Spotlight on sexually transmitted infections in Yorkshire and Humber: 2021 data
Updated 13 January 2026
Applies to England

© Crown copyright 2026
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/sexually-transmitted-infections-yorkshire-and-humber-data/spotlight-on-sexually-transmitted-infections-in-yorkshire-and-humber-2021-data
Summary
Sexually transmitted infections (STIs) represent an important public health problem in Yorkshire and Humber. Out of the 9 UK Health Security Agency (UKHSA)’s regions, it has the third highest rate of new STIs in England.
In 2021, 25,805 new STIs were diagnosed in Yorkshire and Humber residents, representing a rate of 467 diagnoses per 100,000 population. Rates by upper tier local authority ranged from 242 new STI diagnoses per 100,000 population in East Riding of Yorkshire to 732 new STI diagnoses per 100,000 population in Leeds.
The number of new STIs diagnosed in Yorkshire and Humber residents increased by 5% between 2020 and 2021. Rises were seen in the numbers of most of the 5 major STIs compared to 2020, that is:
- syphilis (29%)
- gonorrhoea (16%)
- genital warts (6%)
- chlamydia (3%)
Genital herpes decreased by 3%.
In June 2021, the National Chlamydia Screening Programme (NCSP) changed to focus on reducing reproductive harm of untreated infection in young women. This led to a change in the recommended chlamydia detection rate indicator (DRI) included in the Public Health Outcomes Framework (PHOF). UKHSA recommends that local authorities work towards the revised female-only PHOF benchmark DRI of 3,250 per 100,000 females aged 15 to 24 years. This report relates to 2021 data, for the most part of which the NCSP recommended an offer of screening to all sexually active young people under 25 years.
In 2021, the chlamydia diagnosis rate among Yorkshire and Humber residents aged 15 to 24 years (all recorded genders) was 1,464 per 100,000 residents, against the previous recommended DRI of least 2,300 per 100,000 residents aged 15 to 24 years (all recorded genders).
Where gender and sexual orientation are known, gay, bisexual, and other men who have sex with men (GBMSM) account for 15% of Yorkshire and Humber residents diagnosed with a new STI excluding chlamydia diagnoses reported via the Chlamydia Testing Activity Dataset (CTAD) surveillance system (73% of which were diagnosed with syphilis and 32% diagnosed with gonorrhoea).
STIs disproportionately affect young people. Yorkshire and Humber residents aged between 15 and 24 years accounted for 54% of all new STI diagnoses in 2021. A steep decline (93% decrease) has been seen between 2017 and 2021 in genital warts diagnosis rates in females aged 15 to 19 years. This follows the introduction in 2008 of vaccination against human papillomavirus (HPV), the virus which causes genital warts, for females aged 12 to 13 years.
The white ethnic group has the highest number of new STI diagnoses (16,951, 84%). Although only 2% of new STIs are among the black Caribbean ethnic group, this group has the highest rate (1,371 per 100,000), which is 4 times the rate seen in the white ethnic group. Where country of birth was known, 88% of Yorkshire and Humber residents diagnosed with a new STI in 2021 (excluding chlamydia diagnoses reported via CTAD) were UK-born.
Conclusions
Following the disruptions in service delivery during the first year of the coronavirus (COVID-19) pandemic, the number of consultations at sexual health services (SHSs) increased between 2020 and 2021 and now exceeds the number reported in 2019. In Yorkshire and Humber, the number of consultations for 2021 approached the level of consultations observed in 2019 (294,000 compared to 299,000 respectively). This provides evidence of a recovery in service provision, after the lifting of COVID-19 restrictions in the summer of 2021, partially driven by the continued widespread provision of online consultations.
The number of sexual health screens (for chlamydia, gonorrhoea, syphilis and HIV) in England also increased between 2020 and 2021. This increase may be a result of a built-up demand for screening, a return to pre-COVID-19 pandemic levels of social and sexual mixing, and the substantial number of tests being accessed through online services (1 to 4). It will remain important to continue to monitor and understand whether these changes have affected equity of access to SHS and impacted on detection rates for STIs (5, 6).
Overall, Yorkshire and Humber has the third highest rate of STIs in England and has the second highest rate outside of London. In 2021, whilst there was a drop in total STI diagnoses, this was predominantly driven by a fall in chlamydia (decreasing from 22,000 diagnoses in 2017 to 15,000 in 2021). However, during this period chlamydia diagnoses have increased in GBMSM (increasing from 729 diagnoses in 2017 to 766 diagnoses in 2021). This may reflect a lack of testing in other groups or could reflect an increase in the number of tests among GBMSM. This change in pattern of STI diagnoses could also be due to the impact of service disruption as a result of the COVID-19 pandemic.
STI testing rates have recovered in 2021 to comparable levels pre-COVID-19 pandemic, whereas test positivity has not increased in 2021 compared to 2020 (7). STI consultations have also not yet recovered to pre-COVID-19 pandemic levels but have increased from those in 2020.
In Yorkshire and Humber, diagnosis rates of gonorrhoea have increased between 2017 and 2021 whereas the remaining 4 STIs have either decreased or remained fairly stable. It is important that we continue to monitor these infections and the groups affected. Females aged between 20 and 24 years have the highest rate of new STIs per 100,000 in Yorkshire and Humber and it may be appropriate to consider local health promotion messaging for this group. Diagnoses of gonorrhoea and chlamydia have increased in GBMSM between 2017 and 2021 in Yorkshire and Humber, reflecting national trends.
There is considerable variation within the Yorkshire and Humber region for new STI diagnoses. Whilst the regional rate of new STI diagnoses is 467 per 100,000 population, compared to 551 per 100,000 population across England, Leeds and Kingston upon Hull reported substantially higher rates (732 and 684, respectively). This may reflect the impact of population distribution and other social risk factors and may be influenced by small area deprivation. Further analysis may be useful for investigating the impact of population-level factors on rates of new STIs in Yorkshire and Humber.
UKHSA’s main messages
Providers and commissioners have an important role in communicating messages about safer sexual behaviours and how to access services.
Important prevention messages
Using condoms consistently and correctly protects against HIV and other STIs such as chlamydia, gonorrhoea, and syphilis, and can prevent unplanned pregnancy.
Regular screening for STIs and HIV is essential to maintain good sexual health – everyone should have an STI screen, including an HIV test, on at least an annual basis if having condomless sex with new or casual partners.
In addition:
- women and other people with a womb or ovaries aged under 25 years who are sexually active should have a chlamydia test annually and on change of sexual partner
- GBMSM should have an annual test for HIV and STIs or every 3 months if having condomless sex with new or casual partners
HIV pre-exposure prophylaxis (PrEP) can also be used to provide protection to people at risk of HIV while HIV post-exposure prophylaxis (PEP) can be used after condomless sex if someone has potentially been exposed to HIV, to reduce the risk of contracting HIV; both can be obtained from specialist SHSs.
People living with diagnosed HIV who are on treatment and have an undetectable viral load are unable to pass on the infection to others during sex; this is known as ‘Undetectable = Untransmittable’ or ‘U=U’.
Vaccination against mpox (monkeypox) virus, HPV, hepatitis A and hepatitis B will protect against disease caused by these viruses and prevent the spread of these infections:
- GBMSM can obtain the mpox, hepatitis A and hepatitis B vaccines from specialist SHSs – these vaccines are also available for other people at high risk of exposure to the viruses
- GBMSM aged 45 years and under, can also obtain the HPV vaccine from specialist SHSs
SHSs are free and confidential and offer testing and treatment for HIV and STIs, condoms, vaccination, HIV PrEP, and PEP:
- online self-sampling for HIV and STIs is widely available
- information and advice about sexual health including how to access services is available at Sexwise and from the national sexual health helpline on 0300 123 7123
Charts, tables and maps
Figure 1. New STI diagnosis rates by UKHSA region of residence, England, 2021

Data sources: GUMCAD (previously known as Genitourinary Medicine Clinic Activity Dataset) STI surveillance system, CTAD
Figure 1 is a bar chart showing that London reported the highest rate of new STI diagnosis per 100,000 population in 2021, with the North West and Yorkshire and Humber reporting the second and third highest rate (481.0 and 466.9, respectively; Figure 1).
Figure 2. Number of diagnoses of the 5 main STIs, Yorkshire and Humber residents, 2017 to 2021

Data sources: GUMCAD, CTAD
[note 1] Any increase in gonorrhoea diagnoses may be due to the increased use of highly sensitive nucleic acid amplification tests (NAATs) and additional screening of extra-genital sites in GBMSM. Any decrease in genital wart diagnoses may be due to a moderately protective effect of HPV-16/18 vaccination. Any increase in genital herpes diagnoses may be due to the use of more sensitive NAATs. Increases or decreases may also reflect changes in testing practices.
Figure 2 shows trend lines for the number of diagnoses of the 5 main STIs among Yorkshire and Humber residents. Of the 5 STIs presented, the number of diagnoses of chlamydia have most notably declined over the 5-year period between 2017 and 2021 (decreasing from 21,773 to 15,323). The number of diagnoses of genital warts, genital herpes and syphilis have also declined over this period (Figure 2). Gonorrhoea diagnoses have increased during this time (increasing from 2,871 to 3,409).
Figure 3. Diagnosis rates of the 5 main STIs, Yorkshire and Humber residents, 2017 to 2021

Data sources: GUMCAD, CTAD
See [note 1] above.
Figure 3 shows trend lines for diagnosis rates of the 5 main STIs among Yorkshire and Humber residents. Of the 5 STIs presented, the diagnoses rate of chlamydia has most notably declined over the 5-year period (decreasing from 399.5 to 277.3). The diagnoses rate of genital warts, genital herpes and syphilis have also declined over this period (Figure 2). Gonorrhoea diagnoses have increased during this time (increasing from 52.7 to 61.7).
Table 1. Percentage change in new STI diagnoses, Yorkshire and Humber residents
| Diagnoses | 2021 | Percentage change from 2017 to 2021 | Percentage change from 2020 to 2021 |
| New STIs | 25,805 | -31% | 5% |
| Syphilis | 323 | -21% | 29% |
| Gonorrhoea | 3,409 | 19% | 16% |
| Chlamydia | 15,323 | -30% | 3% |
| Genital Herpes | 1,797 | -28% | -3% |
| Genital Warts | 2,211 | -55% | 6% |
Data sources: GUMCAD, CTAD
See [note 1] above.
Table 1 shows that, between 2020 and 2021, new STI diagnoses increased by 5%. Syphilis diagnoses reported the largest percentage change increase, followed by gonorrhoea (increasing by 29% and 16%, respectively; Table 1). Between 2017 and 2021 the diagnoses of new STIs notably decreased (decreasing by 31%; Table 1) with a notable exception of this trend being observed with gonorrhoea diagnoses, which increased by 19% between 2017 and 2021 (Table 1). However, it is important to remember the significant disruption caused by the COVID-19 pandemic on SHSs and individual’s behaviour.
Figure 4. Rates of new STIs per 100,000 residents by age group (for those aged 15 to 64 years only) and gender in Yorkshire and Humber, 2021

Data sources: GUMCAD, CTAD
Figure 4 is a bar chart that shows rates of new STIs in Yorkshire and Humber in 2021 were highest in those aged 24 years and under. Females aged between 20 to 24 years reported the highest rate of new STIs per 100,000 .
Figure 5. Rates of gonorrhoea per 100,000 residents by age group [note 2] in Yorkshire and Humber, 2017 to 2021

Data source: GUMCAD
[note 2] Age-specific rates are shown for those aged 15 to 64 years only.
Figure 5 shows trend lines for the rates of gonorrhoea by age group (for those aged 15 to 64 years only) that have either increased overtime or remained constant between 2017 and 2021. Rates have increased most notably in those aged 35 to 44 years and those aged 25 to 34 years.
Figure 6. Rates of genital warts per 100,000 residents aged 15 to 19 years by gender in Yorkshire and Humber, 2017 to 2021

Data source: GUMCAD
Figure 6 shows trend lines of the rates of genital warts, which have substantially decreased among both females and males aged between 15 to 19 years from 2017 and 2021.
Figure 7. Rates of new STIs by ethnic group per 100,000 residents in Yorkshire and Humber, 2021

Data sources: GUMCAD, CTAD
Figure 7 is a bar chart showing that rates of new STIs are highest among the black Caribbean ethnic group and the black African ethnic group. They are lowest among the white ethnic group.
Table 2. Proportion of Yorkshire and Humber residents diagnosed with a new STI by ethnicity, 2021
| Ethnic group | Number | Percentage excluding unknown |
|---|---|---|
| White | 16,951 | 84% |
| Black Caribbean | 321 | 2% |
| Black African | 515 | 3% |
| All other ethnic groups combined | 2,413 | 12% |
| Unknown | 5,605 |
Data sources: GUMCAD, CTAD
Table 2 shows that, of the 20,200 new STI diagnoses where ethnic group was provided, the majority were from the white ethnic group, followed by the black African ethnic group and then the black Caribbean ethnic group. Ethnicity information was not available for 5,605 residents, highlighting the need to improve collection of ethnicity data.
Figure 8. Proportion of Yorkshire and Humber residents diagnosed with a new STI by world region of birth [note 3], 2021

Data source: GUMCAD
[note 3] Data on country of birth is not collected by CTAD. All information about world region of birth is based on diagnoses made in specialist and non-specialist services, which report to GUMCAD.
Figure 8 is a bar chart showing the majority (88%) of those diagnosed with a new STI in 2021 were born in the UK.
Figure 9. Diagnoses of the 5 main STIs among GBMSM [note 4], Yorkshire and Humber residents, 2017 to 2021
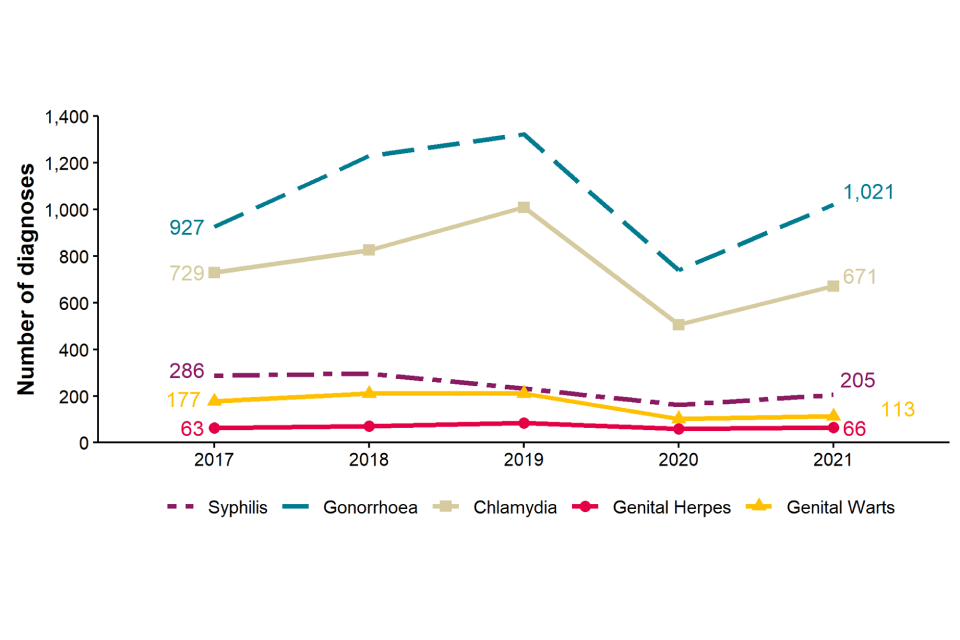
Data source: GUMCAD
[note 4] Data on sexual orientation is not collected by CTAD. All information about GBMSM is based on diagnoses made in specialist and non-specialist services which report to GUMCAD.
Figure 9 is a line chart that show diagnoses of gonorrhoea increased in GBMSM between 2017 and 2021, whereas diagnoses of chlamydia, syphilis, genital warts and genital herpes remained fairly consistent.
Table 3. Percentage change in new STI diagnoses in GBMSM residents in Yorkshire and Humber
| Diagnoses | 2021 | Percentage change from 2017 to 2021 | Percentage change from 2020 to 2021 | ||
|---|---|---|---|---|---|
| New STIs | 2,273 | -11% | 27% | ||
| Syphilis | 205 | -28% | 26% | ||
| Gonorrhoea | 1,021 | 10% | 38% | ||
| Chlamydia | 766 | 5% | 26% | ||
| Genital herpes | 66 | 5% | 10% | ||
| Genital warts | 113 | -36% | 11% |
Data sources: GUMCAD
See [note 4] above.
Table 3 shows the total number of new STIs has decreased by 11% between 2017 and 2021. The number of new diagnoses of gonorrhoea, chlamydia and genital herpes have increased between 2017 and 2021 compared to number of new diagnoses of genital warts and syphilis, which have decreased over this time.
Compared to 2020, all STIs included in Table 3 increased in 2021. However, when comparing 2020 and 2021, it is important to remember the disruption caused by the COVID-19 pandemic on sexual health services and individual’s behaviour.
Figure 10a. Rate of new STI diagnoses per 100,000 population among Yorkshire and Humber residents by upper tier local authority of residence, 2021

Data sources: GUMCAD, CTAD
Figure 10a is a bar chart showing the regional rate of new STI diagnoses for Yorkshire and Humber is 467 per 100,000 population, compared to 551 per 100,000 population across England. Leeds and Kingston upon Hull reported rates higher than the region and England (732 and 684, respectively).
Figure 10b. Rate of new STI diagnoses (excluding chlamydia diagnoses in people aged 15 to 24 years) per 100,000 population aged 15 to 64 years among Yorkshire and Humber residents by upper tier local authority of residence, 2021
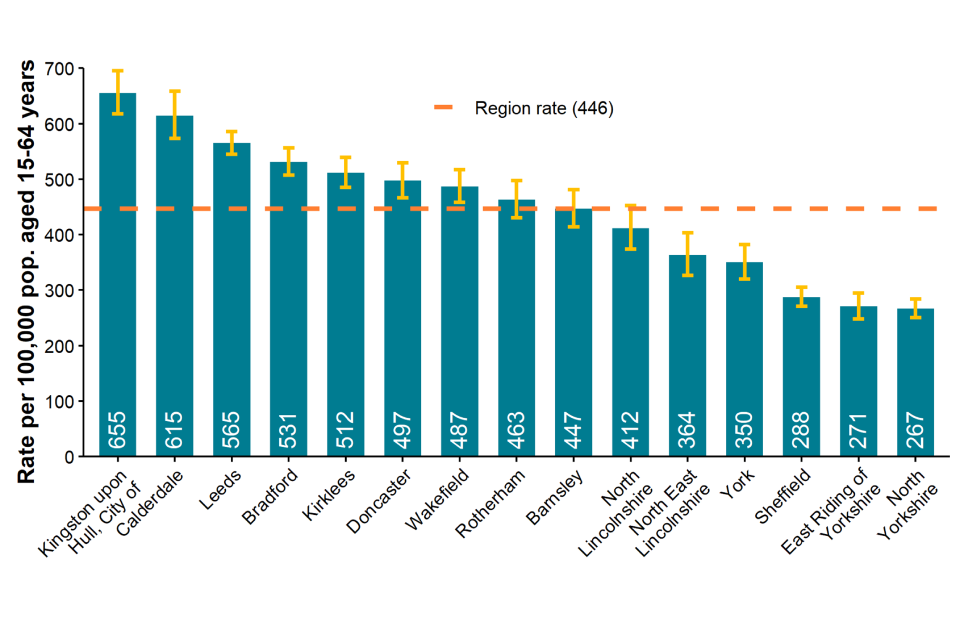
Data sources: GUMCAD, CTAD
Figure 10b is a bar chart showing Kingston upon Hull reported the highest rate of new STI diagnoses, excluding chlamydia diagnoses in people aged 15 to 24 years, followed by Calderdale and Leeds (655, 615 and 565, respectively).
Figure 11. Chlamydia detection rate per 100,000 population aged 15 to 24 years in Yorkshire and Humber residents by upper tier local authority of residence, 2021

Data sources: GUMCAD, CTAD
Figure 11 is a bar chart showing North East Lincolnshire reported the highest rate of chlamydia among those aged 15 to 24 years in 2021, followed by Leeds and Kingston upon Hull (2,631, 2,214 and 1,871, respectively).
Figure 12. Rate of gonorrhoea diagnoses per 100,000 population in Yorkshire and Humber residents by upper tier local authority of residence, 2021
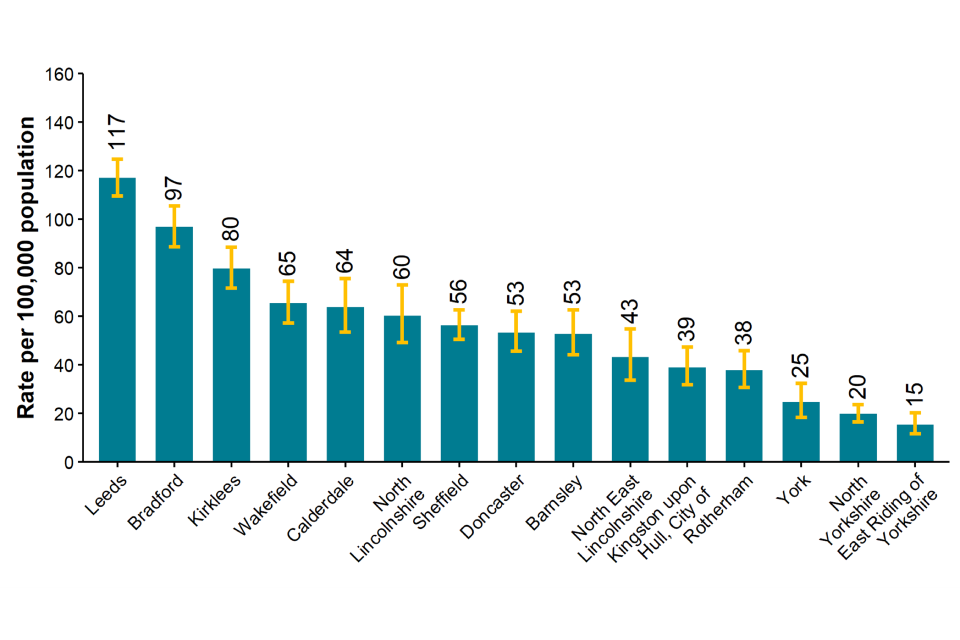
Data source: GUMCAD
Figure 12 is a bar chart showing Leeds reported the highest rate of gonorrhoea diagnoses followed by Bradford and Kirklees (117, 97, 80, respectively).
Figure 13. Map of new STI rates per 100,000 residents by upper tier local authority in Yorkshire and Humber, 2021

Data sources: GUMCAD, CTAD. Map contains Ordnance Survey data (© Crown copyright and database right 2021) and National Statistics data (© Crown copyright and database right 2021)
Figure 13 is a map showing that Leeds, followed by Kingston upon Hull and Calderdale, reported the highest rates of new STI diagnoses in Yorkshire and Humber in 2021 (732.1, 683.8 and 515.0 respectively).
Figure 14. STI testing rate (excluding chlamydia in under 25 year olds) per 100,000 population in Yorkshire and Humber residents aged 15 to 64 years, 2017 to 2021
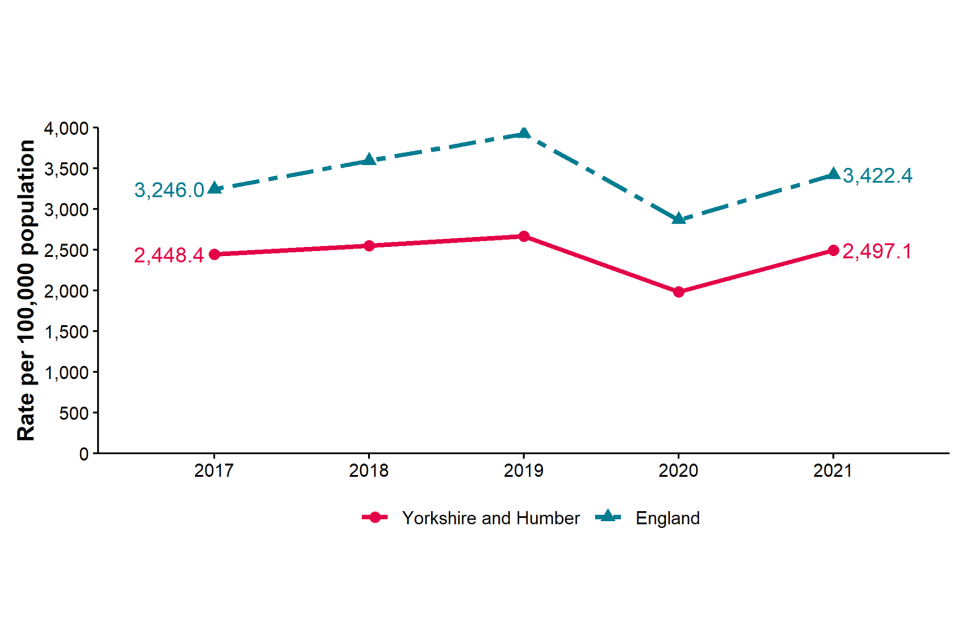
Data sources: GUMCAD, CTAD
Figure 14 shows trend lines for the STI testing rate (excluding chlamydia in people aged under 25 years) which remained fairly constant over the 5-year period between 2017 and 2021. Yorkshire and Humber has consistently reported a lower rate compared to that observed across all of England. Both Yorkshire and Humber and England demonstrated a recovery in testing rate in 2021 following the decline in 2020.
Figure 15. STI testing positivity rate [note 5] (excluding chlamydia in people aged under 25 years) in Yorkshire and Humber residents, 2017 to 2021
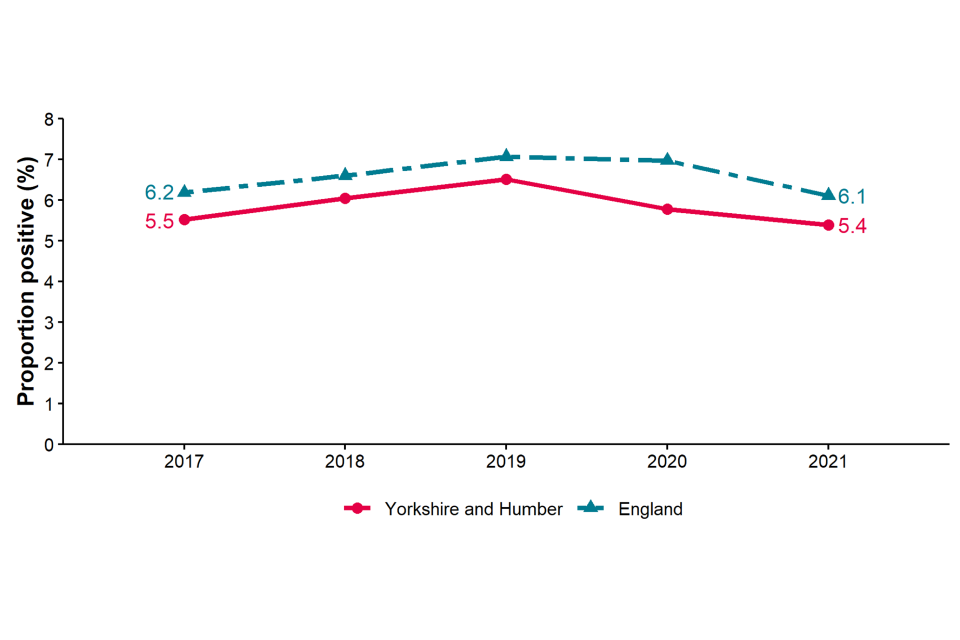
Data sources: GUMCAD, CTAD
[note 5] The numerator for the STI testing positivity rate now only includes infections which are also included in the denominator. These are: chlamydia (excluding diagnoses in those aged under 25 years), gonorrhoea, syphilis, and HIV. Up to 2018 (data for 2017) it included all new STIs.
Figure 15 shows trend lines for the STI testing positivity rate (excluding chlamydia in people aged under 25 years), which has remained fairly stable between 2017 and 2021 in Yorkshire and Humber. England’s rate appears to have gone through a marginal increase and then marginal decrease over the same period and has consistently been equal to or higher than the rate reported in Yorkshire and Humber.
Table 4. Number of diagnoses of new STIs by UKHSA region of residence, data source and data subset 2021
| UKHSA region of residence | GUMCAD specialist SHSs | GUMCAD non-specialist SHSs [note 6] | CTAD [note 7] | Total |
|---|---|---|---|---|
| East Midlands | 10,622 | 6,275 | 3,974 | 20,871 |
| East of England | 15,809 | 4,238 | 5,608 | 25,655 |
| London | 69,545 | 8,162 | 23,792 | 101,499 |
| North East | 7,495 | 1,580 | 2,718 | 11,793 |
| North West | 23,693 | 3,789 | 7,954 | 35,436 |
| South East | 26,578 | 1,960 | 8,287 | 36,825 |
| South West | 13,797 | 2,444 | 4,782 | 21,023 |
| West Midlands | 16,890 | 3,867 | 4,804 | 25,561 |
| Yorkshire and Humber | 16,031 | 2,050 | 7,724 | 25,805 |
Data sources: GUMCAD, CTAD
[note 6] Diagnoses from enhanced GPs reporting to GUMCAD are included in the ‘Non-specialist sexual health services (SHSs)’ total.
[note 7] Including site type 12 chlamydia from GUMCAD.
Table 4 shows that London reported the largest number of new STI diagnoses (101,499 in total) followed by the South East and North West (36,825 and 35,436, respectively).
Table 5. Number of diagnoses of the 5 main STIs in Yorkshire and Humber by STI, data source and data subset 2021
| 5 main STIs | GUMCAD specialist SHSs | GUMCAD non-specialist SHSs [note 8] | CTAD [note 9] | Total |
|---|---|---|---|---|
| Syphilis | 323 | 323 | ||
| Gonorrhoea | 2,535 | 874 | 3,409 | |
| Chlamydia | 6,455 | 1,144 | 7,724 | 15,323 |
| Genital herpes | 1,792 | 5 | 1,797 | |
| Genital warts | 2,192 | 19 | 2,211 |
Data sources: GUMCAD, CTAD
Table 5 shows that all syphilis diagnoses were identified from specialist SHSs as were the majority of all other STIs. Chlamydia and gonorrhoea diagnoses were the most common STI diagnosis made in non-specialist SHSs.
Figure 16. Consultations by consultation type: Yorkshire and Humber residents, 2017 to 2021
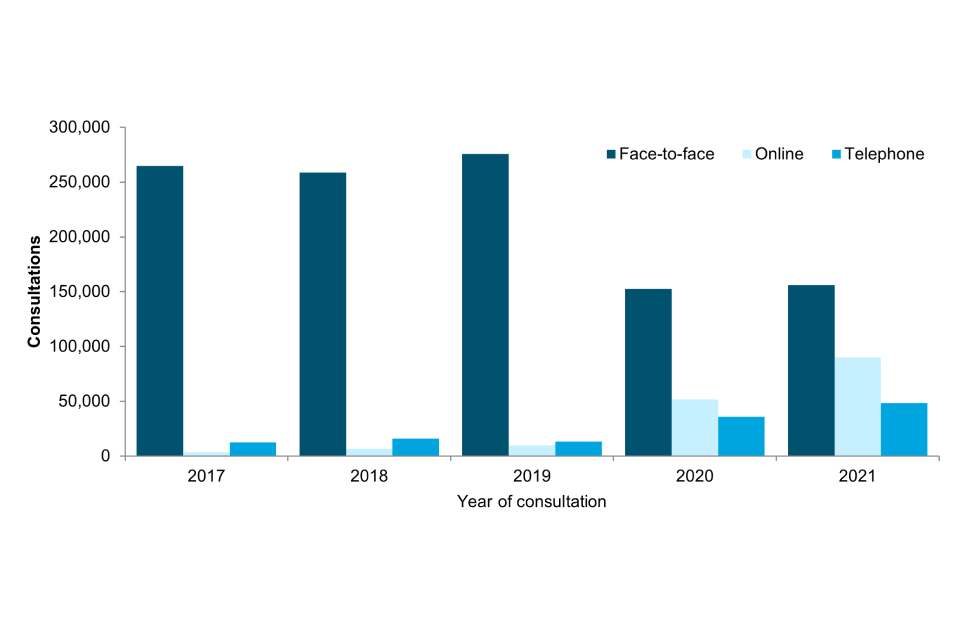
Data sources: GUMCAD, CTAD
Figure 16 is a bar graph showing the number of consultations in Yorkshire and Humber residents attending SHSs (including both specialist and non-specialist services) over the 5-year period: 2017 to 2021 by the type of consultation. It shows that the predominant type of consultation pre pandemic was face-to-face, whereas during and since the pandemic there has been an increase in online and telephone consultations. In 2021, face-to-face consultations were the majority (accounting for 53% of consultations), however, the trend of higher volumes of online and telephone consultations was still observed (Table 6).
Table 6. Consultations by consultation type: Yorkshire and Humber residents, 2017 to 2021
| Consultation type | 2017 | 2018 | 2019 | 2020 | 2021 |
|---|---|---|---|---|---|
| Face-to-face | 264,678 | 258,740 | 275,532 | 15,2544 | 156,086 |
| Online | 3,683 | 6,550 | 9,995 | 51,566 | 89,975 |
| Telephone | 12,461 | 15,971 | 13,476 | 36,013 | 48,202 |
| Total | 280,822 | 281,261 | 299,003 | 240,123 | 294,263 |
Data sources: GUMCAD, CTAD
Information on data sources
Find more information on local sexual health data sources on GOV.UK.
These figures are based on data from the GUMCAD and CTAD surveillance systems published on 4 October 2022 (data to the end of calendar year 2021).
GUMCAD surveillance system
This disaggregates reporting system collects information about attendances and diagnoses at specialist (level 3) and non-specialist (level 2) sexual health services. Information about the patient’s area of residence is collected along with demographic data and other variables. GUMCAD superseded the earlier KC60 system and can provide data from 2009 onwards. GUMCAD is the main source of data for this report.
Due to limits on how much personally identifiable information sexual health clinics are able to share, it is not possible to deduplicate between different clinics. There is a possibility that some patients may be counted more than once if they are diagnosed with the same infection (for infection specific analyses) or a new STI of any type (for new STI analyses) at different clinics during the same calendar year.
CTAD surveillance system
CTAD collects data on all NHS and local authority, or NHS-commissioned chlamydia testing carried out in England. CTAD is comprised of all chlamydia (NAATs) tests for all ages (with the exception of conjunctival samples), from all venues and for all reasons. CTAD enables unified, comprehensive reporting of all chlamydia data, to effectively monitor the impact of the NCSP through estimation of the coverage of population screening, proportion of all tests that are positive and detection rates.
For services which report to GUMCAD and for which CTAD does not receive data on the patient’s area of residence (for example SHSs), information about chlamydia diagnoses is sourced from GUMCAD data.
New STIs
New STI diagnoses comprise diagnoses of the following:
- chancroid
- Lymphogranuloma venereum (LGV)
- donovanosis
- chlamydia
- gonorrhoea
- genital herpes (first episode)
- HIV (acute and AIDS defining)
- Molluscum contagiosum
- non-specific genital infection (NSGI)
- non-specific pelvic inflammatory disease (PID) and epididymitis
- chlamydial PID and epididymitis (presented in chlamydia total)
- gonococcal PID and epididymitis (presented in gonorrhoea total)
- scabies
- pediculosis pubis
- syphilis (primary, secondary and early latent)
- trichomoniasis and genital warts (first episode)
- Mycoplasma genitalium
- shigella
Calculations
Confidence Intervals were calculated using Byar’s method.
Office for National Statistic (ONS) mid-year population estimates for 2020 were used as a denominator for rates for 2021. ONS ceased producing estimates of population by ethnicity in 2011. Estimates for that year were used as a denominator for rates for 2021.
Further information
As of 2020, all analyses for this report include data from non-specialist (level 2) SHSs and enhanced GP services as well as specialist (level 3) SHSs.
For further information, access the online Sexual and Reproductive Health Profiles.
Find more information on local sexual health data sources on GOV.UK.
Local authorities have access to the Summary Profile of Local Authority Sexual Health (SPLASH) Reports (accessible from the Sexual and Reproductive Health Profiles) and the SPLASH supplement reports via the HIV and STI Data exchange.
For an Annual Epidemiological Spotlight on HIV in Yorkshire and Humber, contact yhfs@ukhsa.gov.uk
About the Field Service
The Field Service was established in 2018 as a national service comprising geographically dispersed multi-disciplinary teams integrating expertise in Field Epidemiology, Real-time Syndromic Surveillance, Public Health Microbiology and Food, Water and Environmental Microbiology to strengthen the surveillance, intelligence and response functions of UKHSA.
You can contact your local Field Service team at yhfs@ukhsa.gov.uk
If you have any comments or feedback regarding this report or the Field Service, contact josh.forde@ukhsa.gov.uk
Acknowledgements
We would like to thank:
- local SHSs for supplying the SHS data
- local laboratories for supplying the CTAD data
- UKHSA Blood Safety, Hepatitis, Sexually Transmitted Infections (STI) and HIV Division for collection, analysis and distribution of data
References
1. Mitchell KR, Shimonovich M, Bosó Pérez R, Dema E, Clifton S, Riddell J and others. Initial Impacts of COVID-19 on sex life and relationship quality in steady relationships in Britain: Findings from a large, quasi-representative Survey (Natsal-COVID) Journal of Sex Research March 2022: pages 1 to 12 (viewed on 11 August 2022)
2. Howarth A, Saunders J, Reid D, Kelly I, Wayal S, Weatherburn P, Hughes G and Mercer C. Stay at home ….: Exploring the impact of the COVID-19 public health response on sexual behaviour and health service use among men who have sex with men: findings from a large online survey in the United Kingdom Sexually Transmitted Infections July 2022, pages 346 to 352 (viewed on 11 August 2022)
3. Dema E, Gibbs J, Clifton S and others. Initial impacts of COVID-19 on sexual and reproductive health service use and unmet need in Britain: findings from a large, quasirepresentative survey (Natsal-COVID) Lancet Public Health 2022: volume 7, pages e36 to 47
4. Sonnenberg P, Menezes D, Freeman L and others. Intimate physical contact between people from different households during the COVID-19 pandemic: a mixed-methods study from a large, quasi-representative survey (Natsal-Covid) British Medical Journal Open 2022: volume 12, issue 2 (viewed on 11 August 2022)
5. Ratna N, Dema E, Conolly A and others. O16 Ethnic variations in sexual risk behaviour, sexual health service use and unmet need during the first year of the COVID-19 pandemic: an analysis of population-based survey and surveillance data Sexually Transmitted Infections 2022: volume 98, pages A8 to A9 (viewed on 11 August 2022)
6. Sumray K, Lloyd KC, Estcourt CS, Burns F and Gibbs J. Access to, usage and clinical outcomes of, online postal sexually transmitted infection services: a scoping review Sexually Transmitted Infections June 2022: pages 1 to 8 (viewed on 11 August 2022)
7. UKHSA Official Statistics Sexually transmitted infections and screening for chlamydia in England: 2021 report