Coroners statistics 2020: England and Wales
Published 13 May 2021

© Crown copyright 2021
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/statistics/coroners-statistics-2020/coroners-statistics-2020-england-and-wales
1. Main Points
The statistics presented in this publication cover the Covid-19 pandemic period. During this period, the government passed the Coronavirus Act 2020 which introduced temporary easements to death management and affected the way deaths have been reported to Coroners. Caution should therefore be used when making comparisons to previous years.
| Decrease in the number of deaths reported to coroners in 2020 | 205,400 deaths were reported to coroners in 2020, the lowest level since 1995[footnote 1] – down 3% (5,500) compared to 2019. |
| 34% of all registered deaths were reported to coroners in 2020 | The proportion of registered deaths in England and Wales that were reported to coroners has decreased by six percentage points compared to 2019, the lowest proportion since 1995. |
| Deaths in state detention, up 18% in the last year | 562 deaths in state detention were reported to coroners in 2020 (up from 478 in 2019), the increase is driven by a 52% and 6% rise in deaths of individuals detained under the Mental Health Act 1983 and in prison custody respectively. |
| Post-mortem examinations were carried out on 39% of all deaths reported in 2020 | There were 79,400 post-mortem examinations ordered by coroners in 2020, a 3% decline compared to 2019. However, the proportion of reported deaths requiring a post-mortem has remained stable over the same period. |
| 7% more inquests opened in 2020 | 32,000 inquests were opened in 2020, up 7% compared to 2019. |
| Inquest conclusions down 1%, the largest fall seen in killed unlawfully, road traffic collision and open conclusions | In 2020, 30,900 inquest conclusions were recorded in total, down 1% on 2019. Killed unlawfully, road traffic collision and open conclusions had the largest decreases, down 55%, 22% and 20% on 2019, to 61, 774 and 1,207 inquest conclusions in 2020 respectively. |
| Average time taken to complete an inquest remained stable | The estimated average time taken to process an inquest remained stable at 27 weeks in 2020. |
This annual publication presents statistics of deaths reported to Coroners in England and Wales in 2020. Information is provided on the number of deaths reported to coroners, post-mortem examinations and inquests held, and conclusions recorded at inquests. A map reference of Coroner areas in England and Wales is available in the supporting document published alongside this bulletin. For previous editions of this report please see: www.gov.uk/government/collections/coroners-and-burials-statistics.
2. Statistician’s comment
2020 has been an unprecedented year; the covid-19 pandemic and corresponding restrictions have had a wide effect on all aspects of life in the United Kingdom. This publication covers the work of all coroners across England and Wales, including figures on inquests and post-mortems examinations held, and so any activity in this area may well have been affected by Covid-19.
All deaths in England and Wales must be registered, but the coroner only has a duty to investigate certain deaths. The coroner’s duty to investigate only arises when the coroner has reason to believe that the death is violent, unnatural, the cause of death is unknown or occurring in custody or other state detention. Where a death is from natural causes (for example, from a naturally occurring disease) in most cases that death will not need to be reported to the coroner.
These statistics help to understand those deaths reported to coroners, post-mortem examinations and inquests held, and conclusions recorded at inquests in England and Wales.
2020 saw the highest number of registered deaths in England and Wales since 1995. Provisional figures for 2020 show an increase to 608,016 registered deaths – the highest number in absolute terms since 1995 – as a result of the Covid-19 pandemic. However, in the same year, deaths reported to coroners, which form only a proportion of all registered deaths, decreased to their lowest level - 205,438, since 1995. This is likely a function of the numbers of registered deaths caused by Covid-19 infection, the majority of which will have been of natural cause. This will have meant that a greater proportion than usual of all deaths were from natural causes and therefore did not require a report to the coroner.
There was a small fall (of 1%) in inquest conclusions between 2019 and 2020. The most common inquest conclusion reached by Coroners was Accident/Misadventure - which accounted for nearly a quarter of conclusions, but which was also at its lowest level since our records began. Despite the small fall in the number of total conclusions, the number of verdicts of drug-alcohol related deaths increased by 12% to its highest level since 2014. However, there were falls in other conclusions such as those killed unlawfully (down 55% to its lowest level since 1995), those involved in a road traffic collisions (down 22% since 2019), and suicide (down by 3% on 2019).
At the height of the pandemic, many jury and non-jury complex inquests were halted. Many coroners have, however, been able to hear routine inquests throughout, either on the papers or with courts using audio and videoconferencing. This has been associated with the time taken to process an inquest remaining at 27 weeks, a similar level to last year.
2.1 About the Statistics
The coroner has a duty to investigate only certain deaths. The duty to investigate only arises when the coroner has reason to believe that the death is violent, unnatural, the cause of death is unknown or occurring in custody or other state detention. These statistics help to understand those deaths reported to coroners, post-mortem examinations and inquests held, and conclusions recorded at inquests in England and Wales.
The legal framework under which coroners operate exists in statute and can be found here.
2.2 Covid-19 deaths and Coroner statistics
COVID-19 deaths are likely to be considered to be deaths from natural illness, and therefore will not of themselves be reported to coroners, apart from deaths which the coroner is under a statutory duty to investigate and hold an inquest (essentially deaths in custody or other forms of state detention). Inquests are usually opened in less than 20% of all deaths reported to coroners. In such cases, Coroners are required to provide us with the conclusions of these inquests. The list of short form inquest conclusions which the coroners can provide is set out in legislation and can be found in Table 7 of the coroners’ publication.
2.3 Summary of relevant Policy Changes due to Covid-19[footnote 2]
The government introduced emergency legislation, the Coronavirus Act 2020, in March 2020 to help various services cope with the effects of the pandemic.
Medical Certificates of Cause of Death (MCCD)
Any registered medical practitioner can sign an MCCD. This is even if the deceased was not attended during their last illness and not seen after death, provided that they are able to state the cause of death to the best of their knowledge and belief.
Once that MCCD reaches the registrar there are two possibilities depending on whether the deceased was seen before or after death. If a medical practitioner (who does not have to be the same medical practitioner who signed the MCCD) attended the deceased within 28 days before death (a new, longer timescale) or after death, then the registrar can register the death in the normal way. Second, if there was no attendance either within 28 days before death or after death, then the registrar would need to refer that to the coroner.
Medical practitioners’ duty to notify coroners
The Notification of Deaths Regulations 2019 provide that a registered medical practitioner must notify the coroner where:
-
it is reasonably believed that there is no attending medical practitioner required to sign the MCCD; or
-
it is reasonably believed that the attending medical practitioner required to sign the MCCD is not available to do so within a reasonable time of death.
The emergency legislation disapplies this requirement because, as set out above, the medical practitioner who signs the MCCD does not need to have attended. The duty on a medical practitioner to notify the coroner only applies during the emergency period where it is reasonably believed that there is no other medical practitioner who may sign the MCCD or that such a medical practitioner is not available within a reasonable time of the person’s death to do so.
COVID-19 as a notifiable death and jury inquests
COVID-19 was classified as a notifiable death under the Health Protection (Notification) Regulations 2010 in March 2020. Notifiable in this context means notifiable to the public health authorities, not notifiable to the coroner for the purpose of death investigation. Where the coroner has reason to suspect death was caused by COVID-19 and decides to open an inquest, section 30 of the Act removes the requirement for an inquest to be held with a jury.
2.4 Data and Methodology and related sources of information
-
Coroners in England and Wales have continued to provide the data which is the basis of these statistics and proactively engaged with statisticians to ensure this report was produced in a timely manner and to high standards.
-
The coronavirus pandemic has led to changes to the way coroners investigate deaths reported to them. They have had to be flexible and innovative in the way they conduct their inquests due to social distancing requirements.
-
Caution should be taken when making comparisons between regions of the coronial activities – post-mortems, inquests, timeliness - due to the restrictions based on the tier system around the country. Local authority set-up, resource, facilities and socio-economic make up mean this will not be comparing like with like.
-
Jury inquests have been particularly affected by social distancing requirements.
-
Pressure on NHS front line services has meant that clinicians have not always been available to attend inquests, causing delays, although many have attended remotely, a trend which is likely to continue after the pandemic.
2.5 Covid-19 deaths Signposting
Statistics relating specifically to Covid-19 related deaths can be found in the links below:
- The Office for National Statistics (ONS) publishes covid-19 related deaths here: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths
- The Ministry of Justice also publishes statistics relating to Covid-19 related State detention/prison deaths in the links below: https://www.gov.uk/government/statistics/hmpps-covid-19-statistics-december-2020 and https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/944911/deaths-offenders-community-2019-20-bulletin.pdf
3. Deaths Reported
3% decrease in the number of deaths reported to coroners in 2020
205,438 deaths were reported to coroners in 2020, the lowest level since 1995. This is a decrease of 5,474 (3%) from 2019.
34% of all registered deaths were reported to coroners in 2020
The percentage of all registered deaths that were reported to coroners has decreased by six percentage points when compared to 2019, the lowest level since 1995.
All deaths in England and Wales must be registered with the Registrar of Births and Deaths and statistics on all deaths are published by the ONS. The ONS mortality statistics, based on death registrations, report the number of deaths registered in England and Wales in a particular year irrespective of whether a coroner has investigated the death. The Ministry of Justice’s coroner statistics provide the number of deaths which are reported to coroners in England and Wales. Further background information is provided in Chapter 1 of the supporting guidance document.
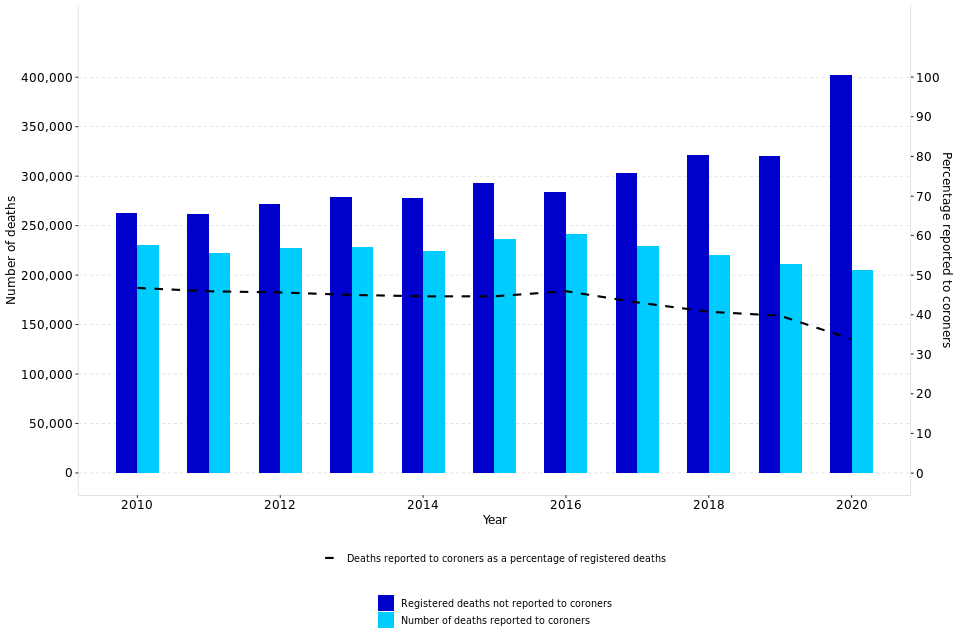
The number of deaths reported to coroners in 2020 decreased by 5,474 (3%) to 205,438, the lowest level since 1995. In comparison, ONS registered deaths rose 77,175 (15%)[footnote 3] from 2019 to 2020. The proportion of registered deaths in 2020 that were reported to coroners was 34%, down six percentage points from 2019.
The number of registered deaths in England and Wales has been broadly increasing, from a low of 484,367 in 2011 before gradually rising to 541,589 in 2018. 2019, however, saw a decrease to 530,857. Provisional figures for 2020 show an increase to 608,016 – the highest level it has been in absolute terms, due to the Covid-19 pandemic. The number of deaths reported to coroners initially followed a similar trend, from a low of 222,371 in 2011 and then rising to a high of 241,211 in 2016. However, in contrast to deaths registered in 2017, 2018 and 2020, deaths reported to coroners over the last four years fell (there was a decrease in both deaths registered and deaths reported in 2019), as shown in figure 1. This shows a reversal to similar broadly stable levels seen prior to 2015, before the impact of Deprivation of Liberty Safeguard on 2015, 2016 and 2017 figures.
Figure 1: Registered deaths and deaths reported to coroners, England and Wales, 2010-2020 (Source: Table 2)
Out of England and Wales Orders
To take the body of a deceased person out of England and Wales, notice must be given to the coroner within whose area the body is lying. When the coroner gives permission for the removal of a body, an Out of England and Wales order is issued.
Coroners issued 4,711 Out of England and Wales orders in 2020, compared with 5,632 issued in 2019. In 2020, the number of orders issued represented 2% of the total number of deaths reported to coroners, ending the consistently rising trend seen since 2015, most likely due to travel restrictions put in place in response to the pandemic, (see Table 5).
Deaths abroad
Travel and tourism have been significantly impeded by the Coronavirus pandemic. This has led to a significant drop this year in deaths abroad where the body has been repatriated and led to a coroner investigation. Such deaths decreased by 60% in 2020 compared to the same period a year earlier, the lowest it has been since before 2010. Of the 205,438 deaths reported to coroners in 2020, less than 1% (771) were reports of deaths that had occurred outside England and Wales, a slight decrease compared to 2019.
4. Deaths in State Detention
Deaths in state detention, up 18% in the last year
Deaths in state detention reported to coroners increased by 18% to 562 in 2020, driven by a rise in number of deaths of individuals in prison custody and those detained under the Mental Health Act 1983 (as amended).
In 2020, a total of 562 deaths which occurred in state detention were reported to coroners[footnote 4], an increase of 84 deaths (18%) on the previous year and representing less than 1% of all deaths reported to coroners.
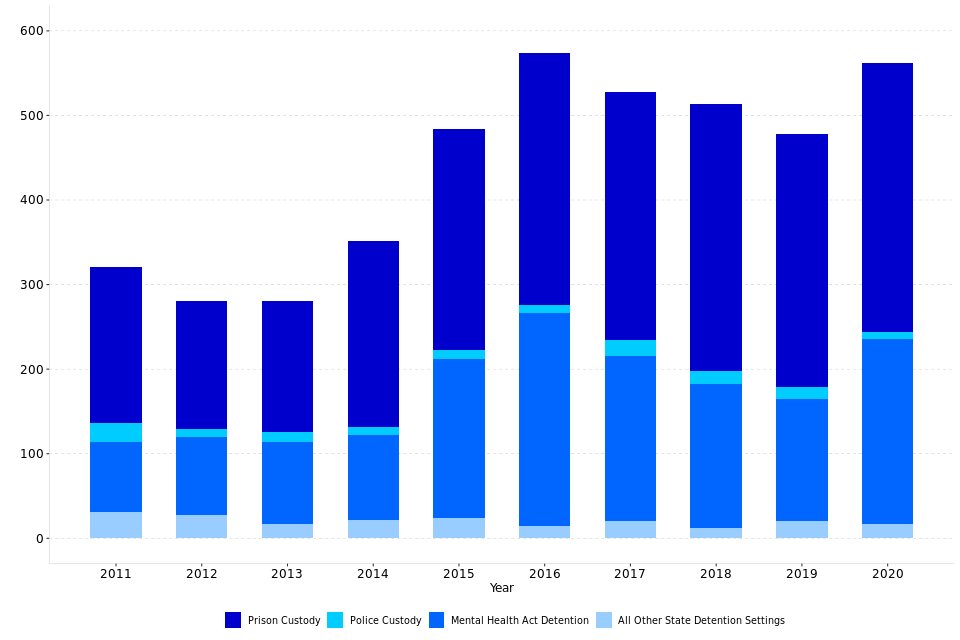
There were 219 deaths of individuals subject to Mental Health Act detention in 2020, a 52% increase (75 cases) compared to 2019. The Care Quality Commission reported 240 deaths under the Mental Health Act 1983 (as amended)[footnote 5] in financial year 2019/20, up 23% on the number they reported in 2018/19 (195 deaths). The number of deaths in prison custody increased by 6% (19 cases) compared to 2019, to 318 deaths in 2020.Her Majesty’s Prison and Probation Service (HMPPS) reported 318 deaths in prison custody in 2020 (Safety in Custody Statistics[footnote 6]), up 6% on the number they reported in 2019 (300 deaths).
From 2015 to 2017 the inclusion of deaths under a Deprivation of Liberty Safeguard (DoLS) led to a distortion of the long-term trend seen in the number of deaths in state detention. This requirement was removed from 1 April 2017 and as such the deaths under DoLS have been plotted excluded from Figure 2 below, in order to aid year-on-year comparison of figures. For more information on DoLS please refer to the supporting guidance which accompanies this bulletin. There has been a general rise in deaths in state detention since 2011, although the number decreased from 2017 until 2020.
Figure 2: Number of deaths in state detention (excluding DoLS), by type of detention, 2011-2020 (Source: Table 6)
5. Post-Mortem examinations held
Post-mortem examinations were carried out on 39% of all deaths reported in 2020
There were 79,357 post-mortem examinations ordered by coroners in 2020, 39% of all cases reported to them (no change compared to 2019).
Post-mortem examinations were held for 79,357 deaths reported to coroners in 2020, down 2,715 (3%) from 2019. This represents 39% of all deaths reported to coroners in 2020, the same proportion as in 2019.
Figure 1 of the supporting guidance document provides an overview of the possible outcomes when a death is reported to a coroner, including circumstances involving a post-mortem.
Figure 3: Post-Mortems as a percentage of deaths reported to coroners, England and Wales, 2010-2020 (Source: Tables 3-4)
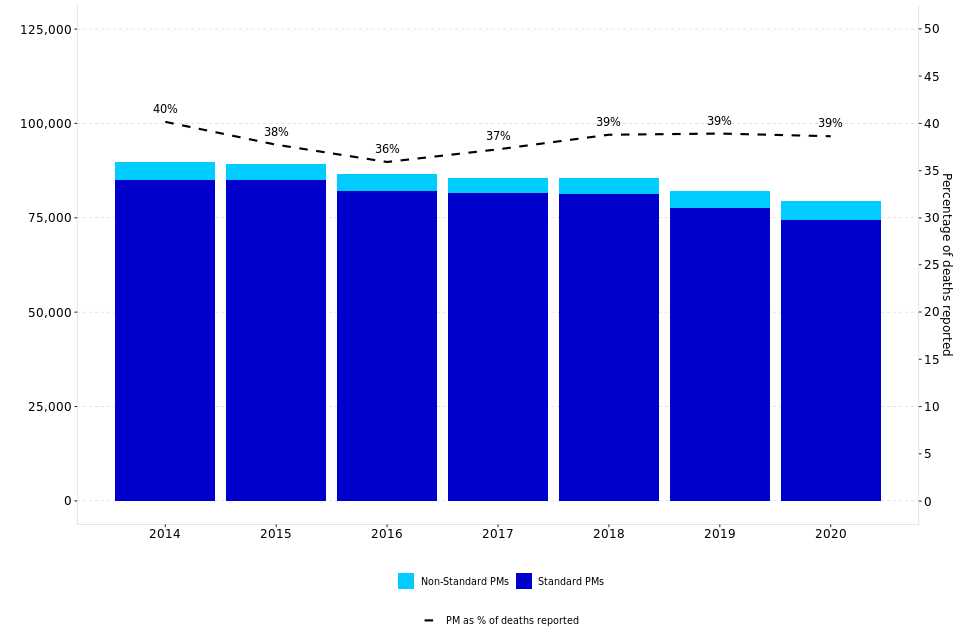
Post-mortem examinations may be classified as either standard or non-standard, depending on the nature of the examination. A non-standard post-mortem is defined as a post-mortem which requires special skills. A non-standard post-mortem could, for example, require a pediatric or other specialist pathologist. In 2020, almost all (94%) of post-mortems were ordered at a standard rate – this proportion is one percentage point lower than in 2019.
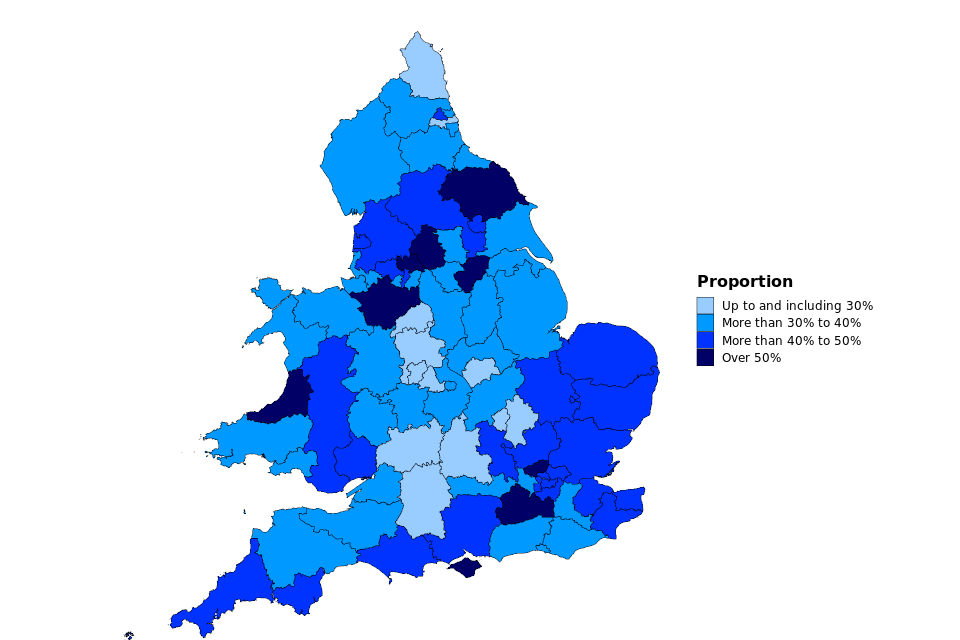
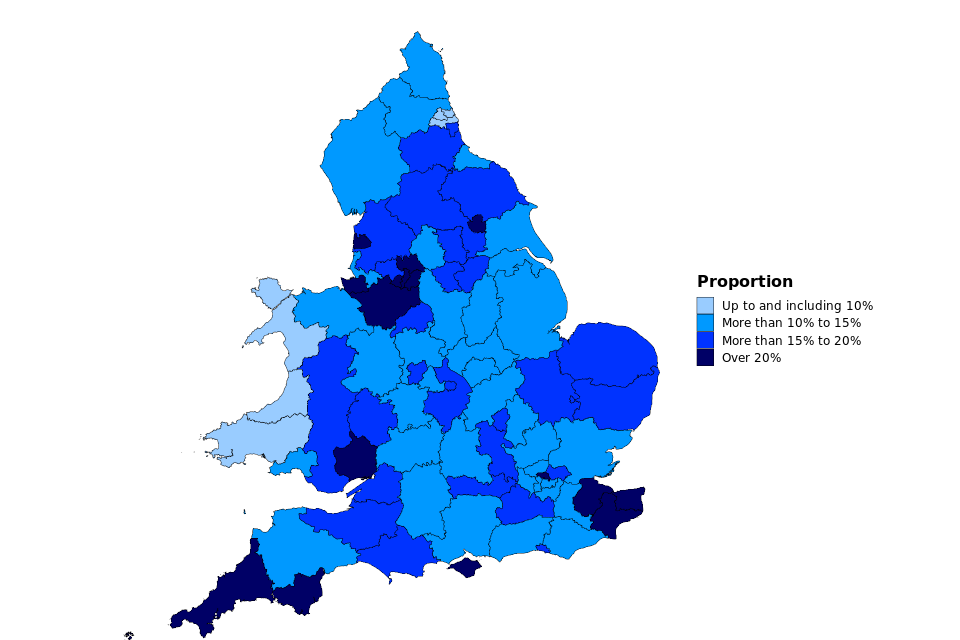
The proportion of post-mortems carried out varies from 16% of deaths reported in Staffordshire South to 63% in North Yorkshire (Eastern), as shown by Map 1.
Map 1: Post-Mortem Examinations held as a proportion of deaths reported to coroners, England and Wales, 2020
Post-mortem examinations in inquest cases
A post-mortem examination will often be held before the coroner decides whether to open an inquest. In 2020, 55% of inquest cases involved a post-mortem, down three percentage points on 2019.
Post-mortem examinations in non-inquest cases
In the majority (81%) of deaths referred to coroners, there is no inquest. In 2020, there were 56,351 non-inquest cases where a post-mortem was held. The percentage of non-inquest cases that required a post-mortem has not changed, 34% in both 2019 and 2020. This figure has remained fairly stable since 2017. There had previously been a downward trend since the beginning of the series (56% in 1995 to 32% in 2016).
Post-mortem examinations in potential inquest cases
Prior to July 2013 when the Coroners and Justice Act 2009 was implemented, deaths were either categorised as ‘inquest’ or ‘non-inquest’ cases. Changes in the way coroners investigate mean that there is now a third category of ‘potential inquest’ cases. This means that the coroner has opened an investigation into the death but has not yet decided whether it is necessary to hold an inquest. Depending on whether the coroner deems it necessary to hold an inquest, these cases will all eventually end up in either the ‘inquest’ or ‘non-inquest’ category. In 2020, there were 7,280 potential inquest cases being dealt with by coroners in England and Wales, with 73% requiring a post-mortem. The number of potential inquests in total has decreased by 17% in the past year.
Cases requiring neither a post-mortem nor inquest
There were 109,816 deaths reported to coroners where there was neither a post-mortem nor an inquest. This type of case has decreased by 4% in the current year and the number of cases reported is the lowest level since 2004. This continues the decreasing trend seen since 2017. The proportion of all deaths reported where there was neither an inquest nor a post-mortem examination has decreased by one percentage point to 53% in 2020. This implies that most deaths reported to coroners do not require inquests or post-mortems. Although this proportion has been slightly declining since 2018.
Histology, toxicology and less invasive post-mortems
In 2020, 21% (17,002) of all post-mortems included histology, a marginal decrease from 22% (18,123) in 2019. Post-mortems including toxicology increased by 511 cases over the same period to 19,802 (up 3%), with 25% of all post-mortems held in 2020 including toxicology - continuing the consistently rising trend seen since 2016.
There were 8,195 post-mortems conducted using less-invasive techniques and 5,844 using only less-invasive techniques (such as Computerised Tomography [CT] scans) in 2020. The number of post-mortems carried out using only less-invasive techniques varied from zero in 12 areas to 1,663 in Lancashire and Blackburn with Darwen. Lancashire and Blackburn with Darwen, Leicester City and South Leicestershire, Stoke-on-Trent and North Staffordshire, and Black Country conducted over a half (86%, 57%, 52% and 63% respectively) of all their post-mortems using only less-invasive techniques. South Yorkshire (Western), West Yorkshire (Western), and Gwent conducted over a quarter of all their post-mortems using less-invasive techniques (28%, 27% and 31% respectively).
This year we have provided a further breakdown for post-mortems to show the figures for second post-mortems which are often conducted following a request from a defence lawyer and post-mortems conducted by a Home Office (HO) forensic pathologist. 45 post-mortems were conducted following a request from a defence lawyer (less than 1% of all post-mortems) and 2% (1,635) of post-mortems in 2020 were conducted by a Home Office forensic pathologist.
6. Inquests Opened
7% increase in inquests opened in 2020
The number of inquests opened in 2020 increased by 2,022 (up 7%) to 31,991. In the last two years there has been an increase in the number of inquests opened despite a decrease in the number of deaths reported to coroners.
There were 31,991 inquests opened in 2020, a 7% increase on 2019. The number of inquests opened in 2018 and 2019 were mostly consistent with figures before DoLS investigation requirements (see section 4) were introduced (excluding 2014, which had 25,889). However, 2020 saw the second highest number of inquests opened since 1995, excluding the years when DoLS investigations were required.
Inquest cases represented 16% of all the deaths reported to coroners in 2020, an increase from 14% in 2019. The number of inquests opened as a proportion of deaths reported in 2020 varied across coroner areas, from 2% in Newcastle upon Tyne to 37% in Gwent. However, most coroner areas held inquests for between 10% and 20% of all deaths reported (63 of the 85 coroner areas). Map 2 shows the Inquests opened as a proportion of deaths reported in 2020 for all coroner areas in England and Wales.
Inquests with juries and suspended investigations
A jury is required by law in certain inquests, including non-natural deaths in custody or other state custody or where the police forces were involved. Holding inquests with juries has been a particular issue during the pandemic due to social distancing requirements, especially where for coroners whose area includes a prison (or prisons). Consideration for these issues should be taken into account when making comparisons to previous years’ figures.
There were 239 inquests held with juries in 2020 (representing 1% of all inquests), a decrease of 288 (55%) compared to 2019.
In 2020, 631 investigations were suspended (and not resumed) by the coroner under Schedule 1[footnote 7] of the Coroners and Justice Act 2009 because criminal proceedings took place. Of these, 599 had a inquest open at the time of suspension, representing 2% of all inquests concluded, down one percentage point compared to 2019.
Map 2: Inquests opened as a proportion of deaths reported to coroners, England and Wales, 2020
7. Inquest Conclusions
1% decrease in inquest conclusions recorded, with the largest fall seen in killed unlawfully, road traffic collision and open conclusions
In 2020, 30,936 inquest conclusions were recorded, down 1% on 2019. Inquest conclusions of killed unlawfully, road traffic collision and open conclusions were down 55%, 22% and 20% on 2019 to 61, 774 and 1,207 respectively.
There were 30,936 inquests conclusions recorded in 2020, down 348 (1%) from 2019. This is the lowest level since 2014. Background information on inquest conclusions is provided in Chapter 1 of the supporting guidance document.
In 2020, the most common short form conclusions (by order of frequency) were death by misadventure (7,513 or 24% of all conclusions), suicide (4,475 or 14%) and death from natural causes (3,845 or 12%). Unclassified conclusions (which include narrative conclusions) made up 21% (6,554) of all inquest conclusions in 2020.
This year saw the lowest killed unlawfully conclusions (61) since 1995, which may be due to pandemic restrictions reducing outdoor activity. The number of suicide conclusions fell, by 3%, compared to 2019. However, 4,475 is still the second highest number of suicide conclusions since 1995.
Figure 4: Number of conclusions recorded at inquests, England and Wales, 2010-2020 (Source: Table 7)
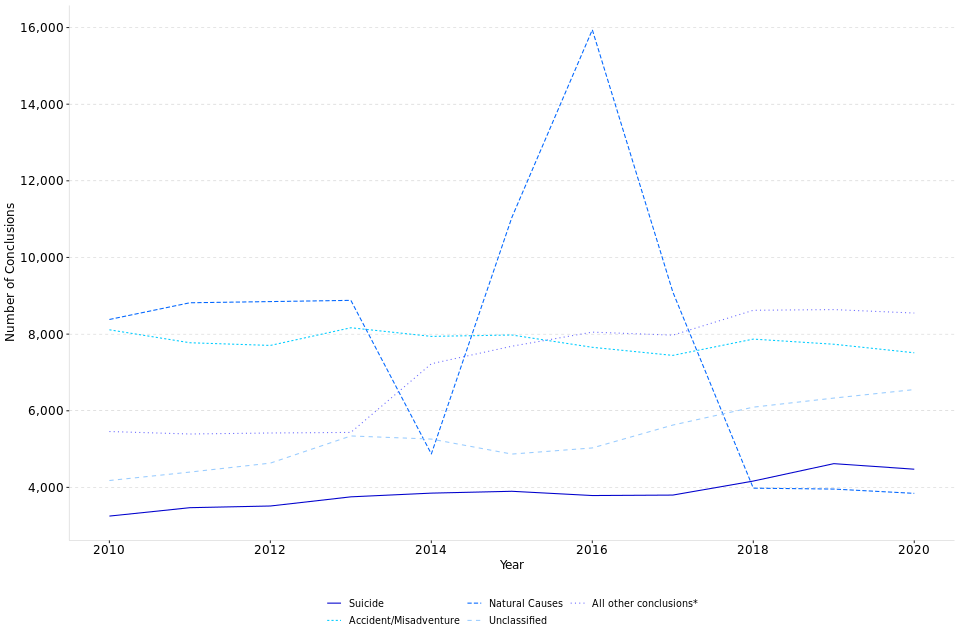
*Includes Killed unlawfully; Killed lawfully; Lack of care or self-neglect; Stillborn; Open; Industrial Disease; Drugs/Alcohol related[footnote 8]; and Road traffic collision.
In 2015 and 2016, there were significant increases in natural causes conclusions, driven by deaths of individuals subject to DoLS authorisations where the majority (94%) had an inquest conclusion of natural causes. In line with the reduction in the number of inquests opened and inquest conclusions following the removal of the requirement to report DoLS deaths, there was also a corresponding decrease in the number of natural causes conclusions in 2017 and 2018. In 2020, natural causes decreased 3%.
In 2020, the number of unclassified conclusions increased by 223 cases (up 4%) to 6,554. Unclassified conclusions made up 21% of all conclusions in 2020, one percentage point more than in 2019. The rise in unclassified conclusions seen until 2014 and again from 2016 is partly due to the increasing use of what are known as ‘narrative conclusions’ by some coroners. In these cases, the conclusion is recorded as unclassified. As well as narrative conclusions, this category includes short non-standard conclusions which a coroner or jury might return when the circumstances do not easily fit any of the standard conclusions[footnote 9].
The proportion of conclusions recorded as suicide remained broadly constant from 2010 to 2017, generally at around 11-12%. However, in 2018, 2019 and 2020, it accounted for 14%, 15% and 14% of all inquest conclusions respectively. This proportion varied from 5% in Gateshead and South Tyneside to 30% in Inner North London[footnote 10].
For the remaining conclusion types, alcohol/drugs related deaths have continued to increase. This year it increased by 426 cases (up 12%) to 3,840, the highest it has been since 2014.
Open conclusions have seen a decrease over the last decade - they accounted for 4% in 2020 compared with 7% in 2010.
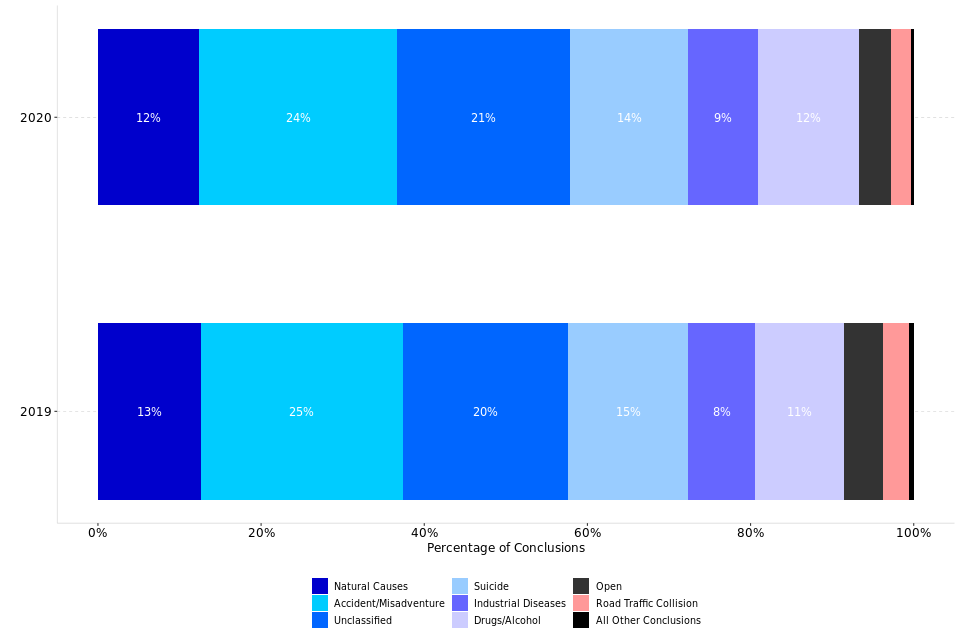
Figure 5 shows the proportion changes in inquest conclusions between 2019 and 2020.
Figure 5: Conclusions recorded at inquest, by category and as a proportion of all conclusions, England and Wales, 2019 and 2020 (Source: Table 7)[footnote 11] [footnote 12]
8. Inquest Conclusions by Sex
Conclusions recorded at inquests by sex[footnote 13]
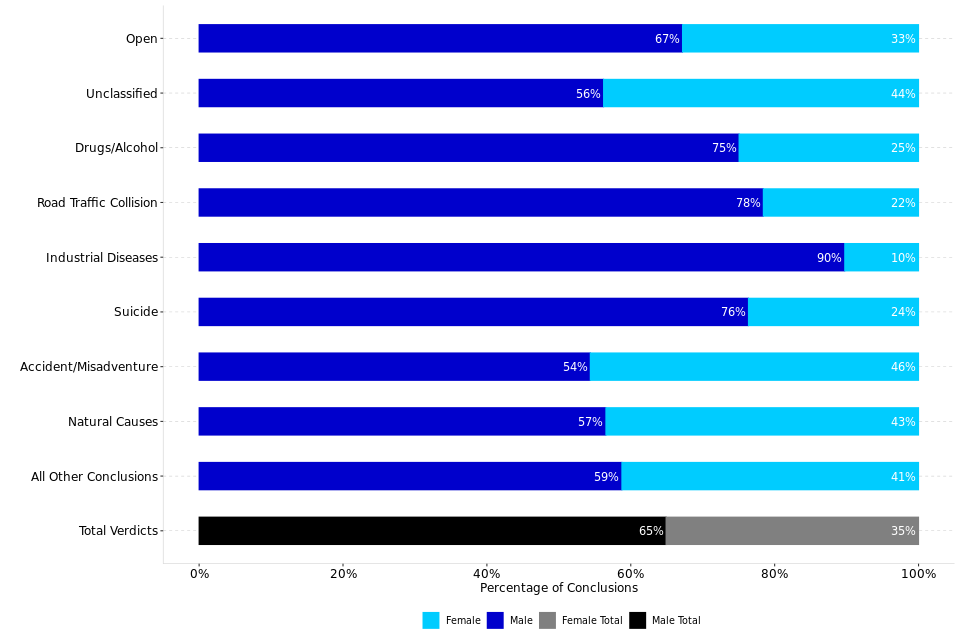
Male deaths accounted for 65% of all conclusions recorded in 2020 while female deaths accounted for 35%, the same percentages as in 2019.
The pattern of conclusions recorded differs between males and females. Males accounted for 57% of deaths reported but 65% of all conclusions recorded in 2020; this suggests that males are more likely to die in circumstances that lead to an inquest.
Correspondingly, female deaths accounted for 35% of all conclusions recorded in 2020 (and 43% of all deaths reported). Figure 6 shows the variation in the sex proportions, depending on the type on inquest conclusion. Industrial disease had the highest proportion of inquests relating to males, at 90%, and accident/misadventure had the highest proportion of inquests relating to females[footnote 14], at 46%.
Figure 6: Conclusions recorded at inquests by sex, England and Wales, 2020 (Source: Table 7)
9. Inquest Conclusions by Age
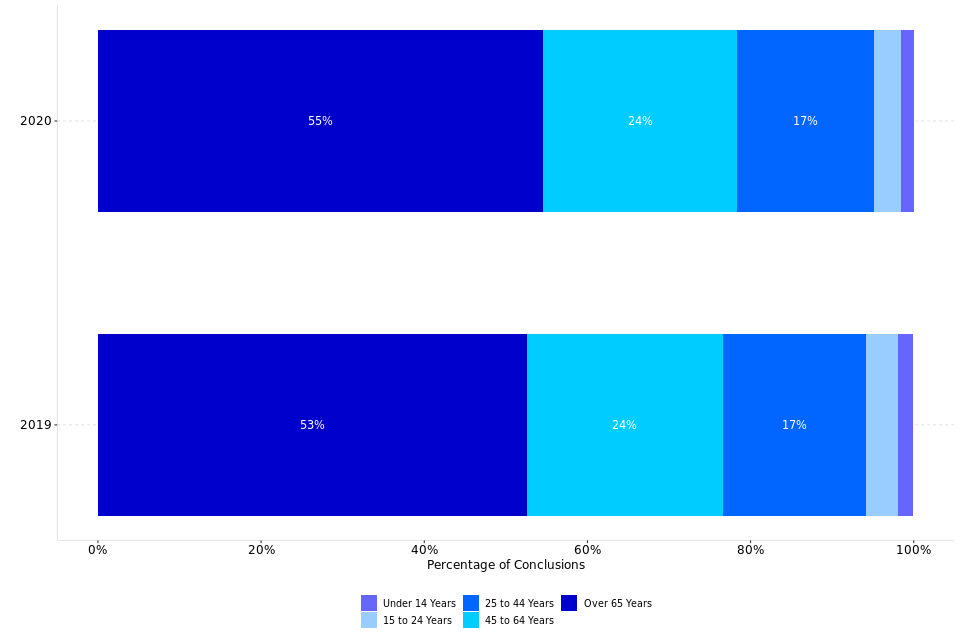
The majority of inquests completed were for those aged 65 years and over
Of the inquests completed in 2020, 55% related to persons who were aged 65 years or over at time of death compared with 5% relating to persons under 25 years of age.
The profile of the age of deceased at inquests has changed slightly from 2019 to 2020. The percentage of inquests completed relating to persons aged 65 or over has increased by two percentage points from 53% to 55%. By contrast, 5% of inquests concluded related to persons under 25 years of age, down from 6% in 2019, while the percentage of those between 25 and 65 years has decreased marginally from 42% to 41% (see Table 8).
Although an age breakdown of registered deaths in England and Wales in 2020 is not yet available, ONS figures for 2019[footnote 15] show that 85% of registered deaths in England and Wales were persons aged 65 or over, with only 1% aged under 25 years old.
Figure 7: Proportion of inquest conclusions by age of deceased, England and Wales, 2020 (Source: Table 8)[footnote 16]
10. Time taken to process an inquest
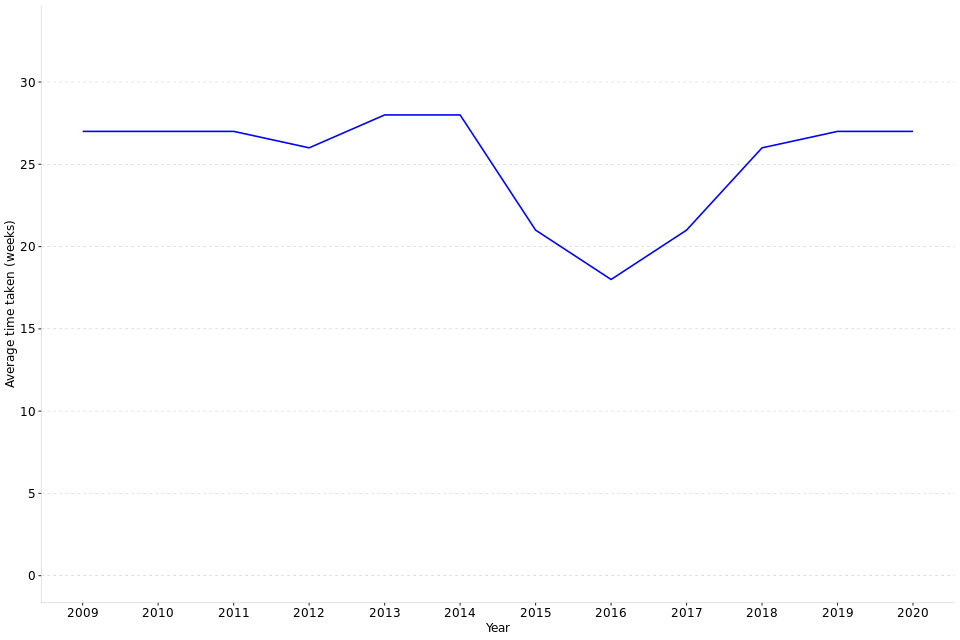
Overall, no change in the average time taken to process an inquest
The estimated average time taken to process an inquest remained stable at 27 weeks in 2020 compared to 2019.
The estimated[footnote 17] average time taken to process an inquest in 2020 (defined as being from the date the death was reported until the conclusion of the inquest) was 27 weeks (see Table 13)[footnote 18], so no change compared to 2019.
The decreases in time taken that occurred in 2015 and 2016 can largely be attributed to DoLS deaths where, in accordance with the Chief Coroner’s guidance, in uncontroversial cases, there could be a ‘paper inquest’, i.e. the Coroner in open court considered the evidence on the papers, which had been discussed in advance with the family (and interested persons) – this agreed process which usually did not require a post-mortem examination report took much less time to process and conclude – thus reducing the average time.
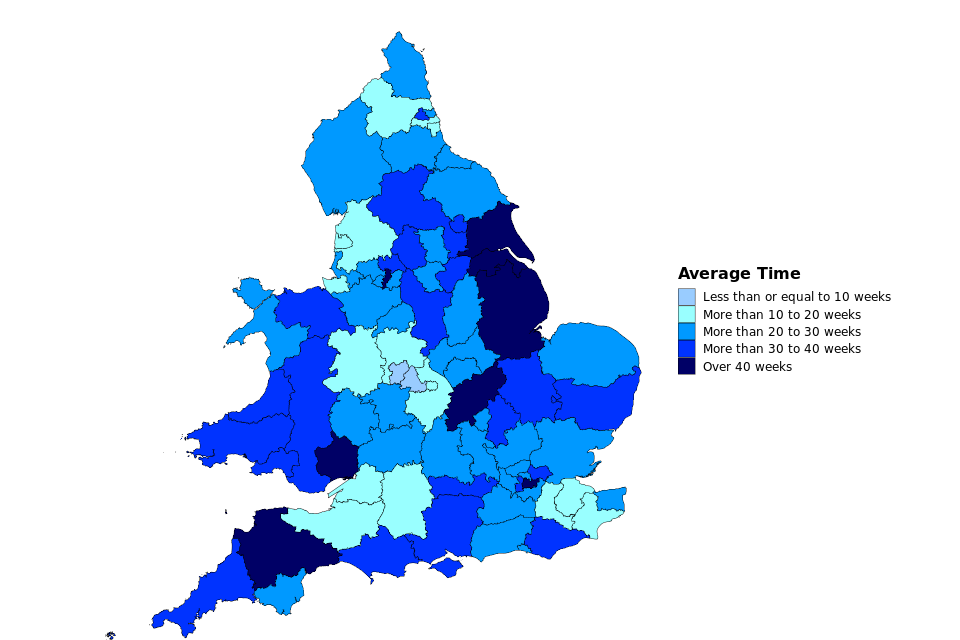
The time taken to process an inquest varies by coroner area - the maximum average time taken to process an inquest in 2020 was 50 weeks in North Lincolnshire and Grimsby, and the minimum average time was nine weeks in the Black Country. The large range of average time (41 weeks) may be due to the fact that the profile of coroner areas although there will be other factors including the resources provided to coroner services can vary greatly and a direct comparison between coroner areas is therefore not advised. Map 3 provides an overview of average time taken across coroner areas in England and Wales.
More information about how the average time taken has been estimated can be found in the Guide to coroners statistics published alongside this report.
Figure 8: Average time taken to process an inquest (in weeks), 2009-2020 (Source: Table 9)
Map 3: Estimated average time taken to process inquests, England and Wales, 2020
11. Treasure and Treasure Trove
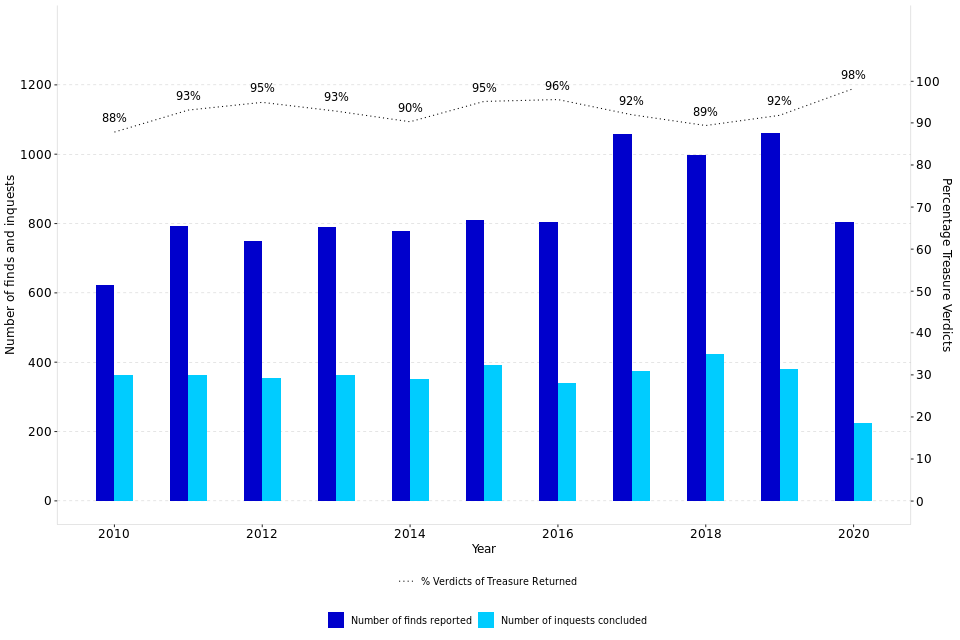
There was a 24% decrease in Treasure finds[footnote 19] reported in 2020 and a 41% decrease in inquest conclusions into finds
803 finds were reported to coroners in 2020, a decrease of 258 on 2019. 224 inquests were concluded into finds. Of these, 98% (220) returned a verdict of treasure, an increase in proportion by six percentage points when compared to 2019 and the highest since 2001.
In 2020, 803 finds were reported and 224 inquests were concluded. There were no inquests held into Treasure Trove in 2020 (relating to finds made before the Treasure Act 1996 came into force), however it is likely that a few such inquests will continue to be held from time to time.
The number of finds reported has historically been steadily increasing since the commencement of the 1996 Act in September 1997, from 54 finds in 1997 to 1,059 in 2017, before decreasing to 999 in 2018, then rising to 1,061 in 2019. In 2020 the number of finds fell to 803 (down 24%), likely due to pandemic restrictions.
Of those 224 inquests concluded in 2020, 98% (220) returned a verdict of treasure, a six percentage point increase compared to 2019 and the highest since 2001.
Figure 9: Finds reported to coroners, treasure inquests held under the Treasure Act, and proportion of Treasure verdicts returned, 2010-2020 (Source: Table 10)[footnote 20]
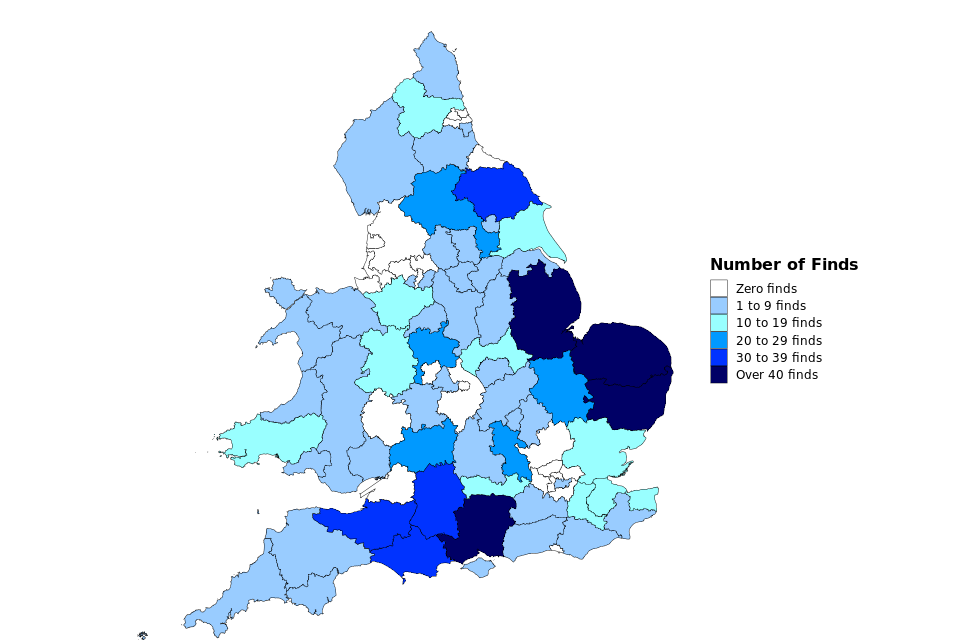
The number of finds and inquests held varies greatly across the country, most likely due to geographical and historical differences between areas. In 2020, 25 coroner areas had no treasure finds reported to them, whilst Norfolk had the highest number of treasure finds at 123. Map 4 shows treasure finds across England and Wales in 2020. More information about the duties of coroners to investigate treasure found within their jurisdiction and the provisions of the Treasure Act 1996 (and the previous Treasure Trove provisions) can be found in the supporting guidance
Map 4: Number of treasure finds reported to coroners, England and Wales, 2020
12. Annex A: Details of recent Coroner Area amalgamations
The following table summarises the coroner area amalgamation that have occurred during 2020. There were no amalgamations in 2019. For a list of all historical amalgamations and changes to coroner areas, please refer to the supporting guidance document.
| Date effective | Previous Coroner Area | New Coroner Area | Nature of merger |
|---|---|---|---|
| 01-Apr-20 | Central Hampshire; North East Hampshire; Portsmouth and South East Hampshire; Southampton and New Forest |
Hampshire, Portsmouth and Southampton | 4 into 1 |
13. Annex B: Further analysis of deaths reported to coroners
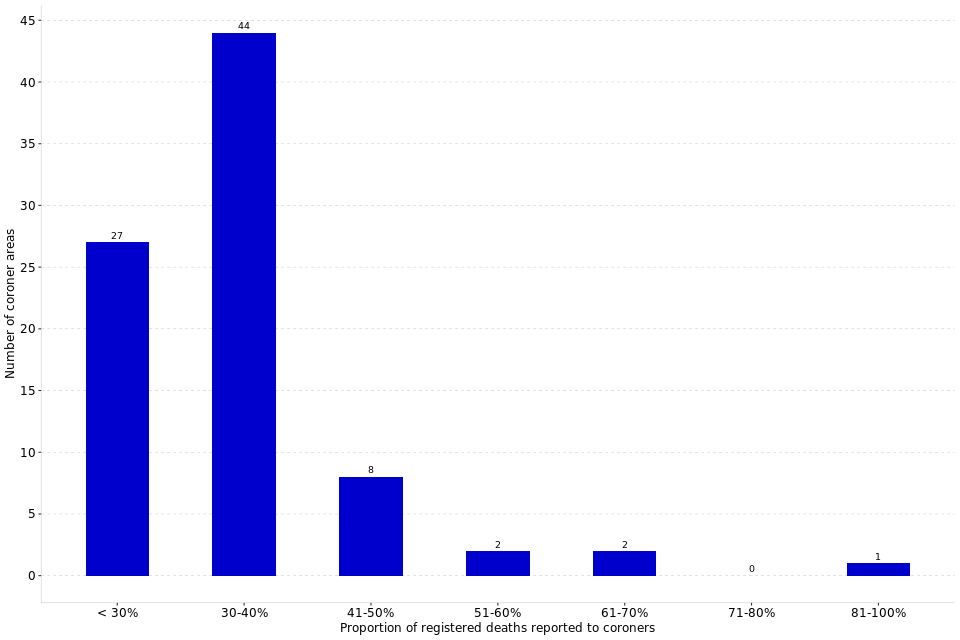
In 2020, the number of deaths reported to coroners as a proportion of registered deaths varied widely across coroner areas, from 16% in North Yorkshire (Western) to 82% in Gateshead and South Tyneside
The number of deaths reported to coroners in 2020 varied markedly by coroner area – from 239 in City of London to 6,880 in Hampshire, Portsmouth and Southampton. The number of deaths reported in each area will be affected by its size, population, demographic breakdown and profile so comparisons of deaths reported to coroners across coroner areas should be treated with caution.
When looking at the number of deaths reported to coroners in 2020 as a proportion of registered deaths[footnote 21], which allow for some differences in population characteristics, there is still a wide variation across coroner areas, with a minimum of 16% in North Yorkshire (Western) compared to the maximum of 82% in Gateshead and South Tyneside. However, caution should be taken when using these figures as local area factors can influence these proportions. For example, large hospitals near boundary lines can impact the proportion, due to the difference between the coroners’ figures being based on the place of death and the ONS figures being based on the place of residence.
The rollout since April 2019 of non-statutory medical examiners who examine deaths not reported to coroners based in NHS Trusts may explain a reduction in the number of deaths reported to coroners in some coroner areas.
Figure 10: Coroner areas split by the number of deaths reported to coroners in 2020 as a proportion of registered deaths (Source: Table 11)[footnote 22] [footnote 23]
13.1 Further Information
Revisions to statistics for previous years
The estimated figure for the number of registered deaths in 2019 which was derived from monthly data for the purposes of Table 2 in last year’s edition of this bulletin has now been replaced by the annual figure published by the Office for National Statistics.
Symbols and rounding convention
Within the ‘Key Findings’ sections, figures greater than 1,000 are rounded to the nearest 100. The following symbols have been used throughout the tables in this bulletin:
| n/a | = | Not applicable |
| - | = | Zero |
| .. | = | No data available |
| (p) | = | Provisional Data |
| (r) | = | Revised Data |
Accompanying files
-
This publication should be read alongside the statistical tables which accompany
-
There is also a supporting comma-separated values file (CSV) to allow users to carry out their own analysis
-
In addition to the bulletin and tables, we have published a coroners’ statistical tool. The tool provides easier access to local level data and allows the user to compare up to four areas of interest, for example, it is possible to compare a coroner area with a geographical region, England and/or Wales.
-
The accompanying guide to coroner statistics provides a more detailed overview of coroners; including the functions of coroners and the chief coroner, policy background and changes, statistical revision policies, and data sources and quality. It also includes a glossary with brief definitions for some commonly used terms.
-
The quality statement published with this guide sets out our policies for producing quality statistical outputs for the information we provide to maintain our users’ understanding and trust.
National Statistics Status
National statistics status means that official statistics meet the highest standards of trustworthiness, quality and public value.
All official statistics should comply with all aspects of the Code of Practice for Official Statistics. They are awarded National Statistics status following an assessment by the Authority’s regulatory arm. The Authority considers whether the statistics meet the highest standards of Code compliance, including the value they add to public decisions and debate.
It is the Ministry of Justice’s responsibility to maintain compliance with the standards expected for National Statistics. If we become concerned about whether these statistics are still meeting the appropriate standards, we will discuss any concerns with the Authority promptly. National Statistics status can be removed at any point when the highest standards are not maintained, and reinstated when standards are restored.
Contact
Press enquiries should be directed to the Ministry of Justice or HMCTS press office:
Sebastian Walters (MoJ) - email: Sebastian.Walters@justice.gov.uk
Other enquiries about these statistics should be directed to the Data and Evidence as a Service division of the Ministry of Justice:
Rita Kumi-Ampofo or Matteo Chiesa - email: CAJS@justice.gov.uk
Next update: Thursday 12th May 2022
URL: www.gov.uk/government/collections/coroners-and-burials-statistics
© Crown copyright Produced by the Ministry of Justice
For any feedback on the layout or content of this publication or requests for alternative formats, please contact cajs@justice.gov.uk
-
1995 is the first year of annual data collection. ↩
-
https://www.judiciary.uk/wp-content/uploads/2020/03/Chief-Coroners-Office-Summary-of-the-Coronavirus-Act-2020-30.03.20.pdf ↩
-
Provisional figure based on ONS monthly death registration figures for 2020: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/datasets/monthlyfiguresondeathsregisteredbyareaofusualresidence ↩
-
These data only represent deaths in custody which were referred to a coroner and subsequently reported to the Ministry of Justice in the coroner’s annual return. ↩
-
For further detail please see Figure 13 of ‘Monitoring the Mental Health Act in 2019/20’, available at the following link: https://www.cqc.org.uk/sites/default/files/20201127_mhareport1920_report.pdf ↩
-
https://www.gov.uk/government/statistics/safety-in-custody-quarterly-update-to-september-2020 ↩
-
Schedule 1 to the Coroners and Justice Act 2009 states that the coroner should suspended an investigation in the event that criminal proceedings may or will take place. ↩
-
For years 2007-2013 this includes the previously used conclusions “Dependence on drugs” and “Non-dependent abuse on drugs” ↩
-
An analysis on unclassified conclusions can be found in the Coroners Statistics 2012 publication (Annex A), available at: www.gov.uk/government/statistics/coroners-statistics ↩
-
Note that Ceredigion has been excluded from this analysis due to a disproportionately low number of inquest conclusions (23) distorting the trend. ↩
-
Total percentages may not equal 100% due to rounding ↩
-
‘All other conclusions’ includes: Killed lawfully; Killed unlawfully; Lack of care or self-neglect; Stillborn and represent together less than 1% of the short-form conclusions recorded. ↩
-
The sex of the deceased is based on the ‘registrable particulars’ which coroners have a duty to record. Deaths certificates only gives two options, ‘male’ and ‘female’, and these will normally be completed by the registrar based on the information given to them by the informant. Under normal circumstances there would not be an investigation to ascertain whether what the informant says corresponds to biological sex or DNA of the deceased. ↩
-
Killed lawfully was excluded from above, as there was only 5 such inquest conclusions in 2020. ↩
-
ONS data is available online at: www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/datasets/deathsregisteredinenglandandwalesseriesdrreferencetables ↩
-
The ‘age not known’ category has been excluded from the chart due to small numbers (less than 0.5%). Totals may not add up to 100% due to rounding. ↩
-
A direct average of the time taken to process an inquest cannot be calculated from the summary data collected; an estimate has therefore been made instead. Please see the Guide to the Coroners statistics published alongside this report for the methodology used. ↩
-
Only deaths occurring within England and Wales are included in this estimation. ↩
-
The latest Department for Digital, Culture, Media & Sport (DCMS) figures are for 2019 and showed there were 1,307 finds reported in England and Wales, in line with the 1,061 treasure finds reported to Coroner Areas in 2019. These figures can be found at: https://www.gov.uk/government/statistics/statistical-release-for-reported-treasure-finds-2018-and-2019 ↩
-
This chart does not include reported findings under “Treasure Trove” ↩
-
As the ONS death registration figures are based on the area of usual residence whereas the coroners’ figures are based on the area where a person died, these figures should be used with caution. For example, the coroner office for the City of London shows a distorted figure above 100% due to the low level of residence and high level of commuters. ↩
-
Provisional figure based on ONS monthly death registration figures for 2020 ↩
-
City of London has been excluded from this analysis due to the percentage of deaths being greater than 100% - please see footnote 21 above for further information. So only 84 coroner areas have been included in this analysis. ↩