
Passenger train derailment at Bognor Regis station, West Sussex, 22 October 2020
Published 17 December 2020

© Crown copyright 2020
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/safety-digest-082020-bognor-regis/passenger-train-derailment-at-bognor-regis-station-west-sussex-22-october-2020
1. Important safety messages
This accident highlights the following safety learning:
- During degraded operations (such as when providing verbal authority for a train to pass a signal at danger), it may not be appropriate to rely on the protection normally offered by the interlocking. It is therefore important that signallers use all available information, including points indicators, to ensure that a route is correctly set before giving permission for a train to pass over it
- It is important that signaller competence management systems impart and maintain required levels of knowledge and familiarity for signallers to operate all signalling locations for which they are authorised, especially where equipment may not operate in ways that signallers would normally expect
- When short-notice changes to working patterns are necessary to cover staff shortages, it is important that the risk of fatigue is managed appropriately. In accordance with Network Rail’s standard on fatigue risk management, roster amendments should be made to minimise the build-up of fatigue and, where resource shortages are likely to be prolonged, the actual hours worked should be reviewed and the roster amended. The amendments should be risk assessed, and control measures put in place to manage identified fatigue risks.
2. Summary of the accident
At around 05:14 hrs, train 2P03, the 05:05 hrs passenger service from Bognor Regis to Littlehampton, derailed around 58 metres from its departure point in platform 4 at Bognor Regis station. There were two members of staff and about 12 passengers on board, all of whom evacuated via the rear portion of the train, which was still in the platform. No one was injured.

The derailed leading end of the train
The train, a three-car class 313 electric multiple unit, was travelling at approximately 5 mph (8 km/h) at the time of the accident. All four wheels of its leading bogie derailed on points, numbered 32B, a short distance beyond signal BR12, which is the platform 4 starting signal.
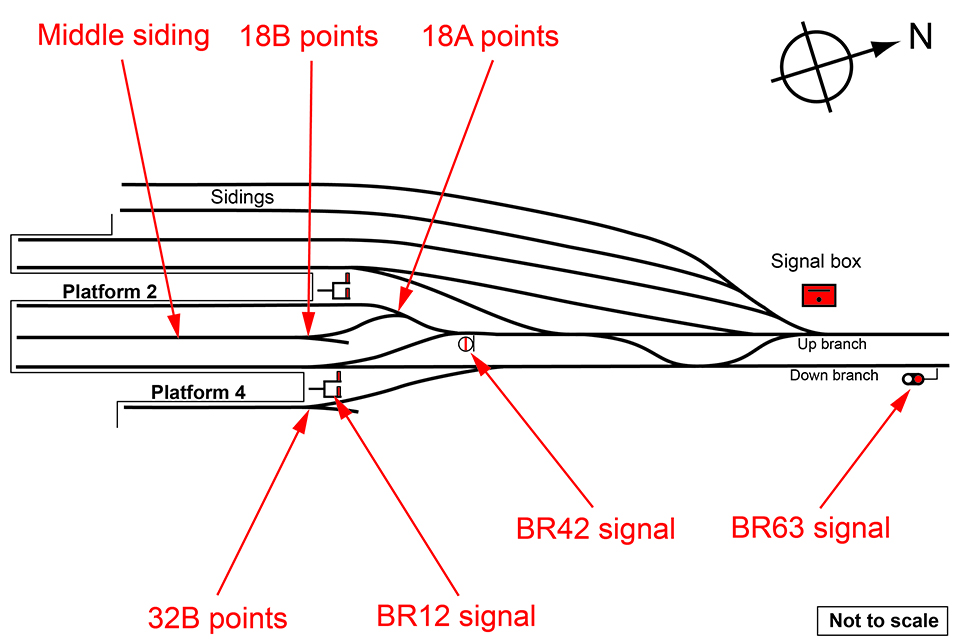
Simplified track diagram showing platforms 2 and 4, the middle siding, signals BR12, BR42 and BR63, and points 18A, 18B and 32B
3. Cause of the accident
Bognor Regis station is the terminus of a short branch line from Barnham, which is on the line between Brighton and Portsmouth Harbour. The signal box, located just outside the station, has a lever frame to control the signals and points in the station area. The signaller on duty on the morning of the accident started work at 04:30 hrs, having been called in at short notice the evening before to cover a staff shortage. He was a relief signaller, who had joined the railway in July 2018 and was passed as competent to operate Bognor Regis signal box in February 2020.
A few minutes before the accident another train, 5P17, the 04:57 hrs empty passenger train movement from Barnham, was approaching the station at Bognor Regis. The signaller at Bognor Regis tried to set a route for this train into platform 2, but found that he could not clear the associated signals, so he gave the train’s driver verbal authority to pass signals BR63 and BR42 at danger (red). These signals could not be cleared to a proceed aspect because of a fault on 18A and 18B points which lead from platform 2 to the middle siding, but the signaller was not aware of this.
The problem with 18 points meant that the train was instead directed into the middle siding. 18B points were damaged as a result of train 5P17 running through them when they were not properly set for this movement.
While the signaller had been dealing with the approach of train 5P17 and its arrival at Bognor Regis station, the departure time for train 2P03 from platform 4 had passed. The signaller found that he was also unable to clear signal BR12. Consequently, he gave verbal authority for the train to pass signal BR12 at danger. However, the signaller did not realise that the reason he could not clear signal BR12 was because 32B points were not in a secure position for this train’s movement, and the electrical interlocking prevented signal BR12 from being cleared.
Points 18A, 18B and 32B are driven by electric motors, which are all powered by the same set of batteries. One of these batteries had failed so that, when the signaller tried to set the routes for trains 5P17 and 2P03, there was not enough energy available to set and lock the points in the reverse position. Train 5P17 was diverted into the middle siding because 18A points had not moved into the normal position, while train 2P03 derailed because 32B points had moved into an intermediate position, allowing the leading wheels to fall in between the rails. Neither train driver was able to see the position of the points clearly because it was dark at the time.
Above the lever frame in the signal box are indicator lights showing whether each set of points has been detected in either its normal or reverse position. After the accident, the indicators for both 18 and 32 points were found to be blank, meaning that neither of these sets of points were detected in a correct position. It is likely that these indicators were also blank before the movement of the two trains. However, the signaller did not notice this, partly because he was relying on the position of the levers, and partly because he was under increasing time pressure as well as probably being fatigued.

Indicators for 18, 21 and 32 points as observed after the accident. The indicators for 18 points (left) and 32 points (right) are blank, showing no detection of these points, whereas that for 21 points (middle) is lit with ‘N’ for normal position.
The signaller was not aware of the problem with the points because he had been relying on the position of levers in the signal box that are used to control the points, rather than checking that the points indicators were illuminated. An informal, locally-produced reference sheet in the signal box described all the lever movements that were necessary for a given train movement, and the signaller repeatedly consulted this sheet to check that he had carried out the correct actions. Because all the levers were in the correct positions according to the sheet, the signaller believed that the routes for each train were correctly set. However, the signaller did not recognise that, because the points at Bognor Regis involved in this accident are motorised, the position of the point levers only served as a reminder that he had commanded the points to move. The lever position does not necessarily reflect the actual position of the points on the ground, as it would if a mechanical linkage was in place and working correctly.
The need to provide verbal authority for train 5P17 to pass two signals at danger increased the workload on the signaller. It also delayed the arrival of that train, so that it coincided with the timetabled departure time of train 2P03. The signaller was conscious of the delay that was building for train 2P03, especially given the difficulty in clearing signal BR12 for it to depart from platform 4.
It is also likely that the signaller was fatigued. His previous duty was a night shift finishing at 06:00 hrs on 21 October 2020, with the remainder of that day being a rostered rest day. He returned home and obtained a few hours’ sleep before waking mid-morning to attend an appointment. He stayed awake for the rest of the day as he was rostered on a spare duty, with no work planned, on 22 October. However, on the evening of 21 October, the signaller’s manager contacted him to ask if he could cover the early hours at Bognor Regis, due to chronic staffing problems in the area. The signaller agreed and went to bed around 22:00 hrs, waking up at 03:50 hrs to start work at the signal box at 04:30 hrs.
4. Previous similar occurrences
A freight train derailment on 10 November 2008 at East Somerset Junction was caused when a signaller, who was probably fatigued, did not operate a set of points to the correct position for the safe movement of the train. RAIB report 28/2009 identified the signaller’s rostering as a probable causal factor, as he had been working alternating six- and 12-hour night shifts on multiple and consecutive occasions in the days and weeks before the accident. The report made several recommendations to improve Network Rail’s rostering and fatigue risk management. Network Rail has since revised its fatigue risk management processes, with its current standard setting out principles including, with particular relevance to the accident at Bognor Regis on 22 October 2020, the assessment of fatigue for short-notice changes to working patterns.
RAIB bulletin B04/2009 describes the derailment of a passenger train departing from platform 2 at Bognor Regis station, which occurred on 14 November 2008. This derailment occurred under different circumstances to the accident on 22 October 2020 as, at the time, special working arrangements were in place due to re-signalling work at Barnham.
On 7 November 2015, a passenger train derailed at Knaresborough, North Yorkshire, after a signaller had given it authority to pass a signal at danger without realising that the points beyond the signal were not in a secure position. As with the signaller at Bognor Regis on 22 October 2020, the Knaresborough signaller had misinterpreted the significance of being able to operate the signal lever, leading him to believe that the route was correctly set, and had not checked the associated points position indicator. The signaller in Knaresborough signal box that day was not a permanent signaller, but was covering the duty due to a lack of available staff, and operated signal boxes infrequently. RAIB report 16/2016 into the Knaresborough derailment made one recommendation, addressed to Network Rail, with the intent of ensuring that signal boxes are always operated by members of staff who have the necessary knowledge and familiarity with the signal box and its operation.
RAIB safety digest D03/2019 describes the derailment of a passenger train at Penryn, Cornwall, on 28 January 2019. The signaller involved was unable to clear a signal for the train and so authorised it to pass the signal at danger. However, the associated points were in an intermediate position due to a technical failure, leading to the derailment. Similar to the situation at Bognor Regis, the levers in the signal box were mechanically interlocked but the controls associated with the points detection did not prevent the signal lever from being reversed, although the colour light signal remained at red.
5. Observations
Many of the sets of points at Bognor Regis, including some of those involved in this accident, were converted from mechanical to motor operation between 2009 and 2012. When this work was carried out, the mechanical locking between the levers was not altered, and so the levers which formerly worked mechanical facing point locks still have to be pulled by the signaller, to release other levers which operate signals. Facing point locks are devices which secure facing points in the correct position.
Network Rail company standard NR/L2/SIG/11201/Mod A5-5 ‘Signalling Design Handbook: Signalling Control Centres’, defines the requirements for levers in such a situation: they should have information on them describing their function (section 5.1); they should be described on the layout diagram in the signal box (section B1.4); and where they are worked to maintain the locking they should be painted white at the top and the colour associated with their original function at the bottom (section B1.9). At Bognor Regis, the former facing point lock levers were still painted all-over blue, badged with their previous function with small tape labels added, and were not described on the signal box diagram.
It was apparent from witness evidence that the function of the former facing point lock levers, and the reasons why they had to be worked, were not understood by some of the signallers at Bognor Regis. The obsolete labelling and lack of description of the levers may have contributed to this.

Example of the labelling on the blue facing point lock levers in Bognor Regis signal box