
Near miss between Audley End and Great Chesterford, 21 April 2017
Published 9 August 2017

© Crown copyright 2017
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/safety-digest-122017-great-chesterford/near-miss-between-audley-end-and-great-chesterford-21-april-2017
1. Important safety messages
This incident demonstrates the importance of:
-
ensuring that planning documentation is appropriate to the task that is to be performed, taking into account the nature of the work activity and the characteristics of the site of work (such as limited sighting of approaching trains)
-
correctly positioning appropriate lookouts, after properly considering how they can both obtain adequate sighting of approaching trains, and reliably communicate with the group that they are protecting
-
regular reassessment of sighting, and a review of the lookout arrangements, by the person in charge of safety as mobile work activities proceed along the line
The incident also reinforces the findings of the RAIB’s recent investigation into track worker safety (RAIB report 07/2017). In particular:
-
the risk that people in charge of safety at a site of work can become preoccupied with the task, which can mean that a safe system of work (SSOW) is not effectively monitored and maintained
-
the need to ensure that people who are in charge of safety at a site of work have the skills and knowledge needed to recognise and respond appropriately to local circumstances, and any subsequent changes that may occur
-
the need to review whether enhanced competence reuirements are necessary for those in charge of safety when working on lines that are still open to traffic
2. Summary of the incident
At 11.33 hours on Friday 21 April 2017, a group of track workers narrowly avoided being struck by a train travelling at approximately 73 mph (117 km/h). The track workers and site lookout did not see or hear any warning provided by the distant lookout, and only became aware of the train because the train driver saw the track workers and continuously sounded the train’s horn. The group moved to a position of safety with less than two seconds to spare, as the train approached and passed the site of work.
The work group consisted of a controller of site safety (COSS) and four other members of staff. The group was measuring the height and stagger of the overhead line equipment (OLE), which involved them being in the four-foot (between the rails) of both lines. The COSS had briefed the group at the depot before travelling to an access point about 200 metres north of Littlebury Tunnel. The planned safe system of work involved working under the protection of lookouts, as the site of work moved along over 2 miles 10 chains (3.4 km), going outward on the up line and returning on the down line. The work on the up line was completed without incident, and the group then proceeded to the second phase of work on the down line, moving south along the line (ie in the up direction, towards London).
For this stage of the work, the COSS implemented a protection system incorporating both a site lookout (close to the group and looking for trains on the up line) and a distant lookout (looking for trains on the down line, and positioned in the up cess, about 180 metres to the south, ahead of the work group). The COSS and two members of staff then undertook work in the four-foot of the down line using optical surveying equipment.
The driver of train 2H20, the 10:28 hrs Abellio Greater Anglia service from London Liverpool Street to Cambridge, reported that after the train came out of Littlebury Tunnel on the down line, he sounded the train’s horn. He then saw a track worker at the side of the up line (the distant lookout) who did not appear to be looking in his direction or aware of the train. He sounded the train’s horn again as the track gang came into view a short distance ahead of him on the down line.
The forward facing CCTV from the train (figure 2) shows the position of the distant lookout at the lineside, about 30 metres beyond a bridge pier. Several staff can be seen in the four-foot of the down line (which is on the inside of the curve). The distant lookout is looking in the direction of the group as the train passes his location (figure 1). The work group then appear to react to the approach of the train, approximately five seconds before it passes them. The work group then move clear of the line and reach a position of safety when the train is only about 60 metres, or 1.8 seconds running time, from the place where they had been working.
3. Cause of the incident
The incident occurred because the COSS had not set up a safe system of work in accordance with the rules.
The COSS was provided with a planning document known as the SSOW pack, which included a RT9099 ‘COSS Record of Arrangements and Briefing Form’. This form gave details of the line speed in the area, and specified a single lookout to provide warning of approaching trains.
When deciding where to position the lookouts, the COSS was required to calculate the required sighting. This calculation is required to determine the warning needed to provide sufficient time for all staff to reach a position of safety at least 10 seconds before a train reaches the site of work.
The COSS wrote down that a warning time of 20 seconds (and therefore a sighting distance of 880 yards) was required. He did not record how he had arrived at this figure.
Due to the curvature of the track on the down line, and various bridges which hampered visibility (figure 1), the COSS decided to appoint a site lookout and a distant lookout, and instructed the distant lookout to stand three to four OLE spans (about 180 metres) away from the group, on the far side of the opposite line. The distant lookout was instructed to warn the site lookout of trains approaching on the down line. The site lookout would then warn the group to move clear of the line. Because the site lookout was instructed to look out for trains on the up line, and would therefore not be facing the distant lookout, the COSS instructed the distant lookout to use his horn to warn of the approach of trains, rather than the blue and the white chequered flag which is normally used to give this warning. The COSS did not consider in detail how the visibility available to both lookouts would change as the group moved along the line, or the implications of the distant lookout’s visibility being restricted by the curvature of the line or by the bridges.
The rule book (Handbook 7) requires the COSS to position a distant lookout in an appropriate position, and that the distant lookout should use a flag to warn the site lookout when a train approaches. However, in this case the COSS had instructed the distant lookout to use his horn to give the warning, and the flag was not used. The group stated that they had tested this method of warning before starting work. The RAIB also understands from witness evidence that the group had used this non-compliant method of warning before.
The curvature of the track at the location of the incident meant that the distant lookout would have been able to see the train when it came into view about 400 metres away from him. Taking into account his distance from the rest of the group, this would have enabled him to give the work group about 16 seconds warning of the approach of a train travelling at 80 mph (129 km/h). This warning was 4 seconds less than the time warning time recorded by the COSS on the RT9909 form. Soon after this, the bridge pier would have obstructed his view of the train until it was about 100 metres from him (figure 1).
When the train came into his view, the distant lookout used his horn to try to warn the group, but witness evidence indicates that ‘sudden windy conditions’ within the cutting meant that they did not hear the warning and were therefore unaware of the approaching train. The distant lookout realised that the site lookout and the group had not acknowledged his warning, so he blew a series of short blasts on the horn which the group also did not hear. The group only began to move clear when they heard the train’s horn and saw it approaching under the bridge (figures 2a to 2d).
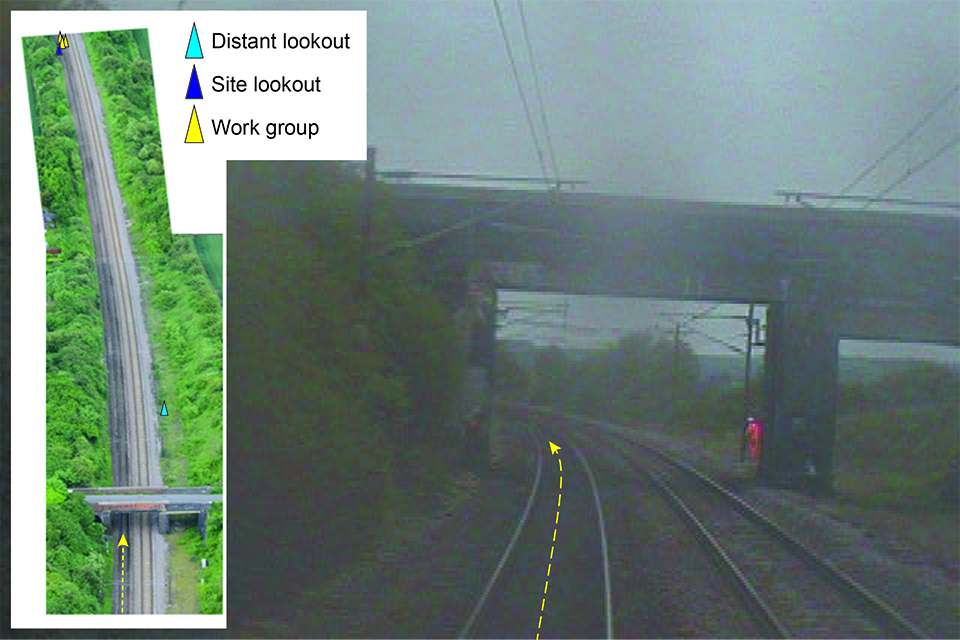
Figure 1: Image from FFCCTV (11:32:53 hrs) from train on the down line. Distant lookout is visible in the up cess (image courtesy of Greater Anglia). The inset image shows aerial view of bridge 1525 and position of the distant lookout.
The sighting distance calculation charts in the rule book, and reproduced in form RT 9909, state that 750 metres (or 800 yards) sighting distance is necessary to provide 20 seconds warning for a train travelling at a line speed of 80 mph (129 km/h or 36 metres per second). However, this is only valid for conditions in which there is a single lookout looking in one direction, and the whole group can reach a position of safety in five seconds. If a distant lookout is appointed, and the site lookout has to look in both directions, the required warning time rises to 30 seconds. At the site of the incident, the line speed meant that 30 seconds corresponded to a sighting distance of 1100 metres. The curvature meant that this could not be obtained without the use of an intermediate lookout. An intermediate lookout is used in situations where, because of track curvature or other obstructions, the distant lookout cannot see the site lookout. The intermediate lookout relays the warnings given by the distant lookout, using a flag. The additional time required to transmit the warning through an intermediate lookout adds a further five seconds to the required warning time and would have raised the required sighting distance to 1300 metres. The group did not have enough people to resource an intermediate lookout, and there is no evidence that the COSS considered using one.

Figure 2: a) 11:32:54 Distant lookout in the Up cess, work group on the Down line b) 11:32:56 Workers in the four-foot c) 11:32:58 Workers moving to the cess d) 11:33:01 Track workers in a place of safety (CCTV images courtesy of Greater Anglia.)
Following the incident, the COSS revised the protection arrangements, repositioned the lookouts and instructed the distant lookout to use a flag to give warning. However, he could not have achieved the required sighting distance because there were not sufficient people in the group to provide both distant and intermediate lookouts.
4. Observations
The SSOW packs described the nature of the work as ‘E01 Patrol No 16’ although the team were actually performing height & stagger measurements. This work differed from patrolling in that it required the use of surveying equipment, which was likely to require more time to remove clear of the track. The circumstances of the incident have identified safety lessons as to whether the nature of undertaking height and stagger measurements is consistent with the use of a system of work intended for patrolling. The RAIB also found that there was no evidence of SSOW packs at this depot being audited within the previous twelve months, as required by the Network Rail standard NR/L2/OHS/019.
5. Previous similar occurrences
Other accidents with similarities to the near miss at Great Chesterford also include:
- Roydon 16 July 2012 (RAIB report 07/2013). Two track workers had to run from a bridge in order to avoid being struck by a train. The track workers were clear of the railway line around two seconds before the train passed them. At the time of the incident, the track workers were working on a line which was open to railway traffic, being protected by a system of work which relied on a lookout providing a warning of approaching trains. The incident occurred because the lookout was not able to give the track workers sufficient early warning of the approach of train, because the controller of site safety (COSS) had implemented a system of work which was inappropriate for the planned work and the location in which it was being undertaken. Following its investigation, the RAIB recommended that Network Rail should review and improve the methods which are used by a COSS to assess both the required and available sighting distances. The Office of Rail and Road (ORR) has reported to RAIB that Network Rail has produced training material for track workers which clearly describes methods by which sighting distances can be measured, and the scope of this training has been widened to encourage lookouts to challenge sighting decisions made by a COSS. Based on this information, the ORR has concluded that Network Rail has implemented this recommendation.
As a result of continuing concern about the number of accidents and near miss incidents involving track workers, the RAIB undertook a class investigation into the safety of track workers outside possessions and published a report (RAIB report 07/2017).
Analysis of incidents in this report identified several common causal factors, and the findings from the investigation highlighted similarities to the near miss at Great Chesterford in the following areas:
-
correct planning and the use of safe systems of work that are specific to the location of the work
-
maintenance of site discipline and vigilance, particularly for experienced staff carrying out routine work
-
improvements in procedures and/or training for those in leadership roles to be able to adapt to changes in circumstances (which is particularly relevant to sites of work which move along the track)
-
improvements to the training of track workers in non-technical skills
-
changes in the competence requirements for people who lead track work in higher-risk situations.
Network Rail is currently considering its response to the recommendations made in each of these areas.
You can print this safety digest.