Guide to coroners statistics
Published 12 May 2022

© Crown copyright 2022
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/statistics/coroners-statistics-2021/guide-to-coroners-statistics
1. Introduction
This document accompanies the annual Coroners Statistics bulletin and provides a background overview of coroners, focusing on concepts and definitions published in Ministry of Justice statistics. It also covers policy background and changes, statistical publication revision policies, data sources, quality and dissemination.
The annual Coroners Statistics bulletin presents statistics on deaths reported to coroners, post-mortem examinations and inquests held, and conclusions recorded at inquests in England and Wales. All editions of the bulletin can be found here: www.gov.uk/government/collections/coroners-and-burials-statistics. The bulletin also includes statistics on investigations regarding finds reported to coroners.
The Coroners Statistics are published annually in May and cover statistics for each calendar year. There is no scheduled revisions policy for this publication.
The United Kingdom Statistics Authority has designated these statistics as National Statistics, in accordance with the Statistics and Registration Service Act 2007 and signifying compliance with the Code of Practice for Official Statistics.
Designation can be broadly interpreted to mean that the statistics:
- meet identified user needs;
- are well explained and readily accessible;
- are produced according to sound methods, and
- are managed impartially and objectively in the public interest.
Once statistics have been designated as National Statistics it is a statutory requirement that the Code of Practice shall continue to be observed.
The data analysed in this publication are based on annual returns from coroners. Thanks are due to coroners and their staff for their work in preparing these returns.
Information on the quality and consistency of the Coroners statistics can be found in the supporting document published alongside this bulletin.
1.1 About the statistics
This annual bulletin presents statistics of deaths reported to coroners in England and Wales in 2021. Information is provided on the number of deaths reported to coroners, post-mortem examinations and inquests held, and conclusions recorded at inquests. The data are collected via statistical returns completed by coroners.
Coroner services in England and Wales are governed by Part 1 of the Coroners and Justice Act 2009 (the 2009 Act), as well as the rules and regulations made under it. The 2009 Act came into force in July 2013, largely replacing the Coroners Act 1988[footnote 1].
The 2009 Act and its rules and regulations can be accessed via the links below:
www.legislation.gov.uk/ukpga/2009/25/contents www.legislation.gov.uk/2013?title=coroners
1.2 Covid-19 deaths and Coroner statistics
COVID-19 deaths are likely to be considered to be deaths from natural illness, and therefore will not of themselves be reported to coroners, apart from deaths which the coroner is under a statutory duty to investigate and hold an inquest (essentially deaths in custody or other forms of state detention). Inquests are usually opened in less than 20% of all deaths reported to coroners. In such cases, Coroners are required to provide us with the conclusions of these inquests. The list of short form inquest conclusions which the coroners can provide is set out in legislation and can be found in Table 7 of the coroners’ publication.
1.3 Summary of relevant Policy Changes due to Covid-19[footnote 2]
The government introduced emergency legislation, the Coronavirus Act 2020, in March 2020 to help various services cope with the effects of the pandemic.
Medical Certificates of Cause of Death (MCCD)
Any registered medical practitioner can sign an MCCD. This is even if the deceased was not attended during their last illness and not seen after death, provided that they are able to state the cause of death to the best of their knowledge and belief.
Once that MCCD reaches the registrar there are two possibilities depending on whether the deceased was seen before or after death. If a medical practitioner (who does not have to be the same medical practitioner who signed the MCCD) attended the deceased within 28 days before death (a new, longer timescale) or after death, then the registrar can register the death in the normal way. Second, if there was no attendance either within 28 days before death or after death, then the registrar would need to refer that to the coroner.
Medical practitioners’ duty to notify coroners
The Notification of Deaths Regulations 2019 provide that a registered medical practitioner must notify the coroner where:
-
it is reasonably believed that there is no attending medical practitioner required to sign the MCCD; or
-
it is reasonably believed that the attending medical practitioner required to sign the MCCD is not available to do so within a reasonable time of death.
The emergency legislation disapplies this requirement because, as set out above, the medical practitioner who signs the MCCD does not need to have attended. The duty on a medical practitioner to notify the coroner only applies during the emergency period where it is reasonably believed that there is no other medical practitioner who may sign the MCCD or that such a medical practitioner is not available within a reasonable time of the person’s death to do so.
COVID-19 as a notifiable death and jury inquests
COVID-19 was classified as a notifiable death under the Health Protection (Notification) Regulations 2010 in March 2020. Notifiable in this context means notifiable to the public health authorities, not notifiable to the coroner for the purpose of death investigation. Where the coroner has reason to suspect death was caused by COVID-19 and decides to open an inquest, section 30 of the Act removes the requirement for an inquest to be held with a jury.
1.4 Data and Methodology and related sources of information
-
Coroners in England and Wales have continued to provide the data which is the basis of these statistics and proactively engaged with statisticians to ensure this report was produced in a timely manner and to high standards.
-
The coronavirus pandemic has led to changes to the way coroners investigate deaths reported to them. They have had to be flexible and innovative in the way they conduct their inquests due to social distancing requirements.
-
Caution should be taken when making comparisons between regions of the coronial activities – post-mortems, inquests, timeliness, due to the restrictions based on the tier system around the country. Local authority set-up, resource, facilities and socio-economic make up mean this will not be comparing like with like.
-
Jury inquests have been particularly affected by social distancing requirements.
-
Pressure on NHS front line services has meant that clinicians have not always been available to attend inquests, causing delays, although many have attended remotely, a trend which is likely to continue after the pandemic.
1.5 Covid-19 deaths Signposting
Statistics relating specifically to Covid-19 related deaths can be found in the links below:
- The Office for National Statistics (ONS) publishes covid-19 related deaths here: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths
- The Ministry of Justice also publishes statistics relating to Covid-19 related State detention/prison deaths in the links below: https://www.gov.uk/government/statistics/hmpps-covid-19-statistics-december-2020 and https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/944911/deaths-offenders-community-2019-20-bulletin.pdf
1.6 Related statistics
All deaths in England and Wales must be registered with the Registrar of Births and Deaths. For those deaths where a coroner conducts an inquest, the death will be registered at the conclusion of the inquest, and the cause of death classified according to the conclusion recorded by the coroner. Statistics on registered deaths in England and Wales are published by the Office for National Statistics (ONS) in their series on mortality statistics. These can be accessed from the ONS website at: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths
The Ministry of Justice’s coroner statistics differ from ONS figures because they count two different, albeit related, events. The Ministry of Justice’s coroner statistics provide the number of deaths which are reported to coroners in England and Wales. These include deaths reported to coroners which occurred outside England and Wales. The ONS mortality statistics, based on death registrations, report the number of deaths registered in England and Wales in a particular year irrespective of whether a coroner has investigated the death. These do not include deaths that occurred outside England and Wales. Additionally, ONS counts deaths when they have been registered whilst coroners count deaths when they are reported.
The proportion of deaths which are reported to coroners has been estimated using death registration figures published by ONS. Estimates for 2021 have been calculated using ONS’ monthly provisional figures on death registrations, while percentages for 2020 and earlier years have been calculated using final annual death registration figures for the relevant year. There can be considerable delay between the date when the death occurred and when the death is registered. Deaths reported to a coroner would not be added to the deaths register until the coroner has concluded their investigation. Therefore it is advised that caution is used when using these figures.
This publication includes figures for deaths reported to coroners which occurred in state custody. Statistics on deaths in prison custody are also published by Her Majesty’s Prison and Probation Service (HMPPS), and are the official source of information on prison deaths. The HMPPS figures can be found in the ‘Safety in Custody’ bulletin, which is available at: https://www.gov.uk/government/collections/safety-in-custody-statistics
Differences between the two sets of figures are in part due to three main reasons. Firstly, there is a time lag in reporting processes. The figures for deaths in custody in this publication relate to those deaths when they have been reported to a coroner in the given year and then reported to MoJ, whereas for the HMPPS publication, deaths are recorded directly after they have occurred. Secondly, HMPPS figures include all deaths which have occurred in prision custoday including deaths which occurred whilst an offender has been Released on Temporary Licence (ROTL) for medical reasons. Deaths while on ROTL are classed as a separate category in the Coroners report, and cannot be broken down between ROTL for medical reasons and other types of ROTL. Finally, if the coroner is unaware that the death occurred in State Detention or classes it under another type of establishment, it may not be recorded as a death in State Detention by the coroner.
This publication also includes figures on deaths reported to coroners of individuals detained under the Mental Health Act (MHA) – similar statistics are published by the Care Quality Commission (CQC)[footnote 3]. Differences between the two sets of figures are likely to be due to a time lag in reporting processes: coroners are required to conduct an investigation within six months of the death being reported to them whilst the CQC receives reports of all deaths of individuals detained under the MHA in a particular year. In addition, the reporting time periods are different (the CQC report is financial year), and also not all deaths reported to the CQC are reported to a coroner.
This publication includes the number of deaths with a conclusion of suicide recorded at inquest - statistics on suicide deaths are also published by the ONS[footnote 4]. The ‘ONS Suicide Statistics UK’ series uses the national statistics’ definition of suicide: deaths given an underlying cause of intentional self-harm or an injury/poisoning of undetermined intent. In 2016, this definition has been modified to include deaths from intentional self-harm in 10- to 14-year-old children in addition to deaths from intentional self-harm and events of undetermined intent in people aged 15 and over.
1.7 Users of the statistics
The main users of these statistics are coroners and Ministers and officials in central government to assist in developing coroners’ policy and its subsequent monitoring. Other users include the Chief Coroner, local authorities (who are responsible for appointing and paying coroners as well as funding their services), other central government departments, and those non-governmental bodies, including various voluntary organisations, with an interest in coroners and inquests. The statistics are used to monitor the volume and types of cases dealt with by coroners in England and Wales each year.
1.8 Map of coroner areas in England and Wales, 2021
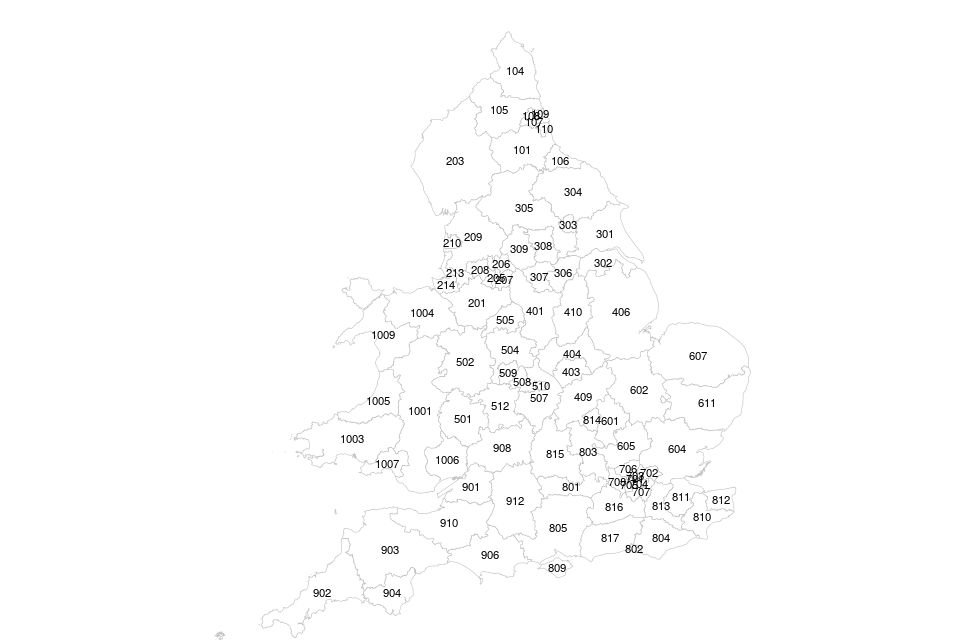
1.9 Key to coroner areas
| North East | East of England |
| 101 – County Durham and Darlington | 601 – Bedfordshire and Luton |
| 104 – North Northumberland | 602 – Cambridgeshire and Peterborough |
| 105 – South Northumberland | 604 – Essex |
| 106 – Teesside and Hartlepool | 605 – Hertfordshire |
| 107 – Gateshead and South Tyneside | 607 – Norfolk |
| 108 – Newcastle upon Tyne | 611 – Suffolk |
| 109 – North Tyneside | |
| 110 – Sunderland | London |
| 701 – City of London [not visible] | |
| North West | 702 – East London |
| 201 – Cheshire | 703 – Inner North London |
| 203 – Cumbria | 704 – Inner South London |
| 205 – Manchester City | 705 – Inner West London |
| 206 – Manchester North | 706 – North London |
| 207 – Manchester South | 707 – South London |
| 208 – Manchester West | 708 – West London |
| 209 – Lancashire and Blackburn with Darwen | |
| 210 – Blackpool and Fylde | South East |
| 213 – Sefton, Knowsley and St Helens | 801 – Berkshire |
| 214 – Liverpool and the Wirral | 802 – Brighton and Hove |
| 803 – Buckinghamshire | |
| Yorkshire and the Humber | 804 – East Sussex |
| 301 – East Riding and Hull | 805 – Hampshire, Portsmouth and Southampton |
| 302 – North Lincolnshire and Grimsby | 809 – Isle of Wight |
| 303 – York City | 810 – Central and South East Kent |
| 304 – North Yorkshire (Eastern) | 811 – Mid Kent and Medway |
| 305 – North Yorkshire (Western) | 812 – North East Kent |
| 306 – South Yorkshire (Eastern) | 813 – North West Kent |
| 307 – South Yorkshire (Western) | 814 – Milton Keynes |
| 308 – West Yorkshire (Eastern) | 815 – Oxfordshire |
| 309 – West Yorkshire (Western) | 816 – Surrey |
| 817 – West Sussex | |
| East Midlands | |
| 401 – Derby and Derbyshire | South West |
| 403 – Leicester City and South Leicestershire | 901 – Avon |
| 404 – Rutland and North Leicestershire | 902 – Cornwall and Isles of Scilly |
| 406 – Lincolnshire | 903 – Exeter and Greater Devon |
| 409 – Northamptonshire | 904 – Plymouth, Torbay and South Devon |
| 410 – Nottinghamshire | 906 – Dorset |
| 908 – Gloucestershire | |
| West Midlands | 910 – Somerset |
| 501 – Herefordshire | 912 – Wiltshire and Swindon |
| 502 – Shropshire, Telford and Wrekin | |
| 504 – Staffordshire South | Wales |
| 505 – Stoke-on-Trent and North Staffordshire | 1001 – South Wales Central |
| 507 – Warwickshire | 1003 – Carmarthenshire and Pembrokeshire |
| 508 – Birmingham and Solihull | 1004 – North Wales (East and Central) |
| 509 – Black Country | 1005 – Ceredigion |
| 510 – Coventry | 1006 – Gwent |
| 512 – Worcestershire | 1007 – Swansea and Neath Port Talbot |
| 1009 – North West Wales |
2. Structure and Functions of Coroners
Under the Coroners and Justice Act 2009 (“the 2009 Act”), each coroner area has one senior coroner, and one or more assistant coroners. A coroner area may also have an area coroner (who may function as a deputy to the senior coroner).
For a list of the current coroner areas and information on changes to these areas, please see Annex A of the Coroners statistics bulletin.
2.1 Chief Coroner
The 2009 Act created the post of Chief Coroner to provide judicial oversight of the coroner system and leadership, guidance and support to coroners. The Chief Coroner’s main statutory responsibilities are to:
- Approve all coroner appointments made by local authorities (along with the Lord Chancellor);
- Provide support, leadership and guidance for coroners in England and Wales;
- Set national standards for all coroners, including new inquest rules;
- Oversee the implementation of the new provisions of the Coroners and Justice Act 2009;
- Put in place suitable training arrangements for coroners and their staff;
- Keep a register of coroner investigations lasting more than 12 months and take steps to reduce unnecessary delays;
- Monitor investigations into the deaths of service personnel;
- Oversee transfers of cases between coroners and direct coroners to conduct investigations;
- Provide an annual report on the coroner system to the Lord Chancellor, to be laid before Parliament;
- Monitor the system where recommendations from inquests are reported to the appropriate authorities in order to prevent further deaths.
On 18 August 2016 the Lord Chief Justice, after consultation with the Lord Chancellor, appointed His Honour Judge Mark Lucraft QC as the second Chief Coroner of England and Wales. Judge Lucraft took up post on 1 October 2016, following the retirement of His Honour Judge Peter Thornton QC.
Further information on the Chief Coroner is available at: https://www.judiciary.uk/related-offices-and-bodies/office-chief-coroner/
2.2 Chief Coroner’s annual report
The Chief Coroner’s annual report to the Lord Chancellor is a statement on the coroner system for the previous calendar year. It must contain an assessment of consistency of standards between coroner areas; information about investigations that have taken over 12 months to complete; and a summary of reports to prevent future deaths and the responses to these. The annual report is published on the Corporate information section of the GOV.UK website[footnote 5].
Coroners are required to notify the Chief Coroner of any investigation that lasts more than a year and to notify the Chief Coroner of the date on which any such investigation was subsequently concluded.
2.3 Investigations
Under the 2009 Act, a coroner conducts an ‘investigation’ into a death (which may or may not include an inquest). Much of the coroner’s investigation takes place before any formal inquest hearing, and includes the coroner considering whether the duty to hold an inquest applies to an individual case.
In the majority of deaths reported to them, coroners’ investigations are concluded without an inquest being held. The coroner will have satisfied themselves, by means of a post-mortem examination or other investigation, on the physical cause of death and that the death was not one on which he or she is required by law to hold an inquest. A post-mortem examination may also take place in order to determine whether or not an investigation is necessary.
A coroner has a duty to investigate a death if:
- the coroner is made aware that the body is within that coroner’s area; and
- the coroner has reason to suspect that: a. the deceased died a violent or unnatural death; b. the cause of the death is unknown; or c. the deceased died while in custody or state detention.
The coroner must then establish who has died and how, when, and where they died.
A coroner’s inquest is held for all deaths in custody or state detention. An inquest with a jury is held where the deceased died while in custody or state detention and the death was violent or unnatural, or of unknown cause; where the death resulted from an act or omission of a police officer or member of a service police force in the purported execution of their duties; or where the death was caused by an accident, poisoning or disease which must be reported to a government department or inspector. Jury inquests are not required where the deceased died in custody or state detention but from natural causes.
Once any post-mortem examination (including any histology or toxicology) has concluded, the coroner must decide how to proceed. There are three main options:
-
The post-mortem examination reveals that the deceased died of natural causes and the coroner considers that it is not necessary to (investigate or) continue the investigation. There will be no inquest.
-
The post-mortem examination reveals that the deceased died of natural causes but the coroner considers that it is necessary to (investigate or) continue the investigation. The coroner must then hold an inquest.
-
After the post-mortem examination, the coroner (still) has reason to suspect that the deceased died a violent or unnatural death, or the cause of death is unknown, or the deceased died while in custody/state detention. The coroner must then hold an inquest.
2.4 Inquest conclusions
At the end of an inquest, the coroner (or jury if applicable) completes a form entitled ‘Record of an inquest’. This form documents the ‘conclusion’ of the coroner or jury as to who died and how, when, and where they died[footnote 6].
Conclusions are recorded in nearly all cases that proceed to inquest. The exceptions are inquests adjourned by the coroner if, for example, criminal proceedings take place. The inquest is usually not resumed because the relevant evidence has been heard elsewhere. Most inquests are held by a coroner sitting alone, without a jury, but as above under “Investigations”, a jury must be summoned in some circumstances, for example where the deceased died while in custody or state detention and the death was unnatural or violent or of unknown cause.
A conclusion consists of the ‘determination’, which states who died, and where, when and how they died; and ‘findings’ which allow the cause of death to be registered. The coroner or jury may use one of the following short form conclusions[footnote 7]:
- accident or misadventure
- alcohol/drug related
- industrial disease
- lawful killing
- unlawful killing
- natural causes
- open
- road traffic collision
- stillbirth
- suicide
Figure 1 shows the possible outcomes involved when a death is reported to a coroner.
2.5 Figure 1: Deaths reported to coroners, 2021
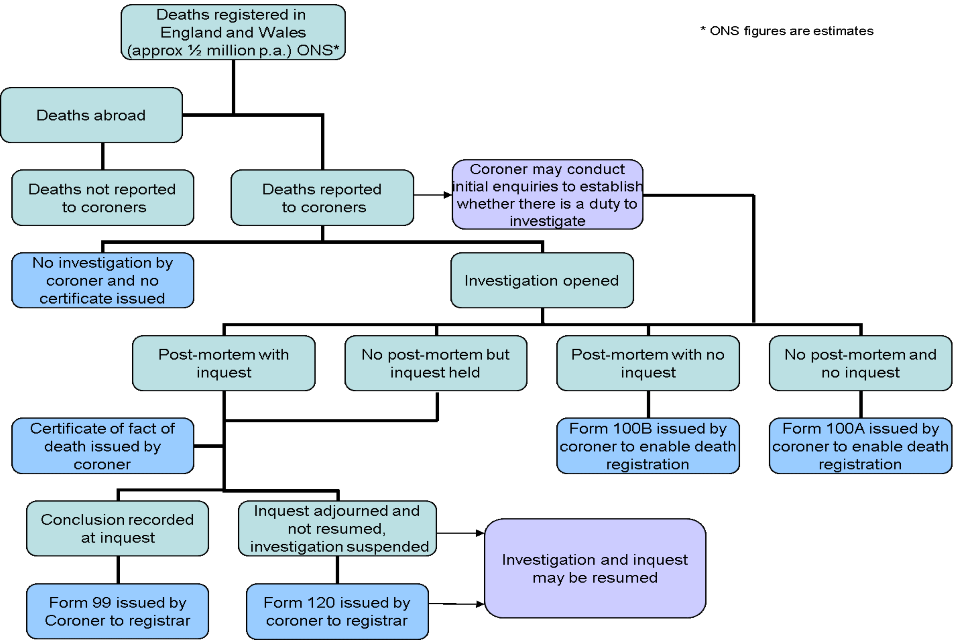
Conclusions recorded in 2021 may relate to deaths from 2021 or earlier years. It is not possible to follow the flow of cases through the system due to the way the data is collected.
2.6 Suspension of investigation / adjournment of inquest
Under Schedule 1 to the 2009 Act, a coroner must suspend an investigation (and if an inquest has been opened, adjourn that inquest) in the following circumstances:
- If asked to do so by a prosecuting authority because someone may be charged with a homicide or related offence involving the death of the deceased (paragraph 1);
- When criminal proceedings have been brought in connection with the death (paragraph 2) ;
- Where there is an inquiry under the Inquiries Act 2005 (paragraph 3);
- If it appears to the coroner that it would be appropriate to suspend an investigation or adjourn an inquest (paragraph 5).
2.7 Average time taken to complete an inquest
For the purpose of determining the average time taken to complete an inquest, the time taken to conduct an inquest is deemed to be from the day the death was reported to the coroner until either (a) the day the inquest is concluded by the delivery of a conclusion or (b) the day the coroner certifies that an adjourned inquest will not be resumed.
The average time for an inquest to be conducted is estimated in the following way: coroners are asked in their annual return to state how many inquests were concluded within certain time periods. There are five time bands, which are: within one month; 1-3 months; 3-6 months; 6-12 months; and over 12 months. All the inquests falling within a time-band are then assumed to have been completed at or near the mid-point of the various time-bands for the purposes of calculating the average. However, inquests within the “under one month” band are assumed to have taken 3 weeks for the purpose of this estimation, and those inquests taking over a year to conclude are deemed to have taken 18 months, although the time-band itself is open-ended. Numbers are then aggregated and the average figure (in weeks) calculated in the normal way.
Only deaths occurring within England and Wales are included in the calculation. Statistics are not collected on the time taken for inquests where the death occurred outside England and Wales. Deaths occurring abroad are often significantly delayed because of the difficulty, for example, of obtaining reports from other countries.
2.8 Treasure
In England and Wales a coroner also handles investigations regarding finds reported to them under the provisions of the Treasure Act 1996. The coroner will inquire into any treasure which is found in their area and establish the identity of the finder. By law, all treasure finds must be reported to the coroner within 14 days except where treasure finds occurred before 24 September 1997 when the find is dealt with under common law “Treasure Trove”. Such cases are extremely rare and the vast majority of cases fall under the Treasure Act 1996.
On 24 September 1997, the Treasure Act 1996 came into force and replaced the common law of Treasure Trove in England and Wales. The 1996 Act introduced new requirements for reporting and dealing with finds. Not all finds need be the subject of an inquest. For more information please see: www.legislation.gov.uk/ukpga/1996/24/contents
An annual report on the operation of the Treasure Act 1996 is published by the Department for Culture, Media and Sport. For more information please see: http://www.gov.uk/government/organisations/department-for-culture-media-sport/series/treasure-and-portable-antiquities-statistics
3. Policy Background and Changes
Prior to 1 June 2005, policy responsibility for coroners lay with the Home Office, but on that date it passed to the Department for Constitutional Affairs as part of machinery of government changes following the 2005 general election. Responsibility now lies with the Ministry of Justice, which was created on 9 May 2007.
3.1 Deprivation of Liberty Safeguards (DoLS)
Deprivation of Liberty Safeguards (DoLS) under the Mental Capacity Act 2005 were introduced in April 2009.
Deprivation of Liberty Safeguards are a procedure prescribed in law when it is necessary to deprive of their liberty a resident or patient who lacks capacity to consent to their care and treatment in order to keep them safe from harm. As a form of state detention any deaths that occur while a person is subject to DoLS were required to be reported to Coroners under section 1 of the 2009 Act.
The coroner data return for 2015 was modified to collect data on the number of deaths that occurred while the deceased was subject to DoLS, as a category within the state detention section of the data return. The 2015 Coroners Statistics bulletin then introduced separate figures on deaths that occurred while an individual was subject to a DoLS. Collection of this information coincided with a substantial increase in the overall number of DoLS authorisations issued in England and Wales following the Supreme Court judgment in the Cheshire West case[footnote 8]. This had a significant impact on a number of key statistics reported in 2017, as well as within the 2015 and 2016 publications.
As of 3 April 2017, a person subject to DoLS is no longer considered to be ‘otherwise in state detention’ for the purposes of the 2009 Act and therefore, any deaths on or after this date are no longer required to be reported to the coroner. The statistics reported in 2018 therefore no longer include DoLS cases. This change has reduced the number of deaths in state detention reported within the 2018 bulletin and had a corresponding effect on other statistics, for example inquests opened and inquest conclusions, in particular deaths by natural causes and the average time taken to complete an inquest.
4. Data Quality and Sources
The figures presented in the Coroner statistics are collected via statistical returns completed by coroners. For the calendar year 2021, all coroner area returns were received electronically. The process by which coroners provide their returns can vary according to the case management system they use. Many coroners use a system provided by an external contractor, while other coroners use alternative computer systems or in some cases a paper-based system. Although care is taken in completing, analysing and quality-assuring the data provided on the statistical returns, the figures are, of necessity, subject to possible inaccuracies inherent in any large-scale collection of this type. Every effort is made, however, to ensure that the figures presented in this publication are accurate and complete.
Returns are individually quality-assured and validated in a process that highlights inconsistencies between years, and between areas. Checks are made to ensure that each return is arithmetically correct, e.g. subtotals and overall totals are correctly summed. Unusual or outlying values found within returns are queried with the data supplier, to confirm whether these are correct, or that an error exists in the information provided which requires amendment.
Coroners are independent office-holders, and there is variation in the way each coroner’s area is structured and managed, and in the mechanisms they have in place for discharging their duties under the Coroners and Justice Act 2009. For example, differences between coroners as to which cases they consider constitute a substantive “reported death” (and are therefore reported in their statistics) where little or no action is required on their part and no post-mortem or inquest is held. As such, the statistics reflect those cases which each individual coroner considers to be a death reported to them, and the figures for different coroner areas can be compared on this basis.
5. Coroner Area Amalgamations
The following table summarises the coroner area amalgamations that have occurred in the previous ten years (since 2007). A list of all amalgamations since 2000 is included in the Coroners statistical tool published alongside this bulletin.
| Date Change Effective | Old areas | New area(s) | Nature of amalgamation |
|---|---|---|---|
| 06-Apr-07 | Norwich and Central Norfolk; King’s Lynn | Greater Norfolk | 2 into 1 |
| 01-May-07 | North East Cumbria; Western Cumbria; South Cumbria and Furness | North and West Cumbria; South and East Cumbria | 3 into 2 |
| 01-Apr-10 | Greater Norfolk; Great Yarmouth | Norfolk | 2 into 1 |
| 01-Jan-12 | Black Country; Wolverhampton | Black Country | 2 into 1 |
| 01-Apr-12 | West Lincolnshire; Spilsby and Louth | Central Lincolnshire | 2 into 1 |
| 01-Jun-12 | Boston and Spalding; Stamford | South Lincolnshire | 2 into 1 |
| 01-Jan-13 | Central North Wales; North East Wales | North Wales (East and Central) | 2 into 1 |
| 26-Jul-13 | Carmarthenshire; Pembrokeshire | Carmarthenshire and Pembrokeshire | 2 into 1 |
| 26-Jul-13 | Darlington and South Durham; North Durham | County Durham and Darlington | 2 into 1 |
| 26-Jul-13 | Derby and South Derbyshire; North Derbyshire | Derby and Derbyshire | 2 into 1 |
| 26-Jul-13 | Bournemouth, Poole and Eastern Dorset; Western Dorset | Dorset | 2 into 1 |
| 26-Jul-13 | Essex and Thurrock; Southend-on-Sea | Essex | 2 into 1 |
| 26-Jul-13 | Plymouth and South West Devon; Torbay and South Devon | Plymouth, Torbay and South Devon | 2 into 1 |
| 26-Jul-13 | Bridgend and Glamorgan Valleys; Powys | Powys, Bridgend and Glamorgan Valleys | 2 into 1 |
| 26-Jul-13 | Mid and North Shropshire; South Shropshire; Telford & Wrekin | Shropshire, Telford and Wrekin | 3 into 1 |
| 26-Jul-13 | Neath and Port Talbot; City and County of Swansea | Swansea and Neath Port Talbot | 2 into 1 |
| 01-Aug-14 | Queens Household | N/A | Abolished |
| 01-Jan-15 | North and West Cumbria, South and East Cumbria | Cumbria | 2 into 1 |
| 02-Apr-15 | Liverpool; The Wirral | Liverpool and Wirral | 2 into 1 |
| 01-Aug-15 | North and East Cambridgeshire; South and West Cambridgeshire; Peterborough | Cambridgeshire and Peterborough | 5 into 1 |
| 01-Apr-16 | East Somerset; West Somerset | Somerset | 2 into 1 |
| 01-Apr-16 | Cornwall; Isles of Scilly | Cornwall and Isles of Scilly | 2 into 1 |
| 01-Apr-16 | Powys, Bridgend and Glamorgan Valleys; Cardiff and Vale of Glamorgan | South Wales Central | 2 into 1 |
| 01-Apr-17 | Central Lincolnshire; South Lincolnshire | Lincolnshire | 2 into 1 |
| 01-Dec-17 | Blackburn, Hyndburn and Ribble Valley; Preston and West Lancashire; East Lancashire | Lancashire and Blackburn with Darwen | 3 into 1 |
| 01-Aug-18 | Teesside; Hartlepool | Teesside and Hartlepool | 2 into 1 |
| 01-Apr-20 | Central Hampshire; North East Hampshire; Portsmouth and South East Hampshire; Southampton and New Forest | Hampshire, Portsmouth and Southampton | 4 into 1 |
6. Useful Publications
Prior to the transfer of responsibility, the Home Office published statistical bulletins based on coroners’ annual returns, from 1980. The last four bulletins published in the Home Office Statistical Bulletin series were as follows: for year 2003, bulletin 9/04; for 2002, bulletin 6/03; for 2001, bulletin 3/02; and for year 2000, bulletin 7/01. These may be found at:
webarchive.nationalarchives.gov.uk/20110218135832/http://rds.homeoffice.gov.uk/rds/hosbarchive.html
Statistics on registered deaths in England and Wales are published by the Office for National Statistics (ONS). These can be accessed from the ONS website at:
www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths
ONS also published a statistical bulletin on the number of suicides in the UK, based on the registered deaths data, and can be found at the following website:
Statistics on deaths in prison custody are also published by her Majesty’s Prison and Probation Service (previously the National Offender Management Service, NOMS), accessible via the following link:
www.gov.uk/government/collections/safety-in-custody-statistics
An annual report on the operation of the Treasure Act 1996 is published by the Department for Culture, Media and Sport. For more information please see:
The Chief Coroner has issued a practical guide for coroners, accompanied by a set of standard letters and forms, for use in treasure cases in England and Wales, accessible via the Chief Coroner’s website:
www.judiciary.gov.uk/related-offices-and-bodies/office-chief-coroner/
The Care Quality Commission (CQC) publishes an annual report on mental health, which includes figures they have collected in relation to deaths while detained under the Mental Health Act:
www.cqc.org.uk/content/monitoring-mental-health-act-report
7. Glossary
The following definitions are intended as a guide to the meaning of terms in the Coroners Statistics bulletin concerning coroners and their work; more detailed definitions will be found in the Coroners and Justice Act 2009 (the 2009 Act) and the Treasure Act 1996 (see links below).
- www.legislation.gov.uk/ukpga/2009/25/contents
- www.legislation.gov.uk/2013?title=coroners
- www.legislation.gov.uk/ukpga/1996/24/contents
Chief Coroner
The judicial head of coroner services in England and Wales, responsible for setting national standards of service, training coroners and their officers and other staff and issuing guidance to them.
Coroner
A coroner is an independent judicial office holder, appointed by a local authority within the coroner area. Some coroners cover more than one local authority area. Coroners are invariably lawyers but coroners appointed before implementation of the 2009 Act may be doctors. They are responsible for the investigation of violent or unnatural deaths, deaths of unknown cause, and deaths in custody or state detention which are reported to them (see ‘Deaths reported to coroners’ section below).
Conclusion
This is the decision the coroner (or jury) reaches at the end of an inquest about how someone died. The conclusion is recorded on a ‘record of an inquest’ form which includes the legal ‘determination’ and ‘findings’. It may comprise one of the following ‘short form’ conclusions: accident or misadventure; alcohol/drug related; industrial disease; lawful/unlawful killing; natural causes; open; road traffic collision; stillbirth; or suicide. Conclusions are recorded in nearly all coroners’ inquests. The exceptions are those inquests adjourned, and not resumed, by the coroner under Schedule 1 to the 2009 Act because criminal proceedings have taken place.
Deaths reported to coroners
In England and Wales, all violent, unnatural or accidental deaths, deaths of unknown cause, and all deaths in custody and state detention, are reported to coroners.
Deprivation of Liberty Safeguard
The Mental Capacity Act 2005, as amended by the Mental Health Act 2007 provides for Deprivation of Liberty Safeguards (DoLS). DoLS were implemented in April 2009 and constitute the procedure prescribed in law when it is necessary to deprive of their liberty a resident or patient who lacks capacity to consent to their care and treatment in order to keep them safe from harm. Since 3 April 2017 such arrangements have been excluded from the meaning of state detention for the purposes of coroner law.
Determination
This is the decision (reached by coroner or jury as appropriate) about the identity of the deceased and how, when and where he or she came by his or her death.
Findings
These are the details about a death that the coroner establishes to enable the death to be registered under the Births and Deaths Registration Act 1953.
Inquest
This is a public hearing held by a coroner in order to establish who has died, and how, when and where they came by their death. It forms part of the coroner’s investigation. An inquest does not establish any matter of criminal or civil liability and does not seek to blame anyone or apportion blame between people or organisations. If it is not possible to find out the cause of death from the post-mortem examination, the death is found to be unnatural (or occurred in state detention) or the coroner considers there is a good reason to continue the investigation, the coroner must hold an inquest to be able to finish his or her investigation. The inquest may be held with a jury, depending on the circumstances of the death.
Investigation
The coroner’s investigation is the process by which the coroner establishes who has died, and how, when, and where they died. The coroner may decide, as part of the investigation, to hold an inquest. The coroner has a duty under the 2009 Act to investigate a death if:
- the coroner is made aware that the body is within that coroner’s area, and
-
the coroner has reason to suspect that:
a. the deceased died a violent or unnatural death;
b. the cause of the death is unknown; or
c. the deceased died while in custody or state detention.
Juries
Nearly all inquests are held by a coroner sitting alone, without a jury. A jury must be summoned if the senior coroner has reason to suspect:
a. that the deceased died while in custody or otherwise in state detention, and that either the death was violent or unnatural, or the cause of death is unknown;
b. that the death resulted from an act or omission of a police officer, or a member of a service police force in the purported execution of his or her duty;
c. that the death was caused by a notifiable accident, poisoning or disease (i.e. under certain statutory reporting obligations under the Health and Safety Act 1974 or any other Act, and in certain other circumstances, especially where there may be a continuing or recurring danger to the public).
Juries in coroner inquests comprise of between seven and eleven members.
Killed lawfully
This conclusion may be recorded, for example, due to termination of a pregnancy, lawful shooting by a police officer, or a death resulting from self-defence.
Narrative conclusion
This is where the coroner makes a brief and factual statement at the conclusion of the inquest rather than returning a short-form conclusion.
Non-inquest cases
This is where the coroner’s investigation is concluded without an inquest being held.
Open conclusion
This may be recorded by the coroner if there is insufficient evidence to enable the coroner or the jury to reach one of the other conclusions
Out of England Order
To take a body of a deceased person out of England and Wales, notice must be given to the coroner within whose area the body is lying. This notice allows the coroner to consider whether an investigation is necessary. When the coroner gives permission for the removal of the body an Out of England order is issued.
Post-mortem examination
This is a detailed examination of a body after death to establish the medical cause of death. A coroner’s post-mortem examination is carried out by a suitable medical practitioner such as a pathologist (a doctor who specialises in medical diagnosis by examining body organs, tissues and fluids) of the coroner’s choice. A coroner may commission a post-mortem examination, whether or not an inquest is held, particularly if the cause of death is not clear. In many cases a post-mortem examination is conducted in order to determine whether or not an inquest is necessary.
Registered deaths
All deaths in England and Wales must be registered with the Registrar of Births and Deaths. The term ‘registered deaths’ in the Coroners Statistics bulletin refers to deaths registered within a specific time period (in this case, calendar years).
Statistics on registered deaths in England and Wales are published by the Office for National Statistics (ONS) in their series on mortality statistics. At the time of the Coroners Statistics 2021 publication, final figures had not been published for the number of registered deaths in 2021, but a provisional figure has been derived from the monthly registration figures which are published by ONS at regular intervals.
Suspensions under Schedule 1 to the 2009 Act
Under Schedule 1 to the 2009 Act a coroner must suspend an investigation (and if an inquest has been opened, adjourn that inquest) in the following circumstances:
- If asked to do so by a prosecuting authority because someone may be charged with a homicide or related offence involving the death of the deceased (paragraph 1);
- When criminal proceedings have been brought in connection with the death (paragraph 2);
- Where there is an inquiry under the Inquiries Act 2005 (paragraph 3,);
- If it appears to the coroner that it would be appropriate to do so (paragraph 5).
Timeliness of inquests
For the purpose of determining the timeliness of inquests, the time taken to conduct an inquest is deemed to be from the day the death was reported to the coroner until either (a) the day the inquest is concluded by recording a conclusion or (b) the day the coroner certifies that an adjourned inquest will not be resumed.
The average time for an inquest to be conducted is estimated in the following way: coroners are asked in their annual return to state how many inquests were concluded within certain time periods. There are five time bands: within one month; 1-3 months; 3-6 months; 6-12 months; and over 12 months. All the inquests falling within a time-band are then assumed to have been completed at or near the mid-point of the various time-bands for the purposes of calculating the average, although inquests within the “under one month” band are assumed to have taken 3 weeks for this purpose of this estimation, and inquests taking over a year to conclude are deemed to have taken 18 months, although the time-band itself is open-ended. Numbers are then aggregated and the average figure (in weeks) calculated in the normal way.
Note: only deaths occurring within England and Wales are included in the calculation. Statistics are not collected on the time taken for inquests where the death occurred outside England and Wales. Deaths occurring abroad are often significantly delayed because of the difficulty, for example, of obtaining reports from other countries.
Treasure and treasure trove
Treasure is defined as:
-
Any object at least 300 years old which:
a. Is not a coin but has metallic content of which at least 10% by weight is precious metal (i.e. gold or silver); and
b. Is one of at least 2 coins in the same find which are at least 300 years old and have that percentage of precious metal; or
c. Is one of at least 10 coins in the same find which are at least 300 years old
-
Any object at least 200 years old which the Secretary of State considers to be of outstanding historical, archaeological or cultural importance.
Treasure Trove relates to treasure finds made before commencement of the Treasure Act 1996 on 24 September 1997.
Coroners have jurisdiction to inquire into any treasure which is found in their area and to establish who the finder is.
-
The Coroners Act 1988 was repealed in July 2013 with the exceptions of section 13 (application for a fresh coroner investigation or inquest) and 4A (8) (a coroner in Wales being regarded as a coroner for the whole of Wales). ↩
-
https://www.judiciary.uk/wp-content/uploads/2020/03/Chief-Coroners-Office-Summary-of-the-Coronavirus-Act-2020-30.03.20.pdf ↩
-
The Care Quality Commission (CQC) annual report on Monitoring the Mental Health Act can be found here: http://www.cqc.org.uk/content/monitoring-mental-health-act-report. ↩
-
For more on ONS Suicide please visit: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/suicidesintheunitedkingdom/previousReleases ↩
-
https://www.gov.uk/government/publications/chief-coroners-combined-annual-report-2018-to-2019-and-2019-to-2020 ↩
-
The 1988 Act term ‘verdict’ was replaced by the 2009 Act term ‘conclusion’. ↩
-
‘Alcohol/drug related’ and ‘road traffic collision’ are short form inquest conclusions under the 2009 Act, which came into effect from July 2013. ↩
-
The Supreme Court’s 2014 judgment in the cases of P v Cheshire West and Chester Council and P&O v Surrey County Council (Cheshire West) clarified the circumstances in which a DoLS is likely to be required and made it clear that many more circumstances amounted to a deprivation of liberty by the state. The Supreme Court decided that deprivation of liberty arose when the person concerned ‘was under continuous supervision control and was not free to leave’ and that the deprivation was the responsibility of the state. It did not matter that the patient in hospital or the resident of a care home was content or compliant or voiced no objection if in fact they did not have capacity to consent to the arrangements. ↩