Travel-associated infections in England, Wales and Northern Ireland: 2020 and 2021
Updated 14 August 2025
Applies to England, Northern Ireland and Wales

© Crown copyright 2025
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/travel-associated-infections/travel-associated-infections-in-england-wales-and-northern-ireland-2020-and-2021
Background
This report, produced by the Travel Health and International Health Regulations (IHR) team in the Clinical and Emerging Infections Directorate, UK Health Security Agency (UKHSA), summarises case numbers of selected travel-associated infections reported in England, Wales and Northern Ireland between 2015 and 2021. Case numbers were previously reported through ECDC between 2015 and 2019 for chikungunya, cholera (Vibrio cholerae serogroup O1 or O139), dengue, yellow fever and Zika.
Additional more detailed information is included in this report on the trends of chikungunya, cholera, dengue, yellow fever and Zika in 2020 and 2021.
Detailed annual reports are available for imported malaria cases in the UK and travel-associated enteric fever cases in EWNI.
The data presented in this report supersedes data in any other reported case numbers due to de-duplication.
Data sources
Data for cases of chikungunya, dengue, yellow fever and Zika was obtained from the Rare and Imported Pathogens Laboratory (RIPL), UKHSA Porton. Case definitions used for these infections are as follows:
- confirmed: molecular detection (PCR, other molecular amplification test or sequencing) and/or positive virus isolation and/or seroconversion between acute and convalescent samples and/or four-fold rise in antibody titre
- probable: IgM and IgG positive and compatible clinical syndrome
Data for confirmed cholera cases was obtained from the Gastrointestinal Bacteria Reference Unit (GBRU), UKHSA Colindale. A confirmed case is a person with Vibrio cholerae serogroup O1 or O139 confirmed by the UKHSA Gastrointestinal Bacteria Reference Unit.
Changes in travel to and from the UK in 2020 and 2021
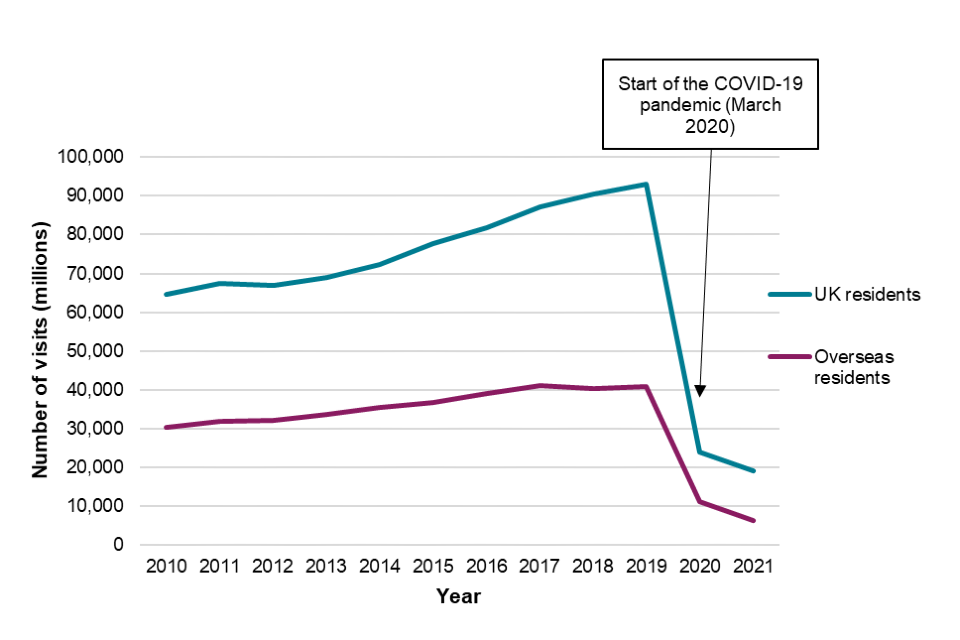
Since the beginning of the COVID-19 pandemic in 2020 there has been a significant decrease in worldwide travel as many countries, including the UK, imposed restrictions on arriving and departing travellers [1]. In line with falling numbers of travellers arriving in the UK, the number of travel-associated infections diagnosed in the UK also decreased.
Data on travel to and from the UK was obtained from the Office of National Statistics International Passenger Survey. In 2020, UK residents made 23.8 million visits abroad, which was a 74% decrease from 2019, and there were 11.1 million visits made by overseas residents to the UK, a 73% decrease compared to 2019 [2].
Between April and June 2021, UK residents made 1 million visits abroad by air and overseas residents made 277,000 visits to the UK [3]. Between July and September 2021, UK residents made 6.1 million visits abroad by air, with most visits being made to European destinations (5.4 million), and overseas residents made 1.3 million visits to the UK. These were a 76% and 86% decrease respectively compared to the same quarter in 2019 [4]. Overall, in 2021 UK residents made 19.1 million visits abroad, which was a 20% decrease from 2020, and there were 6.4 million visits made by overseas residents to the UK, a 43% decrease compared to 2020 (Figure 1). These decreases can be explained by ongoing restrictions to international travel in 2021 [5].
Individual travel destinations for UK travellers from the International Passenger Survey is not available for 2020 due to the suspension of the study during the COVID-19 pandemic [6] and data for April to December 2020 are based on ONS’ administrative sources and modelling.
Figure 1. Visits to and from the UK from 2010 to 2021
Travel-associated infections 2015 to 2021
Table 1. Travel-associated infections in England, Wales and Northern Ireland (EWNI): 2015 to 2021
| Disease (Organism) | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 |
|---|---|---|---|---|---|---|---|
| Chikungunya | 101 | 154 | 92 | 57 | 98 | 36 | 17 |
| Cholera (Vibrio cholerae serogroup O1 or O139) | 15 | 16 | 14 | 17 | 15 | 2 | 1 |
| Dengue | 421 | 464 | 442 | 411 | 787 | 102 | 95 |
| Yellow fever | – | – | – | 1 | – | – | – |
| Zika | 4 | 275 | 21 | 4 | 6 | 1 | 1 |
Case numbers presented in this report include both confirmed and probable cases for chikungunya, dengue and Zika and confirmed cases for cholera and yellow fever.
Chikungunya
Chikungunya is a mosquito-borne infection transmitted by the bite of an infected female Aedes mosquito. It is caused by a virus from the Flaviviridae family. It is characterised by a sudden onset of fever usually accompanied by joint pain (arthralgia); however, symptoms can range from mild or non-existent to severe. Serious complications are not common, but, rarely, in older people the disease can contribute to the cause of death, particularly if there is other underlying illness. Chikungunya mainly occurs in Africa, Asia and specifically in Southern Asia, although there have been cases reported in parts of Europe and North America [7].
Data for cases of chikungunya was obtained from the Rare and Imported Pathogens Laboratory (RIPL), UKHSA Porton.
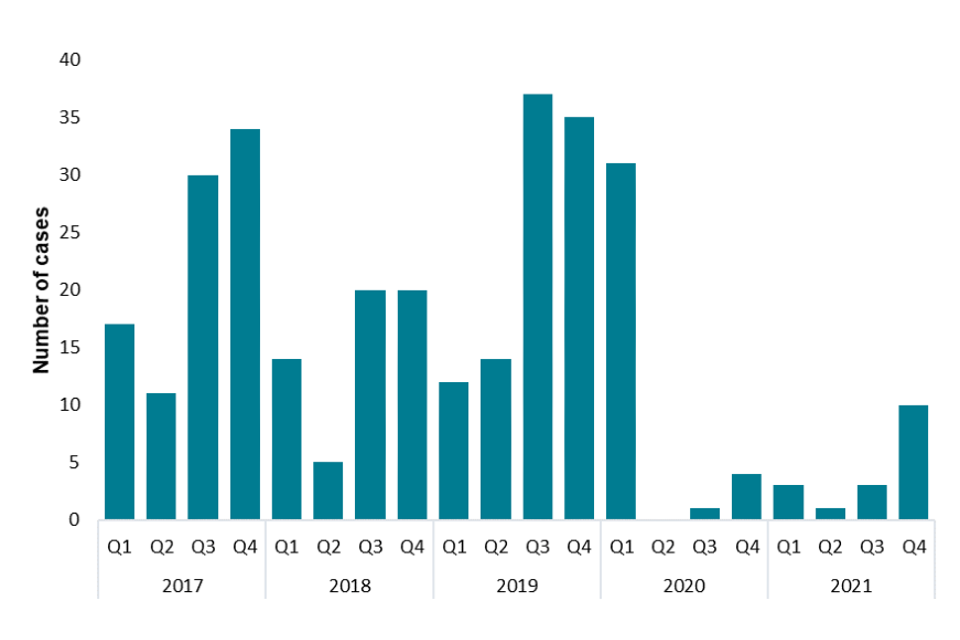
In EWNI, between 2015 and 2019 there were an average of 100 chikungunya cases reported each year, with a peak in 2016 of 154 cases. There were 36 chikungunya cases reported in 2020 (35 in England and 1 in Northern Ireland), which was a 63% decrease compared to 2019. Of these, 8 (22%) were confirmed cases and 28 (72%) were probable cases. There were 17 cases reported in 2021 (16 in England and 1 in Wales), of which 5 (29%) were confirmed cases and 17 (71%) probable cases. The large decrease in cases coincides with the COVID-19 pandemic where international travel greatly reduced, which could explain this change. The majority of cases (n=31) were diagnosed in the first quarter of 2020 and the remaining cases in the third and fourth quarters (Figure 2). Case numbers remained low for the first three quarters in 2021 (n=3, n=1, n=3) and then increased slightly with 10 cases diagnosed in the fourth quarter. This aligns with public health advice to stop travelling at the end of March 2020 due to the COVID-19 pandemic and travel re-opening later in 2020, before the biggest increases in travel occurring later in 2021.
Figure 2. Cases of chikungunya by quarter, Q1 2017 to Q4 2021
In 2020, 22 cases (61%) were female (aged 22 to 85 years, median=52) and 12 (33%) were male (aged 24 to 78, median=48, Table 2). In 2021, 9 cases (53%) were female (aged 7 to 53 years, median=45) and 7 (41%) were male (aged 24 to 83, median=42). There were 2 cases with unknown sex in 2020 and one in 2021.
Table 2. Cases of chikungunya by age group and sex, 2020 and 2021
| Age group | Female (2020) | Male (2020) | Unknown (2020) | Female (2021) | Male (2021) | Unknown (2021) |
|---|---|---|---|---|---|---|
| Under 19 | – | – | – | 1 | – | 1 |
| 20-29 | 3 | 2 | – | – | 1 | – |
| 30-39 | 4 | 2 | – | 1 | 1 | – |
| 40-49 | 3 | 2 | – | 3 | 3 | – |
| 50-59 | 9 | 5 | 1 | 4 | 1 | – |
| 60-69 | 2 | – | 1 | – | 1 | – |
| 70 and over | 1 | 1 | – | – | – | – |
| Total | 22 | 12 | 2 | 9 | 7 | 1 |
In 2020, travel history was known for 34 out of 36 cases, with the majority of these reporting travel to Eastern Africa (14 cases, 41%) and South-Eastern Asia (11 cases, 32%, Table 3). In 2021, travel history was known for 13 out of 17 cases, with cases reporting travel to Western Africa, Southern Asia and Eastern Africa. The most frequently reported country of travel was Somalia in 2020 (13 cases) and Nigeria in 2021 (6 cases). No documented chikungunya outbreaks were reported in Somalia in 2020, however there have been recurring outbreaks in the Somali region of Ethiopia since 2016, including in 2019 [8]. This region borders Somalia and therefore it would be likely that human movement could occur between the borders.
Table 3. Cases of chikungunya by region of travel, 2020 and 2021
| Region of travel | 2020 | 2021 |
|---|---|---|
| Eastern Africa | 14 | 2 |
| South-Eastern Asia | 11 | – |
| Southern Asia | 7 | 5 |
| Western Africa | 1 | 6 |
| Northern Africa | 1 | – |
| Not stated | 2 | 4 |
| Total | 36 | 17 |
Cholera (Vibrio cholerae serogroup O1 or O139)
Cholera is caused by infection of one of two serogroups of the Vibrio cholerae bacteria, serogroups O1 and O139.
Cholera is an acute diarrhoeal disease caused by ingestion of contaminated food or water. Cholera is a vaccine-preventable infection, though vaccination is only recommended for some travellers. Cases may be asymptomatic or have mild symptoms, including acute, profuse watery diarrhoea (‘rice water stools’) and vomiting, leading to dehydration. Some infections may progress to severe disease, and in extreme cases may result in death if untreated [9]. Cholera cases were reported in 27 countries in 2020 and the disease occurs mainly in Africa and Asia, but sporadic cases have also been reported in Europe and the Americas [10].
Data for confirmed cases of cholera was obtained from the Gastrointestinal Bacteria Reference Unit (GBRU), UKHSA Colindale.
Between 2015 and 2019 there were an average of 15 cases each year, with a peak of 17 cases in 2018. There were 2 cases reported in 2020 and 1 case in 2021, all of which were confirmed cases and were reported in England. No cases were reported from Wales or Northern Ireland during this time period. The decrease in cases in 2020 and 2021, coincides with the COVID-19 pandemic where international travel and the number of travel-associated infections imported into the UK greatly reduced.
One case in 2020 was under 19 years old and the other was in the 60 to 69 year age group. The case in 2021 was in the 20 to 29 year age group. In 2020, 1 case reported travel to India and the other reported travel to Pakistan. The case in 2021 reported travel to Bangladesh. Cholera is known to be a risk in these 3 countries in Southern Asia.
Dengue
Dengue is a mosquito-borne infection transmitted by the bite of an infected female Aedes mosquito. It is caused by a virus from the Flaviviridae family and has four main serotypes: DEN-1, 2, 3 and 4. Illness is characterised by an abrupt onset of fever often accompanied by severe headache and pain behind the eyes, muscle pain, joint pains, nausea, vomiting, abdominal pain and loss of appetite; however, symptoms can range from mild or non-existent to severe. Severe dengue is rare in travellers. Dengue is endemic in over 100 countries across Africa, the Americas, the Eastern Mediterranean, South-East Asia and the Western Pacific, with sporadic cases occurring in other countries in Europe [11].
Data for cases of dengue was obtained from the Rare and Imported Pathogens Laboratory (RIPL), UKHSA Porton.
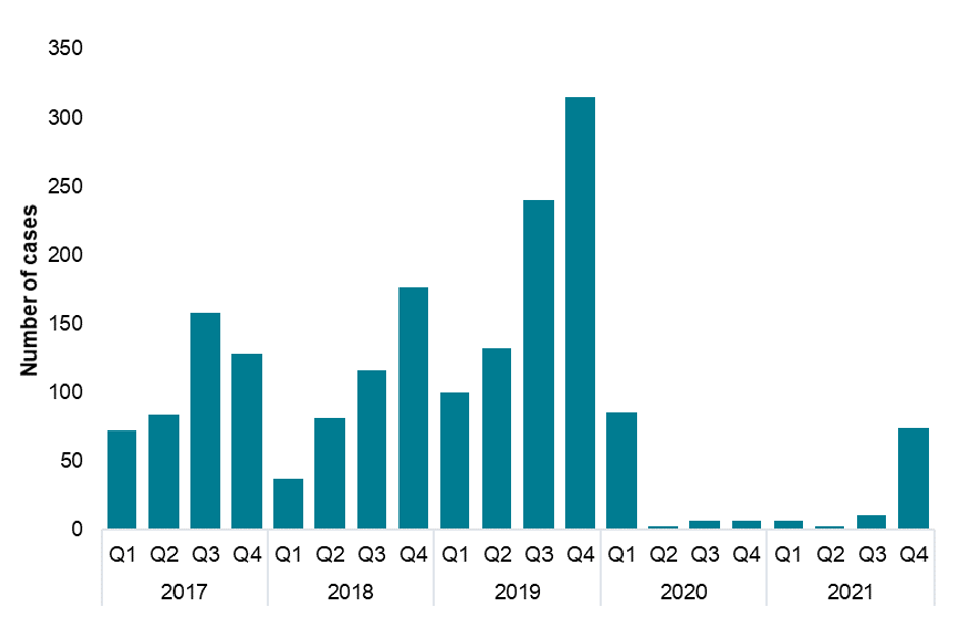
In EWNI, between 2015 and 2019 there were an average of 505 dengue cases reported each year, with a peak in 2019 of 787 cases. There were 102 dengue cases reported in 2020 (101 in England and 1 in Wales), which was an 87% decrease compared to 2019. Of these, 86 (84%) were confirmed cases and 16 (16%) were probable cases. There were 95 cases reported in 2021 (93 in England, 1 in Northern Ireland and 1 in Wales), of which 87 (92%) were confirmed cases and 8 (8%) were probable cases. The large decrease in cases in 2020 and 2021 compared to 2019 coincides with the COVID-19 pandemic where international travel greatly reduced and so there were fewer cases of travel-associated infections, which could explain this change. The majority of cases (n=85) were diagnosed in the first quarter of 2020 and case numbers then greatly decreased with 3 cases in the second quarter and 7 cases in each of the final quarters of 2020 (Figure 3). Case numbers remained low for the first three quarters in 2021 (n=7, n=3, n=11) and there was a large increase in the fourth quarter with 74 cases diagnosed. This aligns with public health advice to stop travelling at the end of March 2020 due to the COVID-19 pandemic and travel re-opening later in 2020, before the biggest increases in travel occurring later in 2021.
Figure 3. Cases of dengue by quarter, Q1 2017 to Q4 2021
In 2020, 51 cases (50%) were female (aged 15 to 83 years, median=36) and 45 (44%) were male (aged 7 to 80, median=36, Table 4). In 2021, 30 cases (32%) were female (aged 15 to 69 years, median=42) and 61 (64%) were male (aged 5 to 73, median=39). There were 6 cases with unknown sex in 2020 and 4 in 2021.
Table 4. Cases of dengue by age group and sex, 2020 and 2021
| Age group | Female (2020) | Male (2020) | Unknown (2020) | Female (2021) | Male (2021) | Unknown (2021) |
|---|---|---|---|---|---|---|
| Under 19 | 6 | 8 | 1 | 1 | 6 | 1 |
| 20-29 | 13 | 12 | 1 | 6 | 9 | – |
| 30-39 | 9 | 5 | 3 | 7 | 17 | 3 |
| 40-49 | 5 | 7 | – | 10 | 16 | – |
| 50-59 | 11 | 7 | 1 | 4 | 7 | – |
| 60-69 | 4 | 3 | – | 2 | 4 | – |
| 70 and over | 3 | 3 | – | – | 2 | – |
| Total | 51 | 45 | 6 | 30 | 61 | 4 |
In 2020, travel history was known for 84 out of 102 cases (82%), with the majority of these reporting travel to South-Eastern Asia (24 cases, 23%) and the Caribbean (21 cases, 20%, Table 5). In 2021, travel history was known for 79 out of 95 cases (83%), with the majority of these reporting travel to Southern Asia (64 cases, 67%). The most frequently reported country of travel was Jamaica in 2020 (10 cases) and India in 2021 (41 cases). The COVID-19 pandemic had a large impact in Southern Asia during 2021 when the highly transmission Delta (B.1.617.2) variant was circulating in the region and there was increased pressure on national health systems. There were also reported dengue outbreaks in the region during 2021, including in both India and Bangladesh [12, 13]. Travel data from the ONS International Passenger Survey demonstrates that there was an increase in the number of visits to India and other countries in Southern Asia by UK residents. which started in Q2 (April to June) and continued in Q3 (July to September) and Q4 (October to December) [14].
Table 5. Cases of dengue by age group and sex, 2020 and 2021
| Region of travel | 2020 | 2021 |
|---|---|---|
| South-Eastern Asia | 24 | 3 |
| Caribbean | 21 | 5 |
| Southern Asia | 16 | 64 |
| Eastern Africa | 8 | 2 |
| South America | 8 | – |
| Central America | 5 | – |
| Western Asia | 2 | 1 |
| Oceania | 2 | – |
| Middle Africa | 1 | – |
| Northern America | 1 | – |
| Western Africa | – | 4 |
| Not stated | 18 | 16 |
| Total | 106¥ | 95 |
¥ Note that some cases travelled to more than one region; all regions are included here so the total is higher than the actual number of cases.
Yellow fever
Yellow fever is a vaccine preventable mosquito-borne infection transmitted by the bite of multiple species of infected mosquitoes, including Aedes and Haemogogus species. Yellow fever virus is a flavivirus from the Flaviviridae family. Yellow fever is endemic in all or parts of 47 countries in Africa and Central and South America. The virus incubates in the body for 3 to 6 days post infection. Many people do not develop symptoms but for those who do, these may include fever, headache, nausea or vomiting, muscle pain (often with backache), and loss of appetite. Most people will make a full recovery after 3 to 4 days, however a small number (approximately 15%) will progress to a second phase of the infection and go on to develop jaundice, abdominal pain, renal failure and haemorrhage (bleeding). Up to half of infections in cases who develop severe symptoms may result in death. Yellow fever is rare in international travellers as there is a safe and effective vaccine available. Although the vaccine is safe, there have been reports of rate adverse events associated with its use [15].
Data for cases of Yellow fever was obtained from the Rare and Imported Pathogens Laboratory (RIPL), UKHSA Porton.
The most recently reported case in EWNI was in 2018 in a traveller who had visited Brazil. Prior to 2018, the last reported case in the UK was a laboratory technician who was working with the Yellow fever virus in London in the 1930s.
Zika
Zika is a mosquito-borne infection transmitted by the bite of an infected female Aedes mosquito. It is caused by a virus from the Flaviviridae family. Transmission is also known to occur through sexual transmission and can be transmitted congenitally from a pregnant woman to her foetus through the placenta. There have also been reports of transmission through blood transfusion [16]. The majority of people with Zika infection do not develop symptoms. Those that do often have mild symptoms which can include fever, headache, malaise, joint and muscle pain, a rash, itching, conjunctivitis and swollen joints [17]. Serious complications are uncommon, however an infection with Zika is a cause of Congenital Zika Syndrome (microcephaly and other congenital anomalies) and neurological complications such as Guillain-Barré Syndrome.
There was an outbreak of Zika virus infection in the Americas and the Caribbean in 2015-2016, during which time the first cases were recorded in the UK. As of 2019, 87 countries have reported autochthonous Zika cases across Africa, the Americas, South-East Asia and the Western Pacific [16, 18].
Data for cases of Zika was obtained from the Rare and Imported Pathogens Laboratory (RIPL), UKHSA Porton.
The number of travel-associated Zika cases in EWNI peaked in 2016 with 275 cases, before decreasing in subsequent years. There was 1 case reported in 2020 and 1 case in 2021, which were both confirmed cases and were reported in England. No cases were reported from Wales or Northern Ireland during this time period. There was a decrease in cases in 2020 and 2021, which coincides with the COVID-19 pandemic where international travel and the number of travel-associated infections imported into the UK greatly reduced, however the number of imported Zika infections has been low for a number of years. Both cases in 2020 and 2021 were between 30 and 50 years old. The case in 2020 reported travel to Thailand and the case in 2021 reported travel to India. Zika virus is known to be a risk in both countries.
References
1. ONS. ‘Coronavirus and the impact on the UK travel and tourism industry’
2. ONS. ‘Overseas travel and tourism: 2020’
3. ONS. ‘Overseas travel and tourism, provisional: April to June 2021’
4. ONS. ‘Overseas travel and tourism, UK, provisional: July to September 2021’
5. ONS. ‘Travel trends: 2021’
6. ONS. ‘International Passenger Survey’
7. WHO. ‘Chikungunya factsheet’ (updated 15 September 2020)
8. Alayu M, Teshome T, Amare H, Kinde S, Belay D, Assefa Z (2021). ‘Risk factors for Chikungunya virus outbreak in Somali region of Ethiopia, 2019: unmatched case-control study.’ Advances in Virology: volume 2021
9. WHO (2017). ‘Cholera vaccines: WHO position paper ’
10. WHO (2021). ‘Cholera Annual Report 2020.’ Weekly Epidemiological Record: volume 96 (37), pages 445 to 460
11. WHO. ‘Dengue and severe dengue factsheet’ (updated 10 January 2022)
12. ECDC (2021). ‘Communicable disease threats report, 24-30 October 2021, week 43’
13. Hossain MS, Amin R, Mosabbir AA (2022). ‘COVID-19 onslaught is masking the 2021 dengue outbreak in Dhaka, Bangladesh).’ PLOS Neglected Tropical Diseases: volume 16, issue 1
14. WHO. ‘Travelpac: travel to and from the UK, 2021 edition’
15. WHO. ‘Yellow fever factsheet’ (updated 7 May 2019)
16. WHO. ‘Zika virus factsheet’ (updated 20 July 2018)
17. PHE. ‘Zika virus: symptoms and complications guidance’ (updated 2 August 2017)
18. WHO. ‘Zika epidemiological update - July 2019)’