Bed rails: management and safe use
How to manage and use bed rails safely.
This web page features the most up-to-date guidance. It replaces previous guidance on the same topic.
You can download a PDF version of .
1. Summary
The MHRA is the regulator of medicines, medical devices and blood components for transfusion in the UK, a role which includes overseeing investigations into adverse events and promoting the safe use of devices in the UK.
At the MHRA we continue to receive reports of incidents relating to bed rails and associated equipment. These incidents are concerning as some have led to patient harm or death, primarily from entrapment.
This document aims to set out best practice in the provision, prescription, use, maintenance and fitting of bed rails.
We have updated this publication to reflect changes in devices and practices, as well as information gained from the investigation of adverse incidents.
The government has extended acceptance of CE marked devices in Great Britain. For more details, see the implementation update on work towards a strengthened future medical devices regime.
Who this guidance is for
This guidance is for all users, carers and staff with responsibility for the provision, prescription, use, maintenance and fitting of bed rails. This includes:
- medical device safety officers (MDSOs) for onward distribution
- medical device trainers
- care home managers and staff
- carers in the community and care-at-home staff
- community equipment stores (CES) and loan store managers
- health and safety or risk managers
- hospice managers and staff
- maintenance staff
- nurses in hospitals and the community
- occupational therapists
- physiotherapists
- those responsible for purchasing beds and bed rails
Scope
This guidance identifies areas for safe practices, so that policies and procedures can be reviewed and put in place. This includes:
- risk management
- safe use of these devices
- roles and responsibilities
- meeting legal requirements
- training
- planned preventative maintenance
It also identifies areas of good practice such as:
- assessing if a bed rail is necessary and appropriate
- the need for good communication between bed occupant and carers or staff
- checking compatibility of the bed rail, bed, mattress and the needs of the bed occupant
- taking into account the use environment and possible interaction with any other equipment, accessories or devices present in that environment as part of the risk assessment
- correct fitting and positioning of the bed rails initially and after each period of use
- reassessing the changing care needs of the bed occupant
This guidance is not intended to replace clinical decision making.
2. Introduction
Bed rails are used extensively in hospitals, care homes and people’s own homes to reduce the risk of bed occupants falling out of bed and injuring themselves. For the purpose of this document the term bed rail will be adopted, although other names are often used, for example, bed side rails, side rails, cot sides, and safety sides.
At the MHRA we continue to receive reports of adverse incidents involving these devices. The most serious of these have led to injury due to falls and death by asphyxiation as a result of entrapment of the head, neck or chest.
From 1 January 2018 to 31 December 2022, we received 18 reports of deaths related to bed rails and associated equipment, and 54 reports of serious injuries.
Most incidents occurred in community care settings, particularly in nursing homes or the patient’s own home. Adequate and appropriate risk management should be carried out to prevent the occurrence of such incidents. Healthcare professionals or competent persons should carefully consider the benefits and risks of bed rails before they are used for a patient.
We have also received reports of entrapment in hospitals (acute settings) with side rails on trolleys and stretchers. This guidance should also be followed in acute settings where bed rails are used with trolleys, stretchers and emergency department beds, particularly if the patient is unattended.
Chest or neck entrapment in bed rails is listed (number 11) as a ‘Never Event’ according to the NHS in 2018. ‘Never Events’ footnote 1 are ”serious, largely preventable patient safety incidents that should not occur if the available preventative measures have been implemented by healthcare providers”.
Bed rails
In general, manufacturers intend their bed rails to be used to prevent or reduce the risk of bed occupants falling and sustaining injury. They are not designed or intended to limit the freedom of people by preventing them from intentionally leaving their beds. In addition, they are not intended to restrain people whose condition disposes them to erratic, repetitive or violent movement.
Use of bed rails in these ways can increase the risk of falling. In some cases, the patient may attempt to climb over the bed rail, leading to the potential to fall from a height. Erratic, repetitive or violent movements may also cause the bed rails to break, leading to an increased risk of falling or injury from the broken rail.
To prevent inappropriate or unintended restraint through the use of bed rails, there must be a robust assessment of whether the use of the bed rail will prevent the person from moving freely or make the person feel restricted from moving freely. In all cases the least restrictive options should be explored. The NHS guidance on the Mental Capacity Act footnote 2 has more information on this.
Bed rails must be UKCA, CE or CE UKNI marked as medical devices, to show they meet the requirements of the UK Medical Devices Regulations 2002 (as amended) footnote 3, in combination with, or as an accessory to, the bed if their intended use meets the definition of a medical device.
Not all beds, bed rails or associated equipment will be classed as medical devices. This will depend on the intended use described by the manufacturer and without a clear medical purpose the definition of a medical device may not be met. In these cases, the product should still meet the requirements imposed by general consumer protection legislation which is outside the scope of this guidance.
Types of bed rail
Rigid bed rails can be classified into two basic types: integral and third party.
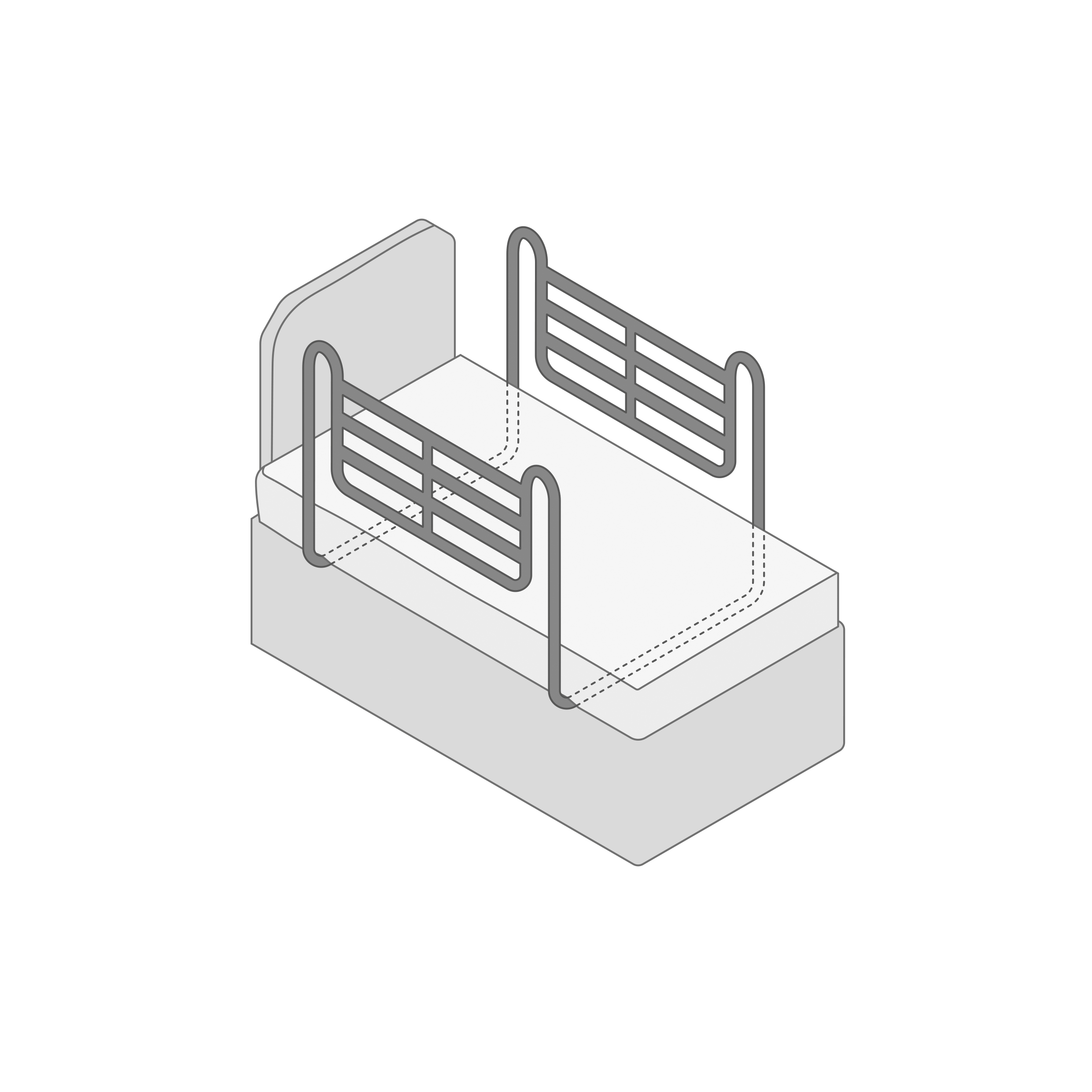
Integral types are incorporated into the bed design and supplied with it or are offered as an optional accessory by the bed manufacturer, to be fitted later. Examples can include hospital/profiling/adjusting beds – see Figure 1 and 3.
Figure 1 - Example of an integral bed rail
{kind=link}
Third-party types are not specific to any particular model of bed. They may be intended to fit a wide range of domestic beds, including divan or metal framed beds from different suppliers. They tend to be fitted under mattresses and use the weight of the mattress to remain in place. See Figure 2.
Figure 2 - Example of a 3rd-party bed rail
{kind=link}
Integral type bed rails have been involved in far fewer adverse incidents than third-party types. Usually this is because risks associated with installation and compatibility are reduced, as correct gaps are designed into the bed. Bed rails should meet recognised product standards that include acceptable gaps and dimensions when fitted to the bed (See Legislation and Standards).
Figure 3 - Example of a community-style bed with full-length integrated bed rails.
{kind=link}
Bed grab handles
Bed rails, which fit under the mattress or clamp to the bed frame, should not be confused with bed grab handles (also known as bed sticks or bed levers), which are designed to aid mobility for the person in bed and to help them transfer to and from bed, rather than to prevent falls from bed.
Bed grab handles can pose the same hazards to users as bed rails, including entrapment. Their use should be carefully considered, risk assessed and documented. We have received reports of deaths relating to entrapment in bed grab handles.
Bed grab handles, which come in a variety of sizes and designs (Figure 4), are not designed to prevent patients falling from their bed. They should not be used as an alternative to bed rails.
Some bed rails can also be used as bed grab handles as they have undergone testing to ensure they can support the additional loads from use in this way. However, not all bed rails can be used as bed grab handles. If the risk assessment demonstrates that the bed occupant requires bed rails to prevent falls and also bed grab handles to aid mobility, then appropriate bed rails which can support the weight of the bed occupant when being used to aid mobility should be used. If the bed rail is not appropriate for use as a bed grab handle, this could result in the bed rail breaking.
Figure 4 - Example of a bed grab handle
{kind=link}
Other devices
The bed occupant’s care needs should always be taken into consideration in a decision to use a bed rail as well as the environment it is used in and other equipment that is or may be present.
Bed rails are often used at the same time as other medical devices or equipment, for example, with pressure-relieving surfaces (either passive, for example air pocket mattresses, or active, for example air flow mattresses), monitoring equipment or other systems depending on the bed occupant’s needs. These devices can affect gaps and need to be accounted for in the risk assessment.
Hazard and areas of risk
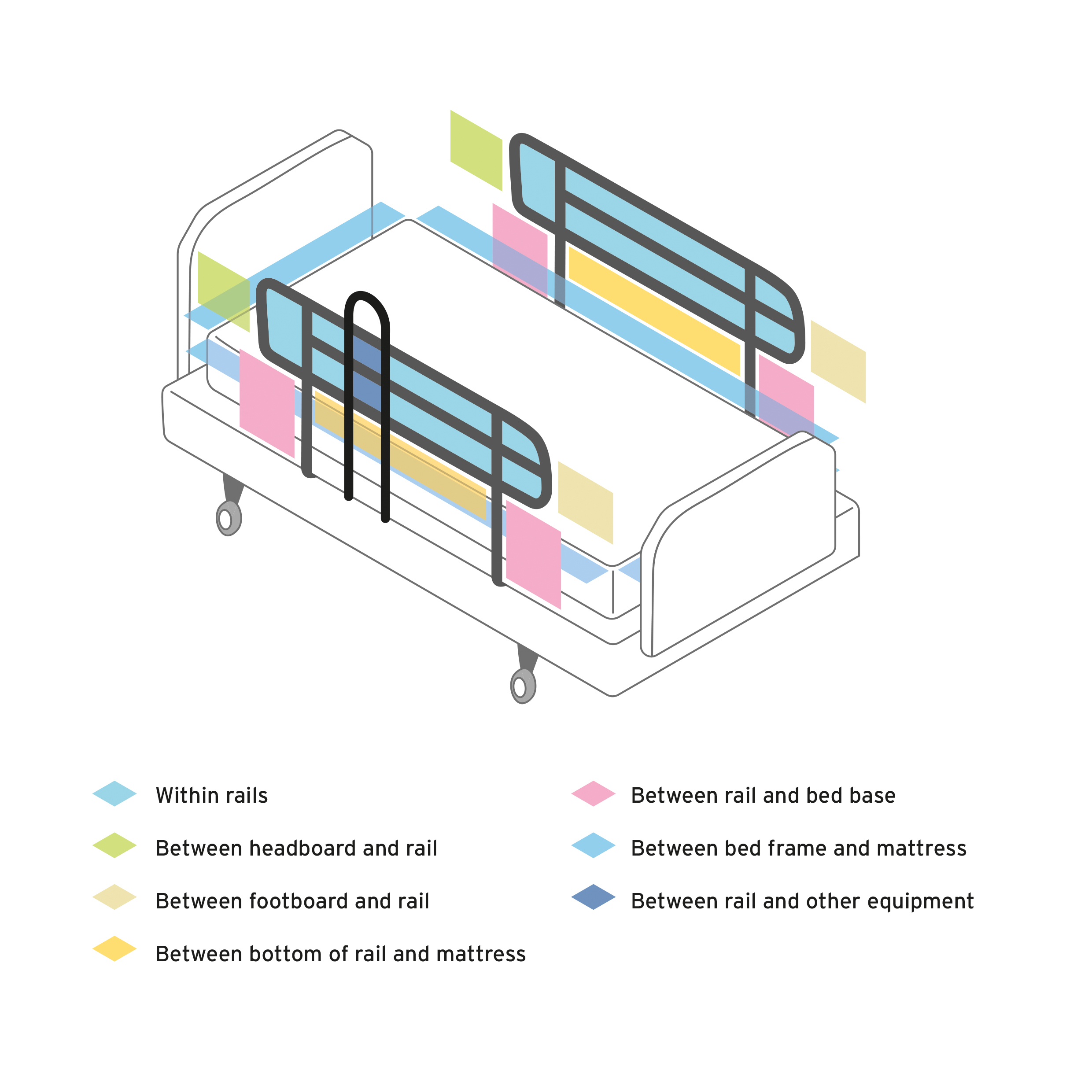
The use of bed rails is associated with several direct and indirect risks to bed occupants, as well as the possible benefits from reducing the risk of falls. Direct hazards include entrapment and entanglement, either within gaps in the rails themselves, between the rails and the mattress or between the rails and the bed frame. In the most serious cases, this has led to asphyxiation and death of bed occupants. Bed occupants may have trapped their head between rails or been unable to free themselves from a position and suffered postural asphyxiation. Severe limb damage has also been reported in cases where someone has become entangled in bed rails. Figure 5 shows the main areas of the bed-bed rail system where entrapment may occur.
Figure 5 - Bed rail entrapment areas. Split rails have additional entrapment risk areas
{kind=link}
Indirect hazards are also present. Cases have been reported where bed occupants have been confused or disoriented and have tried to get out of the bed by climbing over the bed rails. Occupants have then fallen from a greater height than would otherwise be the case, increasing the severity of injury.
3. Risk management and use assessment
Risk management
When medical devices (bed rails, mattresses and others) are prescribed, issued or used, it is essential that any risks are balanced against the anticipated benefits to the user. The process of understanding, evaluating, addressing and recording these risks is known as risk management.
Where manufacturers cannot remove or reduce risks during the design and manufacturing processes, subsequent warnings of any remaining risk should be clearly displayed in the user instructions and product markings. These must constitute acceptable risks when weighed against the benefits to the bed occupant.
Any such warnings or limitations to use, including the necessary maintenance schedules throughout its intended life, should be:
-
considered both during procurement and by prescribers
-
passed on to all users and carers of the equipment
Steps should also be taken to ensure that they are understood and complied with.
Users, carers and prescribers need to follow the manufacturer’s instructions for use and any warnings about associated risks. The equipment should only be used and maintained in line with the manufacturer’s instructions for use.
Risk assessment
There are many bed rails on the market, with a variety of fitting and operation methods.
The possible combinations of bed rails, beds and mattresses (and other equipment in the environment), together with the individual needs of the bed occupant, means that a robust and person-centred risk assessment of the equipment, environment and the person is necessary to avoid serious incidents.
Risk assessments should be carried out before the initial prescription of bed rails.
Additionally, risk assessments should be reviewed and recorded after each significant change in the bed occupant’s condition or needs. Replacement of any part of the equipment combination, including temporary removal for cleaning or maintenance, and permanent replacement, should be reviewed during its period of use, according to local policy. More frequent reviews will be required for children who are growing or patients who are losing weight, for example.
It is highly unlikely that one type of bed and bed rail will be suitable for a wide range of users with different physical sizes and needs.
Some questions to consider during a risk assessment to determine if the overall risks of using bed rails outweigh the possible benefits include:
- how likely is it that the bed occupant would fall from their bed?
- if likely, are bed rails an appropriate solution or could the risk of falling from the bed be reduced by means other than bed rails (see Alternatives to rigid bed rails)?
- could the use of a bed rail increase risks to the occupant’s physical or clinical condition (see Case study 1)?
- how likely is it that the bed occupant may attempt to climb over the bed rails?
- has the bed occupant used bed rails before?
- do they have a history of falling from bed, or conversely of climbing over bed rails?
- what are the bed occupant’s views on using bed rails?
- what configuration of bed, mattress and rail system is being used?
- are other devices being used, which could increase risk, such as lateral turning devices?
Our adverse incident investigations have shown that the physical or clinical condition of bed occupants means that some are at greater risk of entrapment in bed rails. Those at greater risk could include adults, particularly older adults, or children with:
- communication problems
- confusion, agitation or delirium
- learning disabilities
- dementia
- repetitive or involuntary movements
- larger or smaller than average body size (which may change entrapment risks)
- impaired or restricted mobility
- variable levels of consciousness, or those under sedation
Risk assessments should account for any characteristics which might put the bed user at greater risk from use of bed rails.
Every effort should be made to explain to the person being cared for why their bed has or is likely to have bed rails fitted. The potential risks, as identified by their individual risk assessment should also be explained to the person, as appropriate, as well as measures to reduce their risk of falls and entrapment.
The decision to use bed rails should be made with the person’s consent, wherever possible, remembering that they may have a different perception of risk to the prescriber and therefore disagree on whether the risks are acceptable or not. The reasoning for the decision to prescribe bed rails should be effectively communicated and recorded, including to the carers or family members when this is appropriate.
It is also essential to discuss with the bed occupant, and their carers and family members where appropriate, that they should consult with the prescriber if they are planning on purchasing additional equipment privately. Additional equipment can introduce new risks or increase existing risks (see Case Study 6).
Case study 1: inappropriate prescription leading to fall
A bed occupant died after climbing over the bed rails and falling. The user touched the bed position control and raised the bed to its maximum height. They then tried to get out of the bed by climbing over the rail, only to fall and suffer a broken neck. The additional height of the bed rail likely increased the severity of the injury.
Advice
If bed users are known to be in a confused state, then bed rails may serve to increase the overall risk of injury. A risk assessment could have identified the hazard of leaving bed controls accessible and the potential for an increased fall height and of the occupant having sufficient mobility to climb over the bed rails.
We provide an example of a risk assessment checklist, produced using feedback from prescribers of bed rails and the findings of adverse incident investigations in Appendix 1.
Note that the example checklist should not be adopted or used without adequate consideration of a specific bed occupant’s needs and local policies.
The checklist should be used in conjunction with the guidance in this document, together with the judgement of the nurse, therapist, care staff, bed occupant and unpaid carer or family member involved.
Measures to mitigate the risks associated with bed rails
Measures to mitigate the risks associated with bed rails should be considered as part of the initial risk assessment. These measures include:
- ‘netting’ or mesh bed sides
- inflatable bed sides and bumpers (see section 6)
- ultra ‘low height’ beds that minimise the risk of fall injuries
- positional wedges to reduce movement across the bed
- alarm systems to alert carers that a person has moved from their normal position or wants to get out of bed
- fall mats that can be placed beside the bed to reduce the severity of the impact if the bed occupant does fall
Each of these options may act to introduce different hazards even as they reduce the risk of bed fall injury or the risk from bed rails, and so should be assessed and managed appropriately.
4. Purchase and selection
Purchase
Adjustable or profiling beds usually have compatible integral type bed rails available from the manufacturer; these are preferable to other systems that may not fit as well. In all cases it is essential that the selection process follows a risk assessment considering the needs of the bed occupant and the use environment.
Third-party bed rails require particularly careful selection.
If bed rails are being purchased for stock, general factors can be considered at the purchase stage:
- the types of bed they are likely to be used on; specific models or range
- whether their dimensions meet recognised product standards
Risk assessments should be carried out before the initial use of bed rails. Additionally, risk assessments should be reviewed and recorded after each significant change in the bed occupant’s condition or needs. Replacement of any part of the equipment combination, including temporary removal for cleaning or maintenance, and permanent replacement should be reviewed during its period of use, according to local policy. An example of a risk assessment checklist is included in Appendix 1.
We suggest manufacturer’s instructions for use contain information on the selection of the mattress, including dimensions and other characteristics, to reduce the risk of entrapment. They should also contain information on compatibility with other equipment and whether they are suitable for children or small adults. Ensure that the bed, mattress and bed rails in combination are compatible and do not have gaps that are not permitted by device standards. This could lead to entrapment.
For more information on gaps permitted by device standards, see Appendix 2 and Appendix 3. Note that the values expressed in standards are primarily intended for the manufacturers of medical devices.
Selection
In all cases it is essential that the selection process follows a risk assessment considering the needs of the bed occupant.
In community care environments it is common for beds and bed rails to have been acquired from different sources. Often bed rails from unknown sources in use and in many cases, they have been found to be unsuitable or unfit for purpose.
Bed rails for divan beds (domestic) are mainly of the third-party type, not tailored for one specific bed or mattress length and width, or a specific mattress density.
Case study 2: unsuitable combination of a bed and a bed rail
A bed rail intended for use on a domestic divan bed was used on a hospital type bed. This produced a large gap between the bottom of the bed rail and the bed when the mattress was compressed.
A child slipped feet first between the bed rail and the bed. The gap was not large enough for the child to pass completely through and the child was trapped at chest level and died from postural asphyxiation.
Image illustrating case study 2
{kind=link}
Advice
When supplied, the suitability of the installation should be checked, including following the manufacturer’s instructions for use regarding compatibility with other devices.
5. Correct fitting
Fitting and use
It is essential that all bed rails can be fitted correctly to an appropriate bed base allowing safe use. Some aspects to consider at the start of the fitting process are:
- can the bed rails be fitted to the bed correctly following the manufacturer’s instructions?
- do staff understand how to fit them properly?
- are mounting clamps, if present, used in the correct orientation and in good condition?
- is there an inappropriate gap between the lower bar of the bed rail and the top of the mattress or does the mattress compress easily at its edge which could cause entrapment?
- is there a gap between the bed rail and the side of the mattress, headboard or footboard that could trap the bed occupant’s head or body?
- is the bed rail secure and robust – could it move away from the side of bed and mattress in use, creating an entrapment or fall hazard?
- do the dimensions and overall height of the mattress(es) compromise the effectiveness of the bed rail for the particular occupant – are extra height bed rails needed?
Case study 3: user entrapment in inappropriate gaps
Entrapment can happen between the end of the bed rail and the headboard if the gap is inappropriate. Avoid gaps over 60mm, which could be enough to cause neck entrapment.
Entrapment can also occur in the space between a poorly fitting mattress and side of the bed rail or bed rail that does not fit the bed base snugly enough.
The compressible nature of the edge of most mattresses can contribute towards the entrapment risk.
Image illustrating case study 3
{kind=link}
Advice
Assess the possible gaps between rails and other equipment, particularly in the high-risk areas shown in Figure 5 during the rail fitting process.
What to avoid
From our investigations we have identified a number of potential risk areas that, if they had been avoided during the selection process, may have reduced the likelihood of adverse incidents occurring. For example, avoid:
- gaps of over 60 mm between the end of the bed rail and the headboard which could be enough to cause neck entrapment
- gaps over 120 mm from any accessible opening between the bed rail and the mattress platform
- filling any gaps using blankets, bedding or pillows, as these can be compressed and may increase the risk of entrapment
- using bed rails designed for a divan bed on a wooden or metal bedstead, this can create gaps which may entrap the occupant
- using unsecure fittings or designs which permit the bed rail to move away from the side of the bed or mattress, creating an entrapment hazard
- using only one side of a pair of bed rails when the other side is against a wall if this is not specifically permitted by the manufacturer – the single rail may be insecure and move (some manufacturers supply a mattress retainer for use with single sided bed rails which reduces this risk)
- mattress combinations whose additional height lessens the effectiveness of the bed rail and may permit the occupant to roll over the top - extra height bed rails are available if mattress overlays are to be used
- mattress and bed rail combinations where the mattress edge easily compresses, introducing a vertical gap between the mattress and the bed rail
The length, width and height of the mattress should be checked to ensure that these dimensions are within the limits specified by the bed manufacturer and do not introduce gaps that could increase the risk of entrapment. If the mattress is not the right size, the bed rails may not fit properly and create entrapment gaps. Some manufacturers may also specify the density of static mattresses.
Training
Suitable evaluation of a bed occupant before providing a bed rail is a skill. Organisations responsible for the prescription, provision, installation and maintenance of rails should ensure that those carrying out these tasks are appropriately trained in the competent use of these devices. They should have the skills needed:
- to properly conduct a risk assessment in accordance with local policy
- to understand the risks posed by this equipment
Organisations should develop processes to ensure that staff are appropriately trained and that risk assessments are carried out and recorded to a suitable standard.
Those responsible should be aware of how and when to arrange for maintenance and to report faults. Depending on the environment, this could include care staff, family members or the bed occupant themselves.
6. Special considerations
Use in the community
Most reported injuries relating to bed rails are now from incidents that take place in community settings, both in care homes and in people’s own homes.
Use of bed rails in the community comes with additional challenges. There may be greater variability in available equipment, and it can be more difficult to maintain equipment appropriately than in hospitals. Those responsible for day-to-day care may be less aware of the serious risk that can be present with improper use of bed rails. Any subsequent changes in the bed occupant’s health and wellbeing (such as cognitive decline, deterioration in eyesight or weight changes) could increase the risk of inappropriate bed rail use.
Wherever bed rails are used to reduce fall risk, a risk assessment should be undertaken, and the rails should be regularly assessed for suitability and correct function. Carers and the bed occupant, where possible, should be aware of the risks, should have access to the device instructions and should know when to carry out or request reassessment of the needs of the bed occupant. They should also have details for a designated contact if they are concerned about a change or increase in risk.
Case study 4: mattress too light to keep bed rail in correct position
Some designs rely on the weight of the divan or standard mattress to keep the bed rails in position. A lighter mattress can allow the rails to move away from the side of the bed, creating an entrapment gap, or can allow the rails to fall off the bed completely.
Image illustrating case study 4
{kind=link}
Advice
Check the compatibility of any installed equipment and that all these devices are fitted correctly.
Use with children and adults with atypical anatomy
The majority of bed rails on the market are designed to be used only with individuals over 1.46m in height (4 feet 9 inches), which is the height of an average 12-year-old child. A risk assessment should always be carried out on the suitability of the bed rail for the individual child or adult with atypical anatomy, as bar spacing and other gaps will need to be reduced.
When purchasing or making assessments of bed rails for children or adults with atypical anatomy, seek guidance on suitable rails from the manufacturers and assess their compatibility with the size of the individual and the specific circumstances of use. A standard for medical beds for use with children was published in 2017 footnote 4. Older beds may not comply with this standard, and so may have larger gaps which are inappropriate for use with children and small adults (See section Standards). This should be considered as part of the risk assessment.
We recommend that all gaps between the rail bars should be a maximum of 60mm.
Case study 5: insufficient risk assessment which failed to account for the user’s body size
A bed rail was supplied to the parents of a child being cared for in the community. No assessment of the child’s physical size was carried out to determine if an entrapment hazard existed. In this case the gap between the horizontal bars of the bed rail was too large. The child slipped between the bars and asphyxiated as a result of head entrapment.
Image illustrating case study 5
{kind=link}
Advice
Risk assessments should include an evaluation of the suitability of the equipment for the physical characteristics of the intended user. These may need to be updated more regularly where the physical characteristics are changing, for example with growing children.
Adjusting or profile beds
Most adjustable and profiling beds feature integral bed rails that are incorporated into the bed design or are offered as an optional accessory by the bed manufacturer. We have found they are involved in far fewer adverse incidents than the third-party type. However, they can involve some hazards so should be used with caution too.
Some beds have a single-piece bed rail along each side of the bed. These require care in use because when the bed profile is adjusted entrapment hazards can be created. These are not always obvious when the bed is in the horizontal position.
Split bed rails (one pair at the head end and one pair at the foot end) also require care in use because the space between the head and foot end rails may vary according to the bed profile adjustment. Therefore, on some designs, entrapment hazards may be created when the bed is adjusted to profiles other than flat.
Use the rails as instructed by the bed manufacturer. The bed rails must be UKCA, CE or CE UKNI marked to show they meet the requirements of the Medical Devices Regulations 2002 footnote 3 or EU Medical Devices Regulation 2017/207 in combination with, or as an accessory to, the bed.
Bariatric beds
Bariatric beds allow the mattress base to be widened, however, when the bed is widened, the correct mattress for the bed size must be used. Using the incorrect mattress size could increase the risk of entrapment.
Active mattresses, hybrid mattresses and mattress overlays
Active, dynamic or hybrid mattresses or mattress overlays may be prescribed in order to reduce the risk of pressure injury. As these will raise the resting level of the user relative to the top of the bed rail, the effective height of the rail will be reduced. In turn this may increase the risk of the bed user falling from bed. Highly compressible surfaces may also create additional entrapment hazards.
The bed, mattress and rail system should be assessed in all configurations as these risks may not be obvious in a single arrangement. The risk assessment should consider the ‘worst case’ condition in particular: for example, the effective height of the top of the bed rail with the bed plus a fully inflated active mattress, or the highest point reached when an alternating cell mattress is used.
Before and during use of specialist mattresses with bed rails
Consider:
- the reduction in the effective height of the bed rail relative to the top of the mattress may allow the occupant to roll over the top of it - extra height bed rails may be required
- the risk of entrapment in the vertical gap between the side of the mattress and the bed rail may be increased with an easily compressible overlay and/or mattress edge
- if the standard mattress is replaced with an air mattress or lightweight foam mattress, third-party bed rail assemblies (including the mattress and bed occupant) can tip off the bed when the bed occupant rolls against the bed rail (this is because many third-party bed rails rely on the weight of a standard mattress to hold the assembly in place)
- the risk of the bed occupant rolling against the bed rail may be increased with lateral turning devices and this could lead to entrapment
Case study 6: bed occupant fell over the top of the bed rails after additional equipment installed
A pressure ulcer reduction overlay was added to a bed that already had a bed rail fitted. The additional height of the combined mattress/overlay reduced the height of the bed rail. The bed occupant fell over the rail, sustaining a serious head injury.
Image illustrating case study 6
{kind=link}
Advice
Risk assessments should be revised when substantial changes to the bed system are made. Pay particular attention when the effective height of the bed rail may be compromised.
Likewise, the use of patient turning systems for pressure relief carries similar risks of compatibility with other equipment in use and the patient themselves.
The risk assessment should consider the whole patient environment and possible interactions between any equipment that is in that environment.
Inflatable bed sides and bumpers
Typically, inflatable or padded bed sides cannot be adjusted and may require specific dimensions of a mattress and bed rails. It is therefore crucial to adhere to the manufacturer’s recommended size and specifications for the mattress and bed rails to prevent the creation of entrapment gaps and ensure stability. When evaluating the risk of entrapment, it is important to consider that inflatable rails may alter their shape when the bed occupant leans against them.
Some inflatable or padded bed sides house the mattress in its own ‘pocket’ or compartment, a feature which greatly reduces entrapment risks between the mattress and the side walls.
Inflatable bed sides need to be fully inflated to be effective. They may deflate over time so regular checks should be made to ensure this has not happened.
Care should be taken to use inflatable and padded bed sides correctly, as specified in the manufacturer’s instructions for use.
Bed rail bumpers, padded accessories or enveloping covers are primarily used to prevent impact injuries, but they can also reduce the potential for limb entrapment when securely affixed to the bed or rail according to the instructions for use. However, bumpers that can move or compress may themselves introduce entrapment risks. Care should be taken that the patient cannot remove these accessories. For example, a young child may not be able to undo attachments, but as the child grows, they may learn to detach them and this increases entrapment risks from the resulting gaps.
7. Maintenance
Ongoing use
Bed and bed rail devices may have a useful lifetime measured in years and might be used in various locations with many different bed occupants. Manufacturers should specify how devices should be used, cleaned and maintained and how long they can be used for so that they remain in good working order and continue to be safe to use.
Maintenance
MHRA adverse incident investigations have confirmed that some incidents with bed rails have been caused by inadequate maintenance. Bed rails should be included in planned preventative maintenance schemes.
Bed rails should be maintained in accordance with the manufacturer’s recommendations in the instructions for use. Examples of common types of damage include:
- adjusters, clamps and fixings that can wear, work loose, crack, deform, bend or even be missing completely - these issues can result in unintended movement, potentially leading to significant gaps
- bed rails that may weaken over time, especially when bed occupants frequently shake or rattle them
- telescopic components that can become loose or jammed, making it difficult to adjust them properly
- plastic components that can degrade due to factors such as ageing, exposure to light and some cleaning chemicals
- components that may suffer damage due to poor transport and storage practices
To thoroughly inspect these areas, it may be necessary to remove duvets, blankets, sheets and valances.
Bed rail assemblies should be traceable, for example by using the manufacturer’s serial number, the Unique Device Identification number (when available) or labelling with an in-house numbering system. This will assist in ensuring that every device is regularly inspected and maintained in a satisfactory condition. Traceability also allows devices to be suitably identified should a safety issue arise, such as a manufacturer recall due to a fault. Records should be kept of inspections, repairs and maintenance completed on bed rails. Contact the suppliers of the bed rails for advice and replacement parts.
Bed rails found to be unsuitable or in poor condition should be withdrawn from use and appropriately destroyed. We have received incident reports of bed rails being introduced back into use when they have been kept or stored. Manufacturers should be able to advise on the expected working life of their products.
When not in use, bed rails should be stored in matched pairs in a suitable area where they will not get damaged.
Case study 7: bed rails in poor condition from lack of maintenance
A care home had fitted third-party bed rails to a resident’s divan bed. One of the bed rails moved away from the side of the bed, creating a gap in which the resident became trapped and died as a result.
Bed rails in poor condition from lack of maintenance (Side of bed)
{kind=link}
On inspection, the locking mechanism to secure the bed rails against the sides of the bed (under the mattress) was missing.
Bed rails in poor condition from lack of maintenance (Under mattress)
{kind=link}
Advice
This incident could have been prevented if appropriate installation and maintenance checks had been in place, and if users were more aware of the correct configuration of the device.
Follow the instructions for use supplied by the manufacturer. Typical aspects to check during planned maintenance include:
- that the most up to date version of the instructions for use is being followed, as these may change during the lifetime of the device – these can be requested from the manufacturer, or are often available on the manufacturer’s website
- presence of rust – this can affect the ease of adjustability of telescopic tubes
- welded joints are sound, not showing signs of cracking or failure
- cracking of paint or coating – can point to deeper structural failure
- flaking or peeling chrome plating – can cause lacerations
- missing locking handles and fixing clamps, clamp pads and other components
- loose fixings – these affect the rigidity of the assembly (nuts should be of the self-locking type)
- free movement in joints – this can point towards loose, worn or incompatible components
- stripped threads on bed frame clamps – does not allow them to be tightened securely
- bent or distorted components
- damaged plastic components
- intact labelling and if the instructions for use have been updated, the updated version should be provided to the bed occupant and/or their carers
The frequency of inspection should be addressed by local policy, specific to the conditions of use and the recommendations in the manufacturer’s instructions for use. Defective devices should be withdrawn and replaced, if appropriate, quickly.
For more information on this topic, refer to Managing medical devices footnote 5.
8. Legislation and standards
Medical devices legislation in Great Britain and Northern Ireland
The MHRA is responsible for regulating the UK medical devices market. The Medical Devices Regulations 2002 are the principal regulations governing the law on medical devices in Great Britain. In Northern Ireland, the EU Medical Devices Regulation 2017/245 (‘EUMDR’) is directly applicable, and the Medical Devices (Northern Ireland Protocol) Regulations 2021 also make supplementary provision to support the implementation of EUMDR.
If a manufacturer wishes to market a medical device, the device must bear a mark: currently in Great Britain this can either be a UKCA mark or a CE mark, and in Northern Ireland this is a CE mark. A device may only bear these marks if the manufacturer fulfils certain obligations (conformity assessment).
These obligations include making sure that:
- the design of equipment is suitable for the product’s intended purpose
- the device is labelled appropriately and is supplied with instructions for use (where these are necessary for the safe use of the device)
- manufacturers have a quality management system
- manufacturers maintain suitable post-market surveillance of devices
Not all beds or fall protection equipment will be classed as medical devices. This depends on the intended use described by the manufacturer and without a clear medical purpose the definition of a medical device may not be met. In these cases, the product should still meet the requirements imposed by the General Product Safety Regulations 2005.
There is further guidance on the regulations footnote 6 and transitional arrangements footnote 7 on our website.
Health and Safety at Work Act 1974
People responsible for making decisions on the provision of bed rails and the care of people for whom they have been provided need to be aware of their duties under relevant health and safety legislation. These are enforced by the Health and Safety Executive (HSE) and Local authorities. For more information, visit the HSE website.
The Health and Safety at Work Act 1974 footnote 8 places duties on:
-
employers and self-employed people to protect the health and safety of people who might be affected by their work activities - they must do whatever is reasonably practicable to achieve this
-
employees to take reasonable care for the health and safety of themselves and others affected by their acts, and to co-operate with their employer on health and safety obligations
Health and Social Care Act 2008 (Regulated Activities) Regulations 2014: Regulation 12
The intention of this regulation footnote 9 is to prevent people from receiving unsafe care and treatment and prevent avoidable harm or risk of harm. Providers must assess the risks to people’s health and safety during any care or treatment and make sure that staff have the qualifications, competence, skills and experience to keep people safe.
Providers must make sure that the premises and any equipment used is safe and where applicable, available in sufficient quantities.
The Care Quality Commission has ‘Learning from safety incidents’ resources specifically related to bed rails. Each one briefly describes a critical issue: what happened, what CQC and the provider have done about it, and the steps you can take to avoid it happening in your service.
The Management of Health and Safety at Work Regulations 1999
The Management of Health and Safety at Work Regulations 1999 footnote 10 require that employers and the self-employed should make assessments of risk to the health and safety of their workforce and of people not in their employment, and to act upon risks they identify so as to reduce them.
Employers also need to ensure that all employees who are responsible for selecting, fitting, maintaining and checking bed rails have received adequate and appropriate training.
Mental Capacity Act 2005
The Mental Capacity Act 2005 footnote 11 or Adults with Incapacity (Scotland) Act 2000 footnote 12 protect those who may not be able to make decisions about their own care and treatment. When assessing whether a patient who lacks capacity may benefit from the use of bed rails, the views of the patient should be taken into account whenever possible.
All care professionals should understand their obligations under this legislation, and organisations should ensure that these requirements can be implemented effectively.
Standards
Manufacturers may opt to demonstrate compliance with aspects of the UK Medical Devices Regulations 2002 by making sure their products meet designated standards. When purchasing or specifying equipment, you should confirm what technical standards are met by the device. This should be available either in the device instructions for use or from the manufacturer themselves.
The current designated medical bed standard is:
BS EN 60601-2-52: 2010+A1:2015 “Particular requirements for the basic safety and essential performance of medical beds”.
This standard contains requirements for the dimensions and function of medical beds intended for adults and includes information on the permissible gaps between rails and the rails and the bed frame.
A separate standard has now been published that covers beds intended for use with children (and others of small stature):
BS EN 50637:2017 “Medical electrical equipment. Particular requirements for the basic safety and essential performance of medical beds for children”.
Standards such as these are primarily intended for manufacturers to demonstrate that the products they supply are suitable to be UKCA, CE or CE UKNI marked and placed on the market. The dimensions and measurements that they specify may not be appropriate to conduct in a clinical environment (for example requiring the use of tools with precise dimensions and mass) and may not assure safety if they are uncritically applied to all bed users.
Previous medical bed standards were largely replaced by BS EN 60601-2-52, but older beds may have been assessed against these earlier standards. Previous standards include:
BS EN 1970:2000 “Adjustable beds for disabled persons”.
BS EN 60601-2-38:1997 Revision 1 “Medical Electrical Equipment – Part 2. Particular requirements for the safety of electrically operated hospital beds”.
9. Adverse Incidents
An adverse incident is an event that causes, or has the potential to cause, unexpected or unwanted effects involving the safety of device users (including patients) or other persons.
Adverse incidents can be caused by:
- shortcomings in the device itself
- inadequate instructions for use
- insufficient servicing and maintenance
- locally initiated modifications or adjustments
- inappropriate user practices, including inadequate training
- inappropriate management procedures
- the environment in which devices are used or stored
- provision of bed rails which are unsuitable for the bed occupant
We strongly encourage everybody (patients/users/carers) to report all suspected adverse incidents to us. By reporting to us we can:
- collate information to identify trends in device safety and performance
- disseminate advice to the healthcare professions to prevent adverse incidents and promote good practice for use and maintenance of devices
Who to report to
If you are member of the public and live in England, Scotland, Wales, or Northern Ireland you should report adverse incidents via the MHRA Yellow Card scheme.
Healthcare professionals in England can report adverse incidents or near misses via the Yellow Card system.
Professional users in Wales, Scotland and Northern Ireland should report via their local incident reporting system and/or their national incident reporting authority.
You can find more information on our Report a problem with a medicine or medical device page
10. References and bibliography
References
- Never Events list 2018. London; 2018
- NHS Guidance on the Mental Capacity Act
- The Medical Devices Regulations 2002
- BS EN 50637:2017 “Medical electrical equipment. Particular requirements for the basic safety and essential performance of medical beds for children”
- MHRA. Managing Medical Devices. London; 2015.
- Regulating medical devices in the UK
- Implementation of the future Regulations
- Health and Safety at Work etc. Act. 1974
- Health and Social Care Act 2008 (Regulated Activities) Regulations 2014: Regulation 12
- The Management of Health and Safety at Work Regulations 1999
- Mental Capacity Act. 2005
- Adults with incapacity (Scotland) Act 2000
Bibliography
Haugh J, and others. High frequency of potential entrapment gaps in beds in an acute hospital. Age Ageing 2014; volume 43: pages 862 to 865.
Anderson Oand others. Interventions designed to prevent healthcare bed-related injuries in patients. Cochrane Database Syst Rev. 2012;(1).
Healey FM, and others. Bedrail use in English and Welsh hospitals. J Am Geriatr Soc, 2009; volume 57: pages 1887 to 1891.
Healey FM, and others. The effect of bedrails on falls and injury: A systematic review of clinical studies. Age Ageing. 2008; volume 37: pages 368 to 378.
NPSA. Bedrails; reviewing the evidence; a systematic literature review. 2007.
Appendix
Appendix 1: Adult entrapment risk assessment checklist
Example adult entrapment risk assessment checklist.
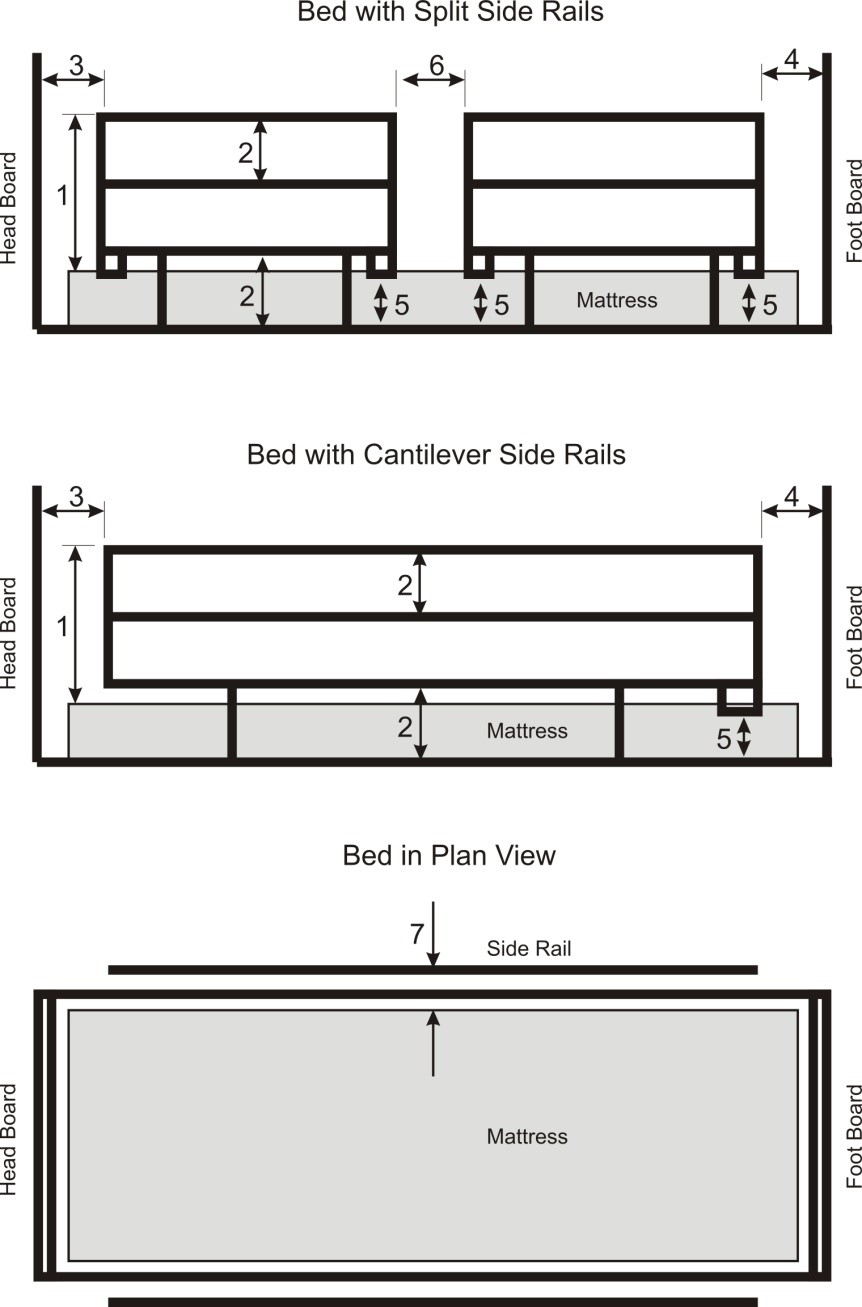
Appendix 2: Bed rail dimensions in BS EN 60601-2-52:2010+A1:2015 Medical Electrical Equipment. Particular requirements for basic safety and essential performance of medical beds
| Description | Diagram Reference | BS EN 60601-2-52:2010 | Notes |
|---|---|---|---|
| Height of the top edge of the side rail above the mattress without compression | 1 | ≥ 220mm | Where a speciality mattress or mattress overlay is used and the side rail does not meet ≥ 220mm a risk assessment shall be performed to assure equivalent safety |
| Gaps between elements within the perimeter of the side rail and between the side rail and mattress platform | 2 | < 120mm | |
| Gap between headboard and end of side rail | 3 | < 60mm | Most disadvantageous angle between headboard and side rail |
| Gap between foot board and end of side rail | 4 | < 60mm OR > 318mm | Most disadvantageous angle between foot board and side rail |
| Distance between open end of side rail(s) and mattress platform | 5 | < 60mm | The gap between the open end of the side rail and headboard is not relevant to this position reference |
| Gap between split side rails | 6 | < 60mm OR > 318mm | When in most disadvantageous position |
| Gap between side rail and mattress in ‘plan’ elevation | 7 | Perform test | 120mm aluminium cone is positioned between mattress and side rail to determine if gap is acceptable or not. |
Note that compliance to this standard requires the use of specific measurement tools, rather than basic distance measurements alone. It is intended to be used by manufacturers. For this reason, we recommend that end users do not use these measurements as the sole basis for evaluating suitability of a bed rail installation.
{kind=link}
Appendix 3: Bed Rail Dimensions in BS EN 50637:2017 Medical electrical equipment. Particular requirements for the basic safety and essential performance of medical beds for children.
| Description | Diagram Reference | BS EN 50637:2017 | Notes |
|---|---|---|---|
| Fully enclosed openings within a side rail, head/foot board, mattress support platform | A1 | <60mm | |
| Fully enclosed opening defined by the side rail, its supports and the mattress support platform | A2 | <60mm | |
| Partially enclosed opening defined by the head board, mattress support platform and side rail | A3 | <60mm | |
| Partially enclosed opening defined by the foot board, mattress support platform and side rail | A4 | <60mm | Except when gap between side rail and foot board is >300mm |
| Partially enclosed opening between segmented or split side rail and the mattress support | A5 | <60mm | Except when gap between side rails is >300mm |
| Partially enclosed opening defined by lowest point of a side rail, the adjacent side rail support and mattress support platform, to the outside of the side rail supports | A6 | <60mm | |
| Other openings defined by accessories (e.g. IV poles, fracture frames) and side rails, head or foot boards and or mattress support platform. Not shown in figures. | A | <60mm | |
| Distance between mattress support platform and the lowest point of the side rail outside the side rail support AND the angle between the side rail and mattress support platform at the range of the mattress height defined by the manufacturer ± 2 cm | B | <40mm AND angle between mattress support platform and side rail interface >75° over the entire range of mattress heights from minimum recommended height minus 2 cm to the maximum recommended mattress height plus 2cm. | |
| Gap between head board and adjacent side rail | C1 | <40mm | |
| Gap between segmented or split side rails with both side rails raised | C2 | <40mm OR >300mm | For a gap >300mm: the gap shall be >300mm or <400mm for the entire vertical distance |
| For all medical beds except junior beds: gap between side rail and foot board. Other openings defined by accessories (e.g. IV poles, fracture frames etc.) and side rails, head board, foot board, and or mattress platform | C3 | <40mm | |
| For junior beds: gap between side rail and foot board. Other openings defined by accessories (e.g. IV poles, fracture frames etc.) and side rails, head board, foot board, and or mattress platform | C4 | <40mm OR >300mm | For a gap >300mm: the gap shall be >300mm or <400mm for the entire vertical distance |
| Region defined by side rail/head board/foot board and the mattress for cribs and cots | D1 | Perform test | Cone tool does not sink below the mattress surface by 50% or more of its 60mm diameter. |
| Region defined by the side rail/head/foot board and the mattress for junior beds and oversize cots | D2 | Perform test OR gap between side rail/head/foot board and mattress <30mm | Cone tool does not sink below the mattress surface by 50% or more of its 60mm diameter. |
Note that 50637:2017 defines different sized beds: cots, oversized cots, cribs and junior beds. See the text of the standard for full definitions or contact the manufacturer of a particular bed in your control that complies with this standard.
Compliance to this standard requires the use of specific measurement tools, rather than basic distance measurements alone. It is intended to be used by manufacturers. For this reason, we recommend that end users do not use these measurements as the sole basis for evaluating suitability of a bed rail installation.
{kind=link}
Updates to this page
-
Guidance updated to reflect: • The need for risk assessments to be updated regularly. The frequency of reviewing the risk assessment will vary depending on the patient and their circumstances and should be recorded as part of the risk assessment, but will likely be more frequent for children. • The entrapment risks that trolleys with side rails share with medical beds. • Additional risks relating to bariatric beds and lateral turning devices. • The differences between bed rails and bed grab handles and the risks if they are used incorrectly. • Involving the patient and/or their family or carers in the decision to use bed rails. • Ensuring that the most up-to-date version of the instructions for use are being used and are provided to the bed occupant and/or their family and carers. The case studies have not been updated
-
This guidance has been updated now that the Government has made regulations that enable CE marked medical devices to continue to be accepted in Great Britain for defined periods beyond 30 June 2023.
-
Paragraph added to the summary section which explains that the government intends to extend acceptance of CE marked devices in Great Britain beyond 30 June 2023.
-
New version of the 'Safe use of bed rails' PDF attached
-
This has been updated due to the end of the Brexit transition period.
-
First published.