to move to a position of safety approximately 2 seconds before the train reached their location.
3. Cause of the incident
This incident occurred because the COSS misidentified which of the railway lines at the location had been blocked to the passage of trains (known as a line blockage). Although signage at one of the access points used by the team correctly showed the layout of the track, the COSS did not recognise the error. The error was also not challenged by the other member of the team during a briefing given by the COSS.
The site of the incident was close to Euxton Junction, south of Preston. There are four railway lines at this point. The lines relevant to this incident are designated as the Up Fast and the Down Fast. The other two lines are designated as the Up Slow and the Down Slow.
The train involved in the near miss was train reporting number 1M12, the 11:36 hrs Glasgow Central to London Euston service, operated by Avanti West Coast. At the time of the incident, it was traveling southwards on the Up Fast line after leaving Preston station.
The Network Rail team involved in the incident consisted of two staff. These were the COSS, who was also the team leader, and a technician. At the time of the incident, a third member of the team was not on the lineside, and so was not involved.
The planned safe system of work (SSOW) had been sent to the COSS as part of a safe work pack (SWP). This pack contained details of three SSOWs which were to be used as part of the work. These included a separated system of work which, at the incident location, would have required the team to keep at least 2 metres between the site of work and the nearest running rail of the adjacent open line. The SWP also included one planned line blockage for the Up Fast line, and a second for the Down Fast line to allow other items of work to take place closer to the lines concerned.
At around 12:00 hrs on the day of the incident, the COSS reported for duty at the Network Rail depot located near Preston station. The team received a work order requiring them to conduct two separate items of maintenance work, testing within a LOC, and a track circuit inspection. Both items were in the same area.
The COSS and the other team members are locally based and familiar with the area where the incident took place. However, the COSS could not recall previously going to the specified LOC and was unaware of its precise location. For this reason, the COSS checked the location of the LOC before leaving the depot. However, in doing so, the COSS inadvertently checked the location of a different LOC which was not relevant to the work. This was located next to a down line on another section of railway which had a different engineer’s line reference. The COSS also had a conversation with a colleague about where the LOC was positioned in relation to the access point. Based on these pieces of information, the COSS departed the depot with the incorrect understanding of where the LOC they needed to work on was positioned, including that it was located next to a down line.
The SWP stated that entry to the railway was planned to be made at an access point called Old School Lane, near the LOC the COSS believed they were to work on. On arrival at the access point, the COSS checked the general information board to confirm that they were at the correct location. They then checked the LOC nearest the access point and realised that it was not one they were required to work on. However, the COSS saw a second LOC a short distance to the north. The COSS believed that this second LOC was the one that they were required to work on.
The COSS decided that the work on this second LOC could be done by two people working under the planned separated safe system of work. This information was then briefed to the team, along with the nature of the work. No information was given in this briefing concerning the names of the lines at the location, and no mention was made of any arrangements to take line blockages.
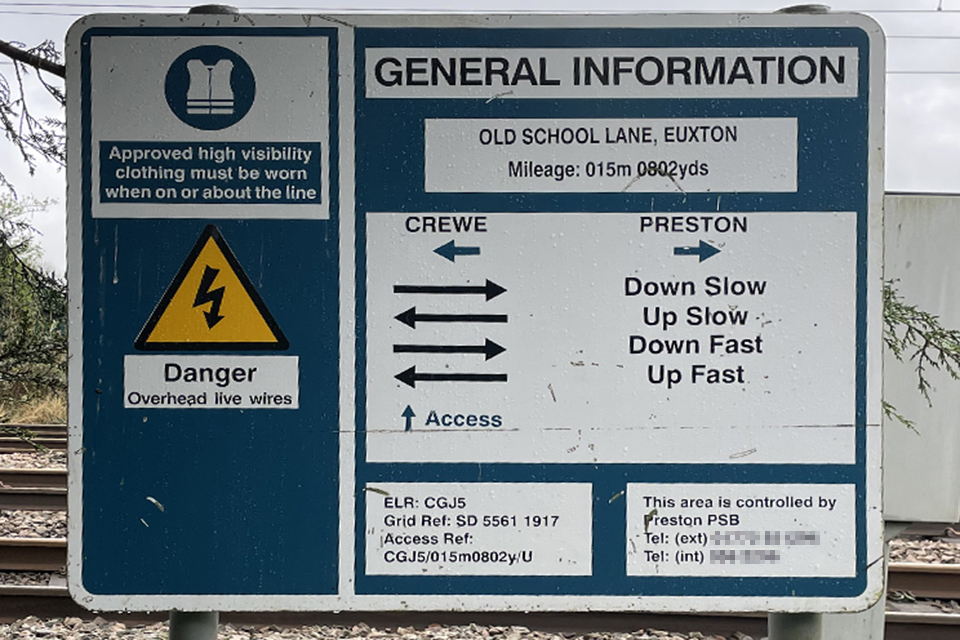
Old School Lane access point general information board.
The general information board provided at the Old School Lane access point indicates that the railway line closest to the access point is the Up Fast line. However, the COSS remained certain that the LOC they were required to work on was adjacent to a down line, and that the nearest line to the access point was therefore the Down Fast.
Having entered the railway at Old School Lane, the COSS and the technician walked north, adjacent to the Up Fast line, towards the second LOC. However, they found that they were unable to reach it safely due to the area of limited clearance between the Up Fast line and a structure (Oak Avenue footbridge). This meant there was no position of safety throughout the length of the structure. There were two access points adjacent to this footbridge, one on either side of the limited clearance, which would have allowed the team to bypass the structure. However, the southernmost of these access points was found to be secured out of use. The team therefore decided to return to the original access point at Old School Lane, and to use public roads to walk north to reach the access point beyond Oak Avenue footbridge. There was no general information sign showing the layout of the railway at this access point.

View from Oak Avenue footbridge, looking towards the south. Railway lines, from left to right, are Up Fast, Down Fast, Up Slow and Down Slow. Old School Lane access point is to the left of centre behind the white cabin.
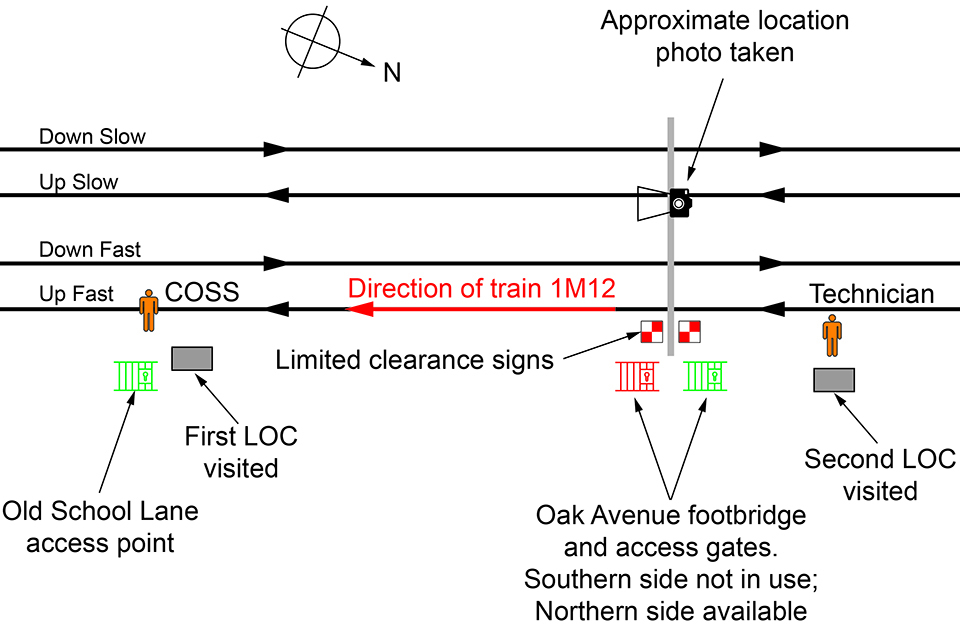
Diagram showing location layout and points of interest, staff positions shown at time of incident. Not to scale.
The team reached the Oak Avenue access point and re-entered the railway. Having reached the second LOC and opened its doors, the team recognised that it contained the wiring for the track circuit that they needed to inspect, which was on the Down Fast line. This track circuit inspection required access to the track itself and the decision was made by the COSS to request a line blockage to prevent the passage of trains for the duration of the work.
At this point, the COSS still believed that the line closest to the LOCs was the Down Fast line. The COSS called the signaller located at Preston and requested that the Down Fast line was blocked. This was granted by the signaller at 13:54 hrs.
The COSS then briefed the technician about the line blockage. However, the COSS did not use the terms Down Fast (or Up Fast) when doing so but instead referred to the blockage as being on the ‘closest line’. The technician did not challenge the COSS during the briefing, nor raise any concerns about which line was blocked to the passage of trains.
A visual inspection was made of a track circuit, although the team were unaware that the equipment examined was actually located on the Up Fast line and not on the (blocked) Down Fast line. The COSS then decided to walk back south towards the Old School Lane access point in search of the LOC which the team still needed to access for the other maintenance task. In doing so, the COSS walked between the rails of the Up Fast line, which was open to rail traffic, still believing that it was the blocked Down Fast line. The COSS was also walking with their back towards any trains that would approach on the Up Fast line.
As the COSS walked southwards, train 1M12 approached at 110mph (177 km/h), within the permissible line speed of 125 mph (201 km/h). As the train approached, it was seen by the technician, who expected it to be routed onto another line. Once the technician realised that the train was continuing on the Up Fast line, they shouted a warning to the COSS. However, the COSS was too far away to hear this warning.
The COSS reported seeing a member of the public on Oak Avenue footbridge who they heard shouting to them that a train was approaching. The COSS ignored this warning, assuming the train was on another line, as they were certain that the line they were on was blocked. The COSS then heard the train’s warning horn. They acknowledged this warning without looking for the train which had sounded it. The train driver at this point realised the COSS was not moving to a position of safety and so had already started to sound the warning horn again, as well as applying the train’s brakes.
As the train got closer the COSS realised their error and managed to move to a position of safety approximately 2 seconds before the train passed them.
The SWP issued to the team included details on the precise location of the access points, but there were no details of the location of any lineside equipment related to the tasks which were being completed. The work order given to the COSS only gave the line reference number but no further details on equipment location. This meant that the COSS had to look up the information themselves and made an error in doing so. Even though information was available at one of the access points which could have highlighted this error, this misunderstanding about the location of line persisted once the team reached site. It ultimately led to the COSS walking without protection on a line open to traffic on which trains could travel at 125 mph (201 km/h).
The team had worked together for a number of years and were familiar with each other and the location. It was reported that they are all willing, and have, challenged errors in previous briefings. It is therefore probable that, if line names had been used by the COSS in their safety briefing, then the technician, or even the COSS themselves would have realised the misidentification of the line which had occurred.
4. Previous similar occurrences
Many incidents and accidents involving track workers have previously been investigated by RAIB. Some of these incidents resulted in fatalities or had the potential to do so. Those with similarities to the incident at Euxton Junction include:
- In August 2017, a passenger train collided with three engineering trolleys on the Settle Junction to Carnforth line, at Clapham in North Yorkshire (RAIB safety digest 16/2017). This collision occurred because the COSS involved had an incorrect understanding of which of the two lines was the Down line when they handed it back.
- In November 2018, a passenger train struck and fatally injured a track worker in the vicinity of Stoats Nest Junction, near Purley (RAIB report 07/2019). The accident occurred after the track worker had placed protection on the track as part of an engineering possession. Having placed the protection equipment, the track worker walked along the track until they reached the end of the protected area and continued walking with their back to rail traffic on an open line. The track worker was probably fatigued when the accident occurred.
- In December 2018, two track workers narrowly avoided being struck by an express passenger train that was travelling at about 100 mph (161 km/h) on the Midland Main Line near the village of Sundon, Bedfordshire (RAIB safety digest 05/2019). The near miss occurred because the track workers were walking along a line open to traffic in the mistaken belief they were on a line which was closed to traffic.
A wider summary of previous RAIB learning, including further similar incidents relating to protection of track workers from moving trains, can be found on the RAIB website.